


Rare pituitary diseases in dogs and cats and their human companions
 0
0 Abstract
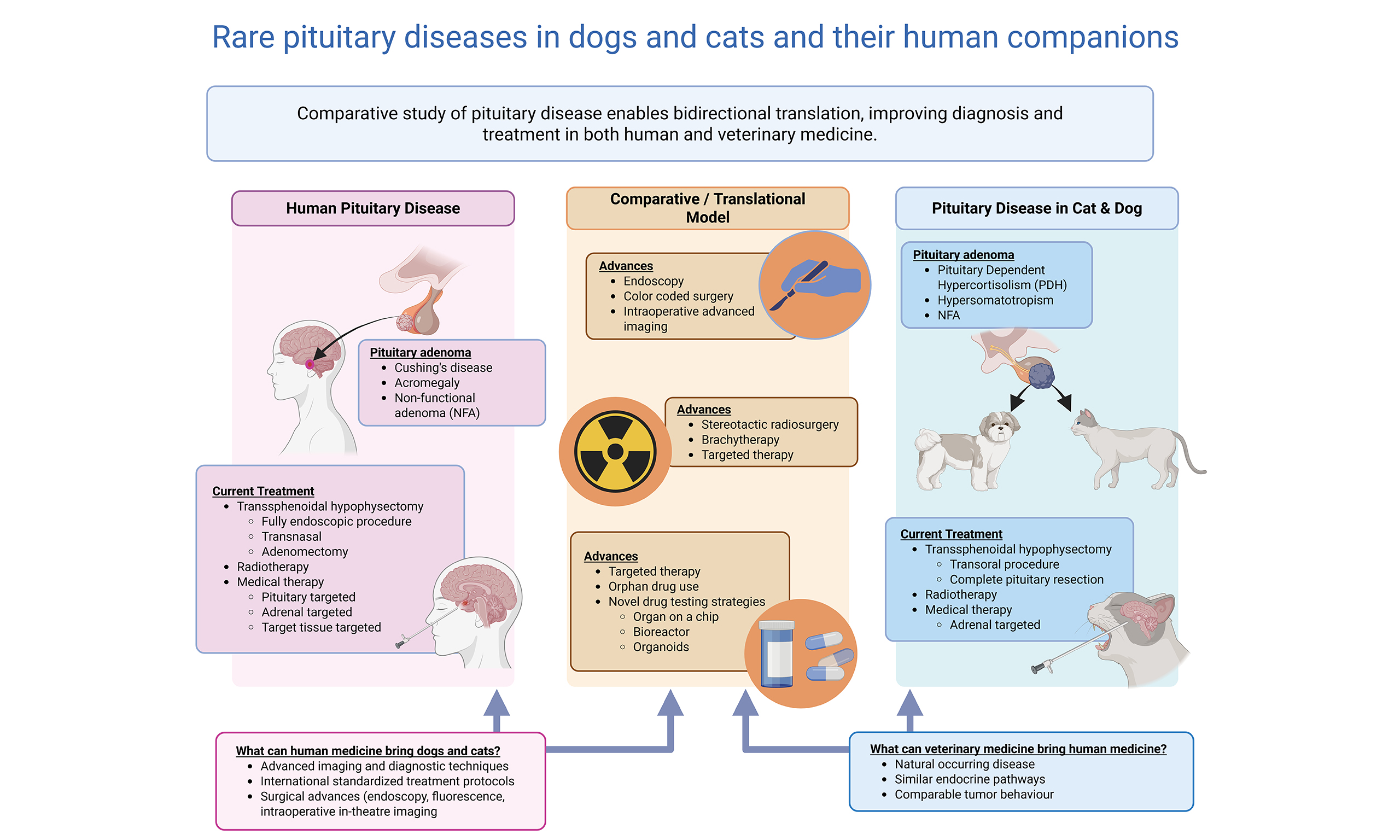
The pituitary gland, though small in size, has been recognized for its essential functions since the early 20th century. Dogs played a pivotal role in understanding its endocrine function, and the history of hypophysectomy in humans and dogs is strongly interrelated. While pituitary diseases are rare in humans, they are more prevalent in dogs and cats, with neoplasia representing the most common pathology. These tumors can lead to endocrine disorders such as Cushing’s disease and acromegaly across species. The classification of diverse pituitary adenomas in humans, has prompted their investigation in veterinary patients and the advances in surgical and medical management of pituitary disease exemplify translational medicine. Techniques developed for humans, first evaluated in experimental dogs and subsequently translated into veterinary clinical practice. In the search for novel medical treatment strategies against pituitary diseases in humans, animal studies investigating the feasibility and safety of orphan drugs in large animal models like dogs and cats with spontaneous disease offer valuable information for the initiation of clinical trials in humans. While the incidence of particular pathologies differs between species, there is a common goal for all patients: refining treatment and improving outcomes. This review discusses current status and developments in treatment options for pituitary tumors in companion animals, and takes a look over the shoulder of our human counterparts to see which current, novel and future practices may be promising for our veterinary patients, and investigate how trials with orphan drugs against pituitary disease in veterinary patients can favor human clinical trials.
Keywords
INTRODUCTION
While dogs and cats share many endocrine disorders with humans, their spontaneous pituitary diseases offer unique opportunities for translational research, bridging the gap between experimental models and clinical practice. Conversely, the progress made in human medicine, particularly in data collection and international collaboration between neuroendocrine pituitary disease treatment centers, may benefit companion animals through the translation of advances in modern human medicine.
The pituitary gland is a central regulator of endocrine function, composed of an anterior lobe (adenohypophysis), posterior lobe (neurohypophysis), and pars intermedia [Figure 1][1,2]. Where the human pituitary has a distinct bilobed appearance [Figure 1A][2], the pituitary gland of dogs and cats has a more rounded shape, where the adenohypophysis encases the neurohypophysis and pars intermedia [Figure 1B][1]. The anterior lobe secretes adrenocorticotropin (ACTH), growth hormone (GH), luteinizing hormone (LH), follicle stimulating hormone (FSH), prolactin (PRL), alpha-melanocyte stimulating hormone (α-MSH), and thyrotropin (TSH), while the posterior lobe releases arginine-vasopressin (AVP) and oxytocin, produced in the hypothalamus and transported via axons to the posterior lobe[1,2]. The pars intermedia produces ACTH and α-MSH[1]. Each region maintains specific hormonal balances within a feedback system linking the pituitary and target glands [Figure 2][1,2].
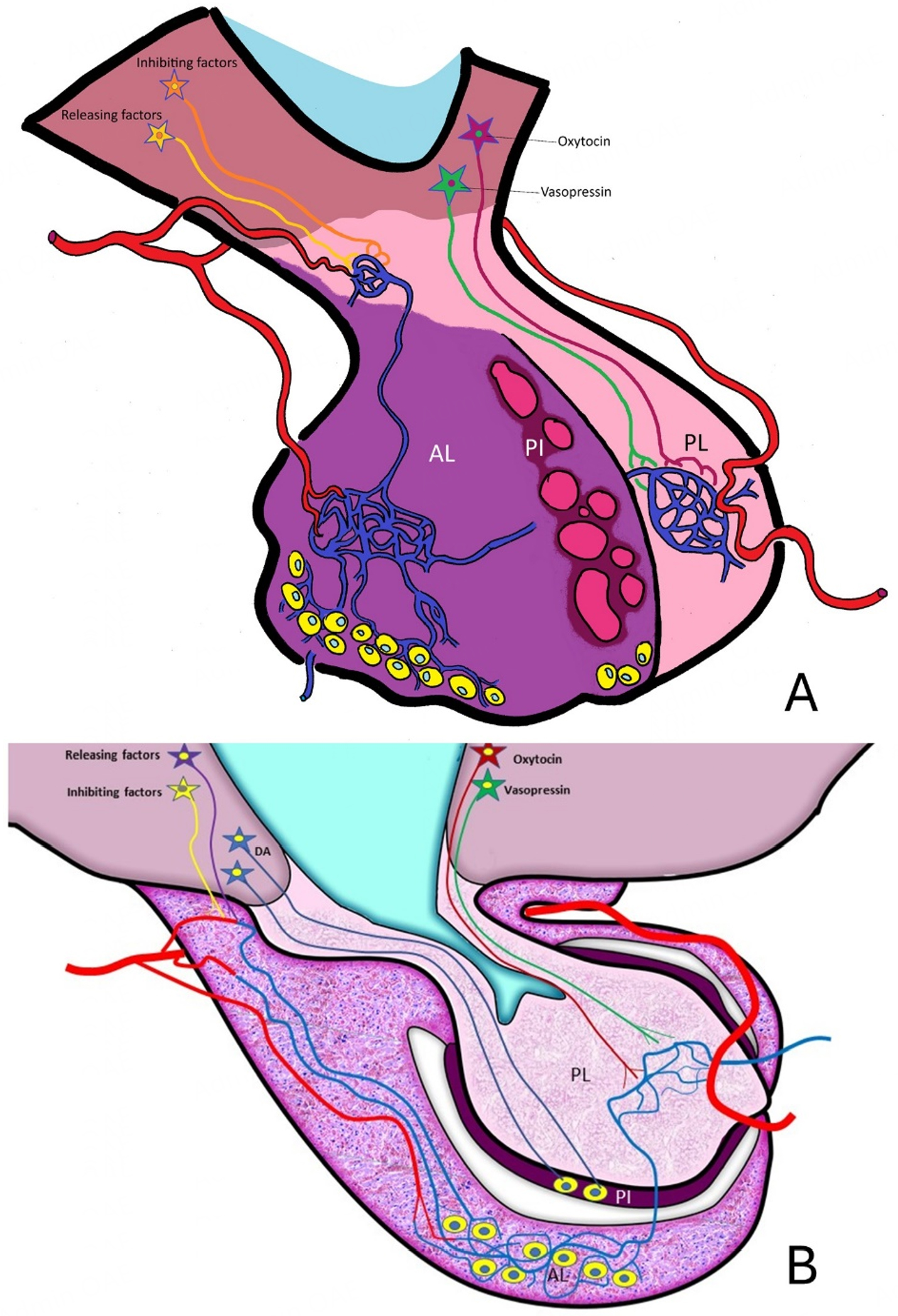
Figure 1. The pituitary gland of the human (A) and the dog (B). A schematic interpretation of the differences in anatomy between the human and the dog. The hypothalamus indirectly communicates with the anterior lobe (AL) through releasing and inhibiting factors that reach the anterior lobe through the capillary pituitary portal system. The posterior lobe (PL) is a downward projection of the ventral hypothalamus. Neurohypophyseal hormones (oxytocin and vasopressin) are produced within supraoptic and paraventricular nuclei in the hypothalamus from which axons extend through the pituitary stalk to the posterior pituitary lobe. The pars intermedia (PI) is under direct neurotransmitter control in the dog and cat, but is mostly inactive in humans, with its original cells dispersed throughout the anterior lobe. (Adapted from Rijnberk and Kooistra, 2010[2]. Written permission for use and adaptation of copyrighted material was obtained from the copyright holder. Figures were prepared using Microsoft Paint (version 11; Microsoft Corporation, Redmond, WA, USA)).
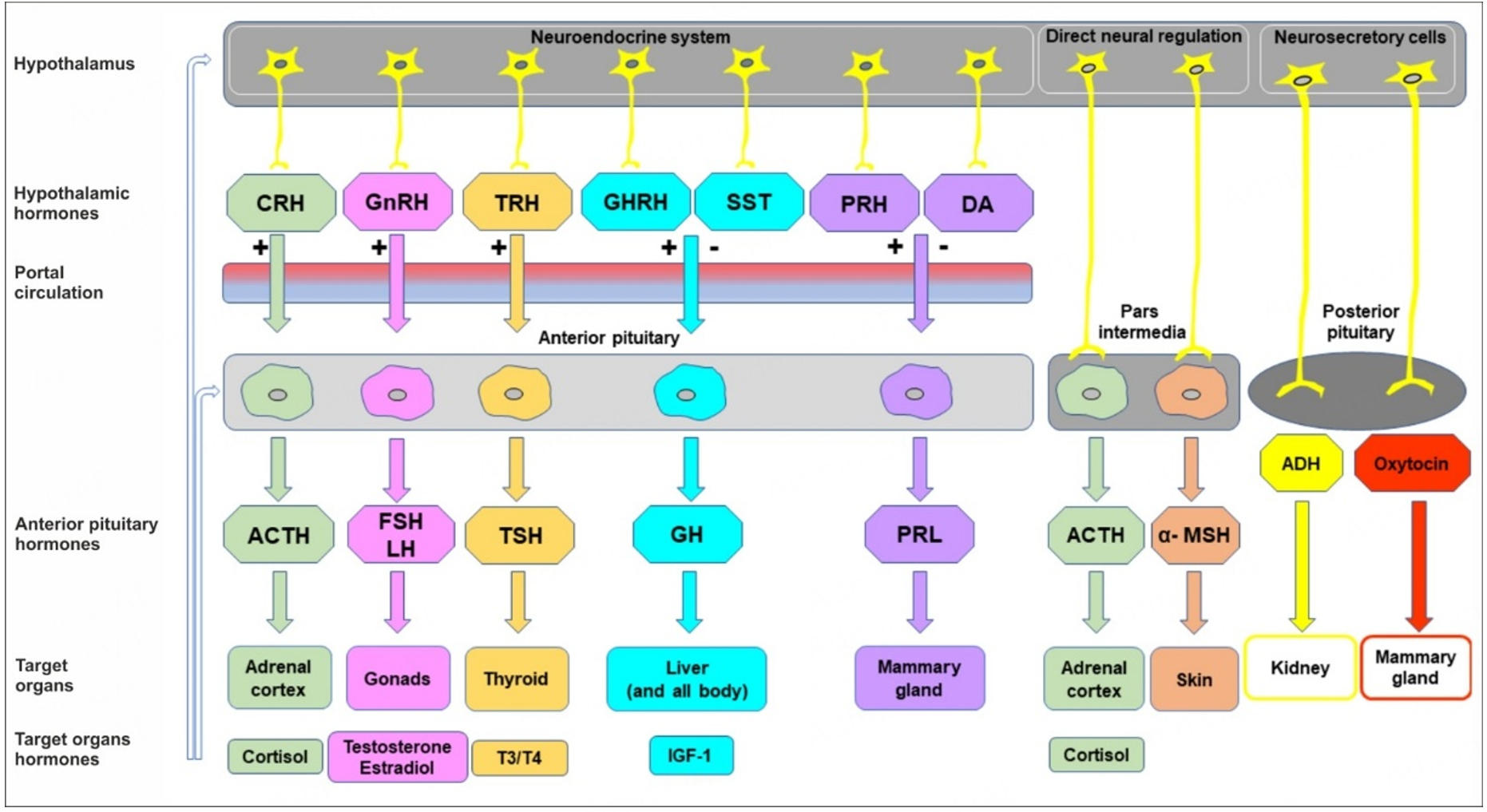
Figure 2. A simplified diagram of the three mechanisms (neuroendocrine system in the anterior pituitary, direct neuronal regulation of the pars intermedia, and neurosecretory cells in the posterior lobe) that regulate the secretion of the hormones in the pituitary gland. Adrenocorticotropic hormone (ACTH), antidiuretic hormone (ADH) or vasopressin, corticotropin-releasing factor (CRH), dopamine (DA), follicle-stimulating hormone (FSH), growth hormone (GH), growth hormone-releasing hormone (GHRH), gonadotropin-releasing hormone (GnRH), insulin-like growth factor 1 (IGF-1), luteinizing hormone (LH), alpha-melanocyte-stimulating hormone (α-MSH), prolactin (PRL), somatostatin (SST), thyrotropin-releasing hormone (TRH), thyroid-stimulating hormone (TSH), tri-iodothyronine (T3), tetraiodothyronine (T4), stimulation (+), inhibition (-). [Adapted from Rijnberk and Kooistra, 2010[2]. Written permission for use and adaptation of copyrighted material was obtained from the copyright holder. Figures were prepared using Microsoft Paint (version 11; Microsoft Corporation, Redmond, WA, USA)].
Pituitary disease divides into endocrinopathies (e.g., ACTH- and GH-producing tumors) and non-functional lesions. Clinical signs reflect hormonal excess or neurological compromise. Endocrinopathies may involve hormone hyper- or hypofunction[3-6], whereas non-functional pathologies, including cysts[7,8], silent/non-functional adenomas[9-12], craniopharyngiomas[13], hypophysitis[14,15], apoplexy[16-19] and rare pathologies like granular cell tumors[20], ganglioglioma[21], and metastases from (endocrine) carcinomas[22-26], often present with neurological signs[27] [Table 1].
Common clinical signs/complaints
| Human | Dog | Cat | |
| PDH/CD | Redistribution and accumulation of fat in the face (moon face), upper back (buffalo hump) and abdomen Thin, fragile skin Hypertension Muscle weakness Hirsutism | PU/PD Polyphagia Abdominal distension Panting Alopecia Calcinosis cutis Centripetal fat redistribution Thin, fragile skin Muscle wasting Joint laxity/arthropathy | PU/PD Thin, fragile skin (feline fragile skin syndrome) Centripetal fat redistribution Abdominal distention Polyphagia Obesity |
| HS/acromegaly | Acromegaly Obesity Hypertension Prognathism Hypopituitarism Sleep apnea | Very rare Acromegaly Abdominal organomegaly Prognathism Obesity | PU/PD Polyphagia Acromegaly (not always clinically evident) Arthropathy Abdominal organomegaly Cardiovascular disease Obesity |
| NFA | Visual impairment Headache Hypopituitarism In severe cases, central neurological signs | Central neurological signs (head pressing, circling, decreased mentation, blindness, epilepsy) | Central neurological signs (head pressing, circling, decreased mentation, blindness, epilepsy) |
Clinical presentation in non-functional sellar masses differs between humans and small animals: humans commonly report visual deficits and headaches early[28], while dogs and cats are typically diagnosed only after overt neurological changes such as seizures or altered behavior[18,27,29]. Anatomical variation explains this. In humans, the pituitary fossa is covered with the diaphragma sellae at the dorsal rim. This diaphragm consists of a fold of dura mater, surrounding the pituitary stalk (infundibulum), and separates the extracranial pituitary gland from the intracranial components including the hypothalamus and optic chiasm[30,31]. The optic chiasm in humans overlies the diaphragma sellae in 80% of cases and is positioned approximately 1cm dorsal to the diaphragma sellae[30]. The pituitary tumor growth will start by dorsal compression of the diaphragma sellae, lifting the optic chiasm dorsally, causing visual impairment[31]. Due to the high dependence of visual function, patients will vocalize their visual impairment readily[30].
In dogs and cats, the optic chiasm is located rostrally from the tuberculum sellae, and with a lack of a rigid diaphragma sellae, the mass is more prone to expand dorsally before it expands rostrally, where the optic chiasm is located in these species. Visual impairment will only become evident once this is severe enough that it nears blindness and behavioral changes become evident to their owners[18,27,29]. Therefore, masses compromising eyesight in dogs and cats are relatively large on presentation, and visual impairment alone as a presenting clinical sign is relatively rare in dogs and cats[18,27,29].
Prevalence of pituitary pathologies also varies by species. Unlike in human medicine, the true prevalence of diseases in dogs and cats is not well documented. The underlying causes of illness in affected animals are often not investigated, and diagnoses may be missed. Furthermore, in most countries there is no standardized system for monitoring disease prevalence or recording causes of death. This issue is particularly pronounced in cats, for which disease data are poorly documented overall. Consequently, current published estimates of disease prevalence should be interpreted with caution. However, in the sparse literature available, in cats, somatotroph adenomas predominate (estimated prevalence 1/1.000-1/2.000), followed by corticotroph adenomas and non-functional masses[29,32]. An increase in recognition of underlying causes of diabetes mellitus in recent years and improved awareness in veterinary medicine has led to an increase in the diagnosis of hypersomatotropism (HS) in cats[29,32]. The marked acromegalic features observed in human patients are often not clinically evident in cats. This has led to the general adoption of the term HS rather than acromegaly when describing this condition in cats[32]. In dogs, corticotroph adenomas predominate (prevalence approximately 1/1.000 to 1/2.000), with rare cases of non-functional masses, somatotroph adenoma, prolactinoma, craniopharyngioma, or hypophysitis[14,15,22,32]. So far, TSH-, LH-, and FSH-producing tumors have not been reported in dogs and cats[4,33]. In humans, somatotroph adenomas (1/7.500-1/35.000), prolactinomas and non-functional (gonadotroph) adenomas are most common, while corticotroph adenomas are rare (approximately 1/500.000-1/800.000)[34-47].
Treatment strategies differ among species. In human medicine, therapy targets hyperfunction by selective adenomectomy, tumor mass reduction, radiotherapy, and pharmacological intervention[34-47]. Complete hypophysectomy, most commonly used in dogs and cats, is avoided due to quality-of-life concerns from hypopituitarism[48]. Species differences also modify the impact of FSH/LH depletion: loss of gonadal hormones in humans has great psychological and physical impact whereas gonadectomy in veterinary patients at an early stage in life is common practice and loss of FSH/LH appears to carry no consequences. Postoperative behavioral changes in animals may also reflect hormonal deficiencies, but have not been investigated.
For veterinary patients, the aim in Cushing’s disease (CD) [pituitary-dependent hypercortisolism (PDH)] is elimination of ACTH excess and restoration of normocortisolism[49,50]. In acromegaly/HS, therapy in all species, seeks to normalize GH/insulin-like growth factor 1 (IGF-1) levels, resolve secondary diabetes mellitus, and reduce morbidity. In non-functional pituitary adenomas, treatment goal is to eliminate or reduce the mass effect. In all cases, surgical excision not only removes the primary tumor, but also treats the mass effect caused by large pituitary adenomas. Surgical excision or radiotherapy can effectively address the cause of hormonal excess but has consequences. After surgery, hormone replacement therapy is needed, consisting of lifelong glucocorticoid and thyroid hormone supplementations, and temporary to lifelong ADH replacement[32]. Radiation therapy of the pituitary gland can lead to hypopituitarism[44,51] and replacement therapy may be necessary. On the other hand, adjuvant medical therapy is commonly needed following radiotherapy for functional adenomas to address persistent endocrine hyperfunction. In both veterinary and human medicine, surgery remains the primary treatment for acromegaly/HS and Cushing’s disease/PDH. In this manuscript, acromegaly and Cushing’s disease (CD) refer to the human condition, whereas HS and PDH are used to describe the corresponding disorders in dogs and cats.
SURGERY
The early days; experimental and translational pituitary surgery (late 1880s-1960)
The first experimental surgical approaches to the pituitary and pituitary fossa were performed by the end of the 19th century, as means to investigate the pituitary function[52,53]. Different animal species were subjected to numerous variants of surgical approaches in order to understand the function of the pituitary gland.
Going forward; 1960-now
By the late 1950s and early 1960s, surgeons in human medicine started implementing intraoperative imaging using fluoroscopy (1957), and introducing endoscopes (1961) and the operating microscope (1965)[53,63]. This created a significant step in refinement and accuracy of the surgical procedure. With improved understanding of functional anatomy, and advances in imaging through CT and MRI [Figure 3], visualization, and instrumentation in the decades that followed, human pituitary surgery evolved into a central therapy[34,40,53,63-68].
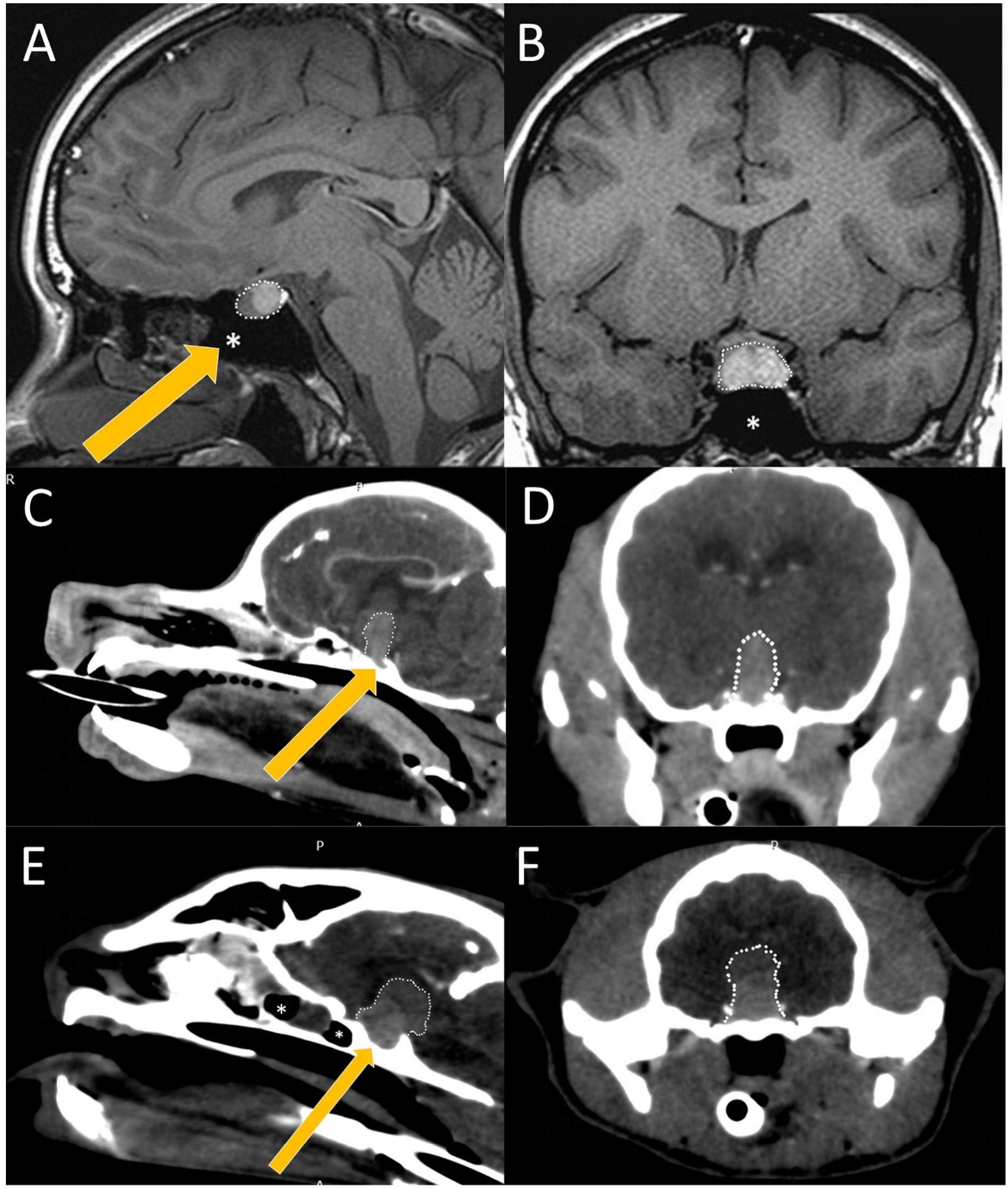
Figure 3. Radiographic anatomy of the pituitary in relation to the brain and skull of man (A and B), dog (C and D) and cat (E and F). All cases depicted, involve a large pituitary adenoma (white dotted outline). A midline sagittal (A, C, E) image at the level of the pituitary fossa and a transverse (B, D, F) image of all three species demonstrate the profound anatomical differences between the length of the maxilla and nasal bones. The presence of the large air-filled sphenoid sinus rostroventral to the pituitary fossa (white asterisk) is visible in the sagittal plane in man (A), is absent in the dog (C) and present in the cat (E), but in the cat located completely rostrally to the pituitary fossa. Mode of entrance is depicted with a yellow arrow. (Image rendering with RadiAnt DICOM Viewer, Medixant, van Stee L).
In veterinary medicine, clinical application of pituitary surgery lagged until the 1960s, with sparse reports until the 1990s when micro-neurosurgical adaptations, supported by advances in imaging, anesthesia and intensive care improved outcomes[69-74]. While nowadays transsphenoidal surgery is a standard therapy in humans, pituitary surgery is still limited to few veterinary centers globally[12,32,75].
Translational opportunities to improve outcome
Current state and recent improvements in technique
From early days in transsphenoidal surgery, anatomical variation between species forced surgeons to develop different surgical approaches to the pituitary fossa. Though techniques may differ, the importance of translational surgery remains. In humans, the short nasal length and relative large skull, combined with a large air-filled sinus rostral to the pituitary fossa, enables a full endoscopic procedure [Figure 3A]. Therefore, transsphenoidal surgery in humans has advanced to full endoscopic pituitary surgery through transnasal approaches[35-37,45,76-79], while temporal approaches are reserved for large masses[35,38,46].
Veterinary patients currently undergo a microsurgical transoral approach[32,70,71] since companion animal skull anatomy [Figures 3 and 4] overall lacks the space and large air-filled sinus that enables a transnasal endoscopic approach as used in human medicine. However, the implementation of telescopes in pituitary surgery in veterinary patients is increasingly investigated. Anatomical differences in dogs and cats [Figure 4] limit the full endoscopic adoption of human techniques but the endoscopic [Figure 5] and exoscopic visualization has improved outcomes and educational value also in dogs and cats[32,80-83]. Patient-specific 3D drill guides[84,85] and intraoperative neuronavigation[86,87] are emerging to improve accuracy of the surgical approach to the pituitary fossa.
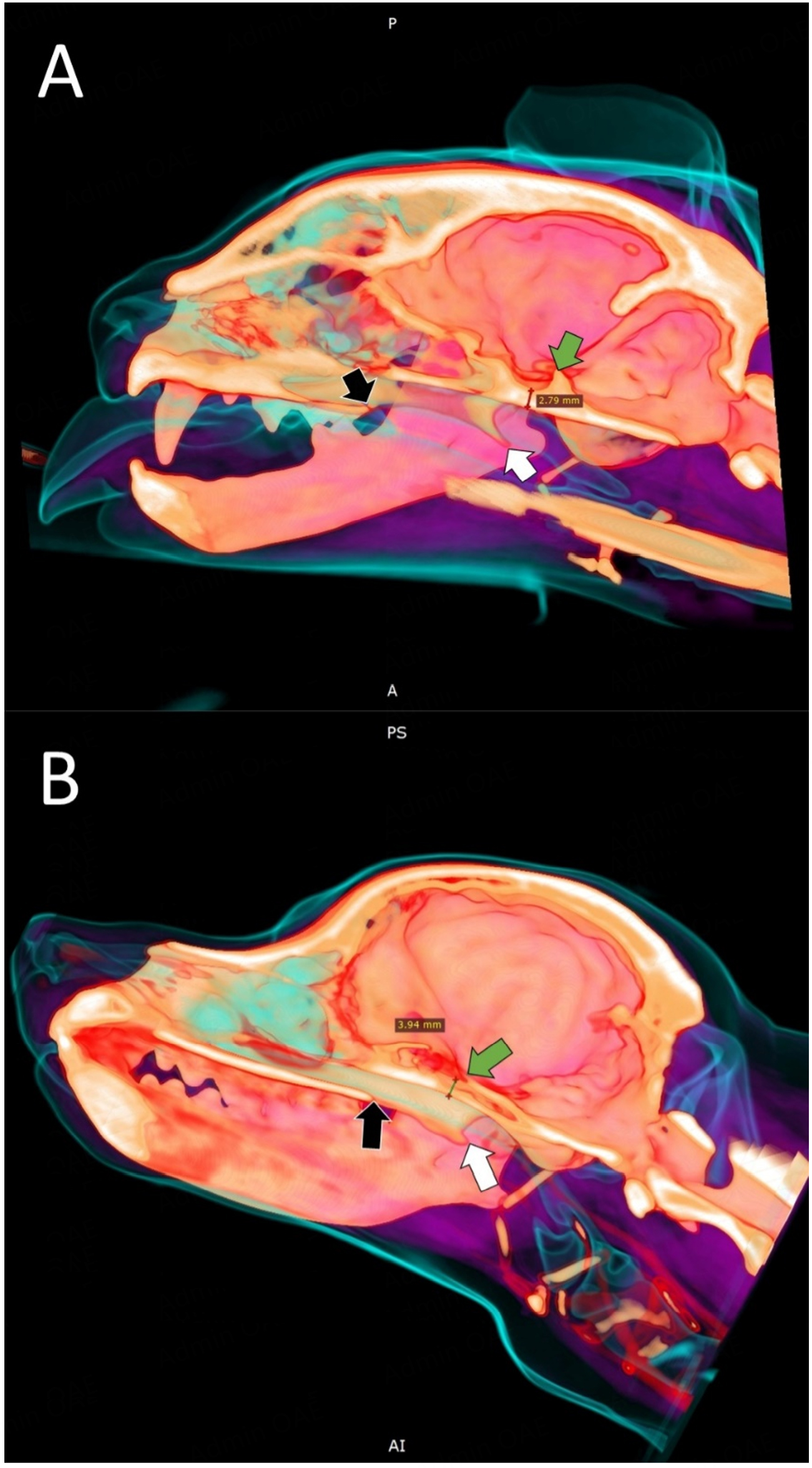
Figure 4. Sagittal 3D mock-up for in silico preparation of a transsphenoidal approach in a cat (A) and a dog (B). Anatomic landmarks for intraoperative identification of correct surgical positioning of the burr hole are marked with arrows. Green arrow: dorsum sellae. White arrow: hamular process of the pterygoid bone. Black arrow: caudal edge of the hard palate. Thickness of the sphenoid bone is measured at the deepest part of the pituitary fossa (red line in A, black line in B). (Image rendering with RadiAnt DICOM Viewer, Medixant, Courtesy van Stee L).
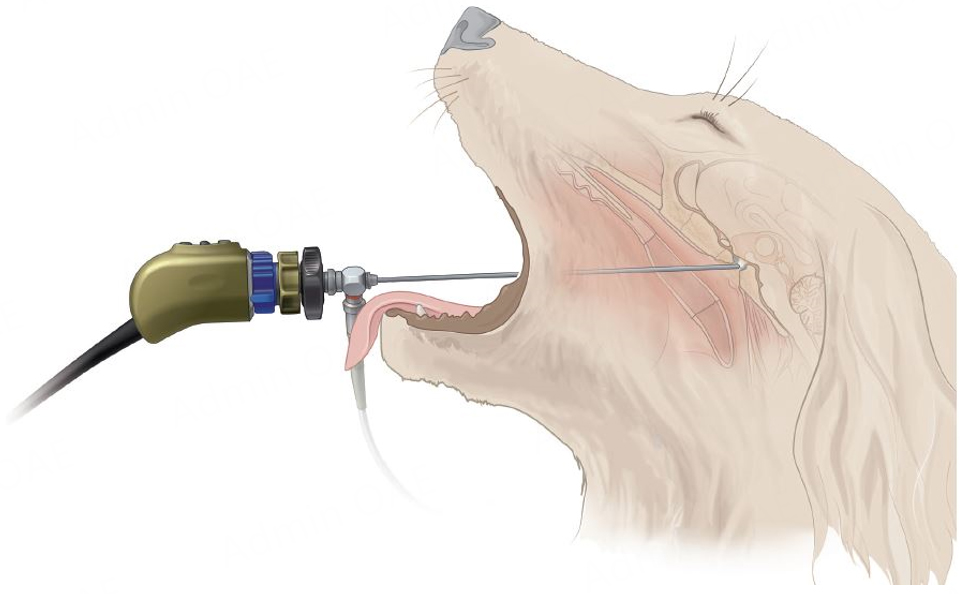
Figure 5. Fossa endoscopy in the dog and cat. A transoral approach is performed through the soft palate to reach the ventral aspect of the sphenoid bone. Following burring at the correct location, the pituitary mass is extracted from the fossa. A rigid angled telescope can be used to visualize and support the approach and course of hypophysectomy, and when introduced inside the fossa, to assess neural and vascular structures and completeness of tumor resection.
At this moment, the long term recurrence rate of PDH in dogs after curative intent transsphenoidal hypophysectomy is reported at 27% at a median time of 555 days post-surgery[88]. In that report, 306 dogs underwent a transsphenoidal hypophysectomy for PDH in a single institution[88]. The survival rate at four weeks after surgery was 91% with a 92% confirmed remission rate[88]. In human medicine, postoperative remission is reported to be around 70%-80% in expert centers, with a long term recurrence rate of
Surgical dexterity is also key in veterinary medicine, and a study on hypophysectomy in 306 dogs with PDH in a single institution reported long term follow up results with postoperative mortality rates and postoperative remission rates of 9% and 84%, respectively[88]. Remission rates after hypophysectomy increased over time, whereas tumor size measured as the P/B ratio at time of admission increased as well[88]. This may well be a reflection of an improved surgical dexterity. Studies in veterinary medicine describing long term outcome in large cohorts of HS or non-functional pituitary adenomas, are lacking due to their small numbers.
The improved outcomes after transsphenoidal hypophysectomy that are reported over the last decade, are likely to be caused by improved preoperative treatment and planning, improved dexterity during surgery and overall perioperative care and improved postoperative treatment and monitoring[32]. Postoperative management includes monitoring for changes in homeostasis that need addressing, and providing analgesia and anti-microbial prophylaxis, on top of hormone replacement therapy. Cases with severe preoperative neurological signs or cases that underwent a massive change in intracranial pressure during surgery, may need additional management. Overall, uncomplicated cases of dogs treated for PDH remain hospitalized at the intensive care unit (ICU) at a median of 2-3 days. Cats treated for HS and concomitant diabetes mellitus may need a longer hospital stay to stabilize their electrolyte and glucose homeostasis[94,95]. Complications occur and include upper respiratory complications (rhinitis, soft palate dehiscence) and ophthalmologic complications like keratoconjunctivitis sicca (KCS) and subsequent corneal damage are a direct result of the transsphenoidal surgery[32]. Aspiration pneumonia and serious central nervous system complications like Cushing reflex and altered mental status are also reported, but are less common to rare. Animals at increased risk of complications are brachycephalic dogs (upper and lower respiratory complications, palatal dehiscence, gastrointestinal), cats (dehiscence of soft palate, prolonged hospitalization, lifelong ADH replacement therapy), older animals with endocrine disease (KCS), and animals with very large masses (central nervous system complications and permanent ADH replacement therapy)[32,81,88,94,95]. Most complications are self-limiting or can be treated with little intervention[32].
Expanding our horizon in veterinary surgery
Ideally, the surgeon should be able to distinguish tumor tissue from normal tissue, and even differentiate between tumor types during surgery. Preoperative testing, imaging and functional testing alike, may not always give this information. Distinguishing between normal and diseased tissue is especially important in cases in which only the disease portion of the pituitary is to be removed - thus in the majority of human cases and the need for more reliable techniques is pressing further development[36,77,78,96,97].
Molecular imaging (positron emission tomography (PET)/CT, PET/MRI) is expanding in humans for perioperative tumor localization and postoperative assessment; veterinary applications remain limited[96,98-104]. Intraoperative MRI, image-guided surgery, and fluorescence-guided techniques improve precision in humans but are constrained in veterinary practice by cost, patient size and validation[96,105-108]. As an example, current telescopes that can detect indocyanine green fluorescence, measure at least 4.5 mm in diameter, while the sphenoidotomy performed in dogs and cats for pituitary extraction is often smaller in cross section. Intraoperative differentiation could be aided by local techniques like ultrasonography[96]. However, the limited spatial resolution and interpretation variability combined with the probe size make it less suitable for companion animals. Probing techniques that are aimed at tissue properties like elastography and spectroscopy may be promising for human cases where adenomectomy is performed, however, especially patient size and surgical aim exclude these refining technical options in dogs and cats[96].
Augmented and virtual reality[109-115], and 3D-printed training models[116-119], are being explored to refine surgical training and accuracy. As prices of 3D programs and printing have come down, in silico training programs and live-like models should become more available. If not only for training novice surgeons, both human and veterinary, it could enable dexterity training for trained surgeons without the ethical costs of in vivo and ex vivo training and without the price tag it once came with[118-119]. Artificial intelligence and machine learning show potential in predicting outcomes and optimizing therapies, and are already implemented in large studies in human medicine[97,120,121]. Large cohort studies are possible in medicine when humans patient numbers become large through international pituitary treatment center collaborations, exchanging patient data and implementing study protocols throughout the world[48,91,97,120,121]. In veterinary medicine, case numbers remain low with the few specialized animal hospitals available. Limited veterinary data remain a challenge for limited veterinary data remain a challenge for large data models large data models[121-124]. This represents a significant loss for both veterinary and human medicine. While human medicine may benefit from naturally occurring clinical models for the development of novel treatment strategies, dogs and cats suffering from pituitary disease could in turn benefit from additional therapeutic options that were previously unattainable.
While the different techniques described above may become implemented in transsphenoidal surgery in dogs and cats during the initial attempt to achieve surgical cure, there is a group of patients that will either not achieve remission, or suffer recurrence at one point in time. Sometimes, residual disease is left behind by choice, as part of a debulking strategy, and sometimes inadvertently. In the former case, there may already be a strategy for further adjuvant treatment, for example mass reduction prior to radiation therapy. Or, when complete excision in a single procedure is considered to be excessively risky. And thus, a second surgical intervention is planned for the future. In large masses, neoadjuvant radiotherapy may be an option too, where radiotherapy is used to decrease tumor size, aiding subsequent surgical extraction. In the latter case, recurrence eventually will become evident as the clinical signs the animal presented with initially, also recur. In functional tumors, functional testing on a regular basis may pick up on early recurrent disease[32]. In case of non-functional masses, regular advanced diagnostic imaging is advised[32]. In order to improve outcome assessment for veterinary pituitary disease patients, a protocolized workup, treatment and follow up akin to the consensus statements[36,48,91,93] in human medicine would be helpful[32]. In cases of recurrent disease, surgical intervention can, just like in human medicine[48,91,93] be a viable choice[5,8].
In cases in which transsphenoidal surgery fails, or recurrence develops over time, follow up treatment will greatly depend on the type of primary tumor. In case of a functional adenoma, treatment will be aimed at decreasing the clinical signs caused by the endocrinopathy. The first line of treatment will likely be medical, following the preferred pharmaceutical therapy at the moment. If a second surgical procedure is not advised or chosen, follow up radiation therapy may be offered to prevent further tumor mass increase and subsequent intracranial tumor mass effects. In case of a nonfunctional adenoma, treatment of recurrent disease will depend on clinical signs and mass effect. If a second surgical procedure is feasible, this may be preferred. However, in veterinary patients with very large masses, rapid and massive surgical decompression may lead to severe neurological deterioration. If surgery is necessary, but a complete resection is unsafe or unlikely to achieve, a surgical debulking procedure and postoperative radiation therapy may be the safest way[32]. If the patient’s condition facilitates radiation therapy alone, this may also be considered.
RADIOTHERAPY
If feasible, hypophysectomy is the primary treatment of choice for functional pituitary tumors, due to its high likelihood of inducing endocrine remission and its potential to be curative[82,88,95]. However, the limited number of specialized surgeons worldwide who have the expertise to perform hypophysectomy in dogs and cats significantly restricts access to this surgical option[32]. Consequently, radiation therapy (RT), which is more widely available, is frequently employed in the treatment of pituitary tumors in these species
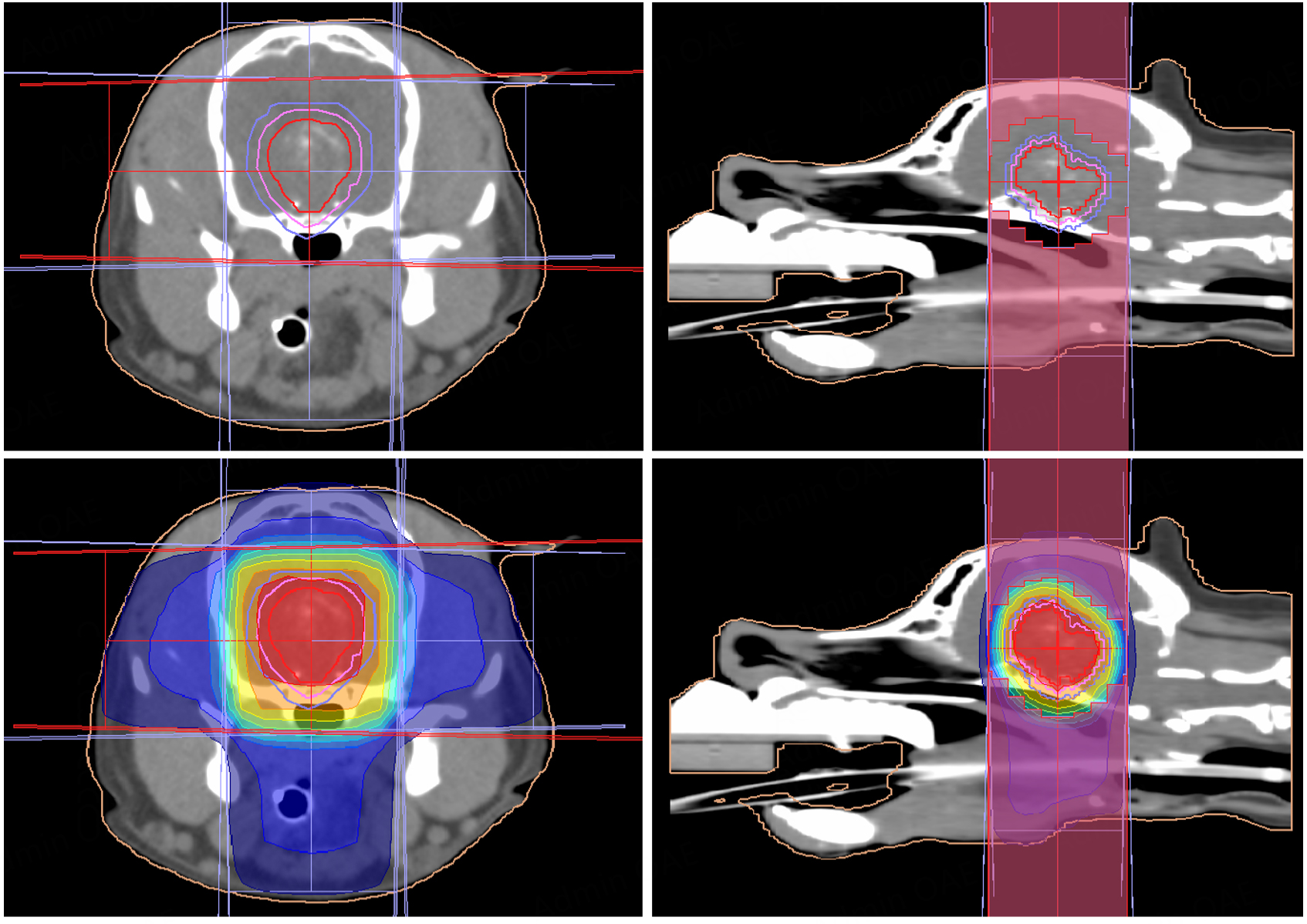
Figure 6. Four-field 3D conformal radiotherapy plan for a canine pituitary tumor. Axial and sagittal CT images show the gross tumor volume (GTV, red), clinical target volume (CTV, pink), and planning target volume (PTV, light purple). A dose color-wash is displayed from 30% (blue) to 100% (red) of the prescribed dose. The configuration of the lateral multileaf collimator is visible on the sagittal images. (Images derived from Monaco Treatment Planning System, version 5.11.03 Elektra AB, Stockholm, Sweden).
Effectiveness of RT on tumor control and neurological signs
RT has consistently demonstrated efficacy in reducing tumor size and alleviating neurological signs caused by mass effect in both dogs and cats[125]. Tumor size reductions > 30% are frequently observed, with neurological improvement reported in 75%-91% of canine patients, depending on the protocol used[128,130,131]. Similar results are reported in cats, with improvement in neurologic signs in 91%-100% of cases[127,132-135].
Endocrine response
The endocrine response to RT (improvement of clinical signs, time to effect and the duration of response) is more variable, often necessitating the continuation of medical therapy and ongoing endocrine monitoring[125,136].
In dogs with PDH, clinical improvement is observed in approximately 36%-82% of treated individuals[103,126,129,130,137]. Median endocrine control durations of up to 27.6 months have been reported[138]. In cats with insulin-resistant diabetes mellitus, endocrine response is generally favorable, with insulin-related improvement in 56% to 95% of cases, and diabetic remission achieved in up to 32%, either temporary or permanent[127,134,135,139]. Concurrent endocrine signs began improving within 1-5 months[134]. These results highlight the potential of radiotherapy to induce substantial hormonal stabilization or even remission in feline pituitary tumor patients.
Survival outcomes
The reported median survival time (MST) in dogs varies with the RT protocol used. Conventionally fractionated radiotherapy (CFRT, 38-50 Gy in 10-20 fractions) is associated with the longest survival outcomes, with MSTs ranging from 514 to 688 days, with some studies reporting longer-term outcomes. Specifically, Kent et al. (2007)[126] reported a mean survival time (Mean ST) of 1,405 days, while the MST was not reached, indicating long-term survival in many cases. In this study, treated dogs with smaller pituitary tumors, based on pituitary-to-brain height ratio or area, had longer survival times than those with larger tumors[126].
Other CFRT-based studies reported MSTs of 514 days[129], 678 days[128], and 688 days[140]. One study found significantly longer survival times with a definitive RT protocol compared to a palliative approach (MST 605 vs. 262 days)[129]. In contrast, stereotactic radiosurgery (SRS) and stereotactic radiotherapy (SRT), which utilize higher doses in fewer fractions (e.g., 1 × 16 Gy or 3 × 8 Gy delivered over consecutive days), show MSTs between 118 and 357 days[130,141,142]. Although SRT/SRS can lead to rapid clinical improvement, they may not offer the same long-term survival benefit.
In cats, outcomes appear more favorable. MSTs after radiation therapy range from 508 to 1,072 days, with SRT protocols yielding the longest reported survivals[127,133-135,139]. Overall, RT provides prolonged survival in feline pituitary tumor patients, particularly when using stereotactic protocols[125,135,139]. However, in contrast to SRT, large-scale population studies evaluating CFRT in cats are lacking[125].
Adverse effects and complications
RT is generally well tolerated in both species. Corticosteroids are commonly administered during and shortly after the radiation treatment period to reduce the risk of secondary edema and associated clinical signs[125]. Reported late adverse events in dogs are relatively uncommon but have been reported and may include complications such as pituitary hemorrhage and otitis media[125,136]. In cats, the development of hypothyroidism post-SRT occurs in approximately 14% of cases and may require lifelong supplementation[139]. Although the overall incidence of toxicity is low, both early and late adverse effects warrant ongoing monitoring.
Combination therapy
In veterinary medicine, RT is an established primary treatment option for pituitary tumors[125]. Its potential role as an adjuvant therapy following incomplete surgical excision has not yet been the subject of dedicated veterinary studies.
In human medicine, postoperative radiation therapy significantly reduces recurrence rates following subtotal tumor resection, with 5- and 10-year recurrence rates as low as 2.3%[143].
Owing to advances in high-resolution imaging that enable early detection of recurrence and the proven efficacy of delayed radiotherapy, complete or near-complete resection without immediate postoperative radiotherapy remains a safe and pragmatic strategy in human medicine[143,144]. In veterinary medicine, no comparative studies have evaluated recurrence rates following hypophysectomy with or without adjuvant RT, but based on human data, postoperative radiation is a good treatment option when residual tumor or recurrence is present.
Comparison with human medicine and future perspectives
In human medicine, radiation therapy for pituitary adenoma is primarily used in cases of postoperative residual tumor, recurrence, or persistent hormonal hypersecretion[51,144]. Both CFRT and stereotactic techniques such as SRS and SRT provide excellent local tumor control, with reported rates of 90%-95% at 5 to 10 years[44,144]. Endocrine remission varies widely, ranging from 46% to 100% with conventional fractionation and 10% to 100% with stereotactic approaches[44]. The most common long-term adverse effect is hypopituitarism, occurring in 40%-62% of patients[47,51]. Advances in RT delivery, including Intensity-Modulated Radiation Therapy (IMRT), Volumetric Modulated Arc Therapy (VMAT), and especially proton therapy, allow for improved dose conformity and better sparing of adjacent critical structures[44,51,145]. Proton therapy, in particular, has shown promise in reducing the risk of visual impairment and long-term toxicity compared to photon-based techniques[47,51]. Although not yet commercially available in veterinary medicine due to cost and infrastructure limitations, proton therapy may become a viable option in selected veterinary patients, especially when critical neurovascular structures are at risk.
Novel intratumoral approaches, such as ^188Ho microbrachytherapy, have reduced tumor volume by 40% in reported experimental cases and may provide alternatives for large, inoperable tumors[146].
Going forward
Radiation therapy is an effective and often essential treatment modality for pituitary tumors in dogs and cats. While CFRT offers the best long-term survival in dogs, SRS/SRT protocols provide shorter treatment schedules with acceptable outcomes, especially in cats. Endocrine responses are variable, particularly in canine PDH, whereas cats can show good improvement in insulin resistance due to HS or PDH. Although radiotherapy can provide significant endocrine improvement in veterinary patients with pituitary tumors, the results are generally less favorable compared to surgical treatment. Adverse effects are generally minimal with modern RT planning, but long-term endocrine monitoring remains essential. Looking ahead, advancements in RT techniques, optimizing RT protocols and the potential integration of proton therapy may further refine treatment outcomes while reducing toxicity.
MEDICAL TREATMENT
In the past, before pituitary endocrinopathies were understood, diseases were often treated symptomatically, and over time, management shifted toward organ-targeted therapies as pituitary function became better understood.
Though surgery is the mainstay curative treatment option for functional pituitary masses in both human and veterinary medicine, there are multiple drugs that may be adopted from human medicine, and could be considered, now or in the future, as part of an individualized multimodal treatment plan [Figure 7].
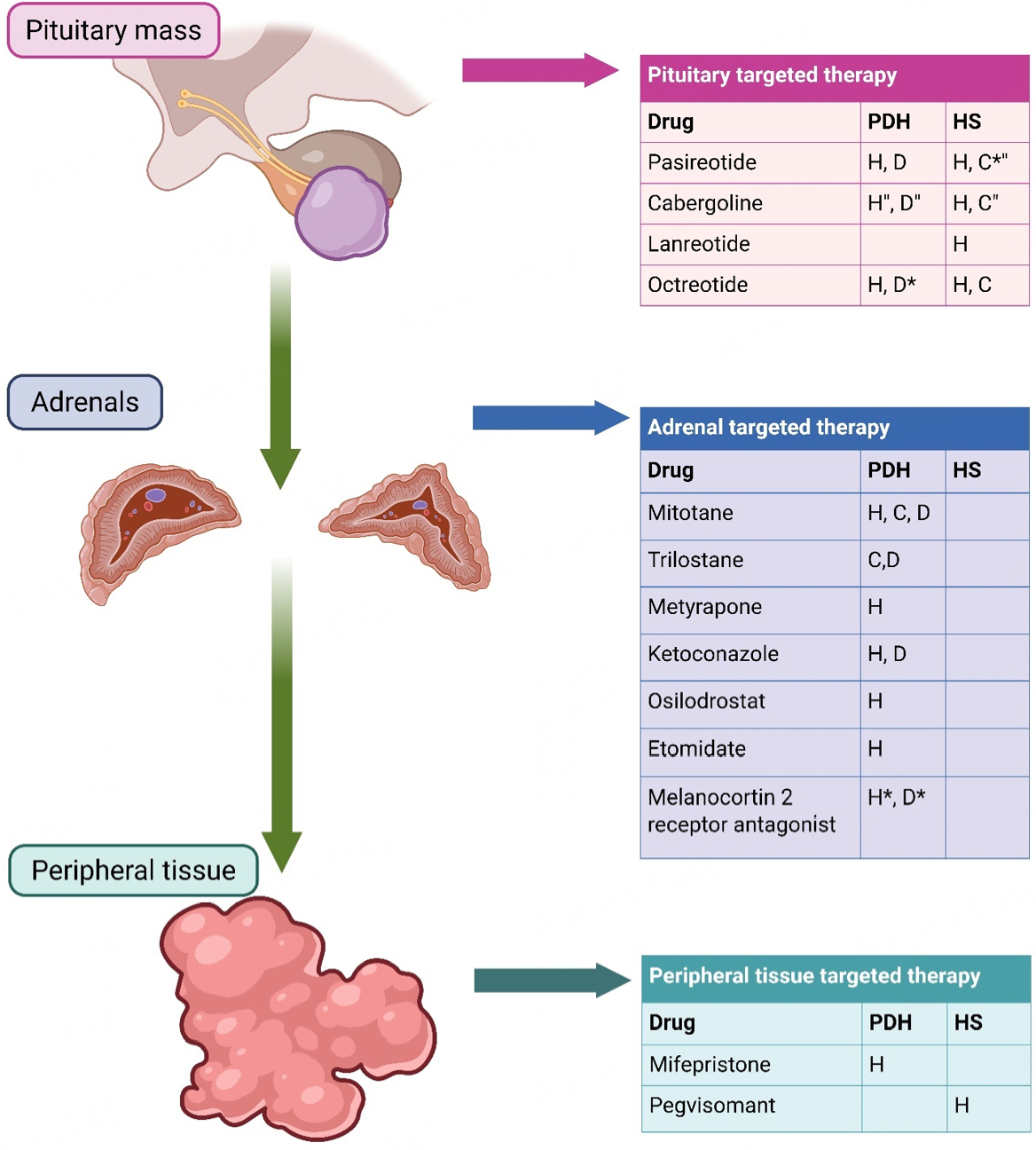
Figure 7. H: drug used in current treatment protocols in human medicine. Drugs used or suggested for medical treatment in veterinary medicine: C = applications in cats, D = applications in dogs. Applications marked with a * are currently investigated for their use. Applications marked with” have been applied but have limited effect. PDH: pituitary-dependent hypercortisolism in dogs and cats or CD in humans. HS: hypersomatotropism in cats and dogs or acromegaly in humans. (Created in BioRender. van Stee L. (2026) https://BioRender.com/atydvoi).
Pituitary-dependent hypercortisolism
In human medicine, metyrapone was discovered as an adrenal steroidogenesis inhibitor, and initially used in the diagnosis (in the late 1950s) and later also treatment of Cushing’s syndrome with a reported normalization of urine cortisol levels (urinary-free cortisol, UFC) in 70% of cases[48,147,148]. Starting from the early 1960’, the first cases in human Cushing’s syndrome and CD were treated with success with another steroidogenesis inhibitor, called mitotane, also referred to as o,p’dichlorodiphenyldichloroethane
Other pathways to treat CD were explored, and drugs such as the somatostatin receptor ligand pasireotide and dopamine receptor agonists like cabergoline were introduced[48]. Efficacy of pasireotide and pasireotide long-acting release, introduced as a treatment starting from 2005, is reported to be between 15%-26% and 40% UFC normalization respectively. Cabergoline has the same efficacy in lowering UFC with 40% normalization. Mifepristone became a drug of interest for the treatment of CD around 1985, though lacking cortisol markers of efficacy[48,150].
Current medical management is continuously updated through international cooperation and communicated through consensus statements[48]. Continuous monitoring is warranted and generally includes repeat imaging for tumor progression, urine free cortisol, and plasma ACTH levels. If the tumor shows progressive growth, the disease management plan should be re-evaluated[48].
In canine hypercortisolism, the adrenal cytotoxic agent mitotane, first adopted in veterinary medicine mid 1970s, was largely replaced by trilostane mid 2000s, now the drug of choice[1,151-157].
Hypersomatotropism
In human medicine, primary medical therapy or acromegaly is indicated in those patient who refuse surgical intervention, cases that have contraindications ruling out surgery or are considered to gain little benefit or have a high risk of poor outcomes after surgery. The first line drugs of choice are the somatostatin receptor ligands octreotide and lanreotide, due to their good safety profile and high efficacy. IGF-1 levels normalize in 30%-55% of patients on long-term treatment and tumor size can even decrease over 20% in more than half the treated cases[91]. Cabergoline is a relative cheap drug that has a limited role in human medicine, as its effects are relatively modest on reducing GH/IGF-1 levels. It is currently used in cases in which there is mild elevation of GH/IGF-1 after surgery, or as an add-on therapy where the maximal dose of somatostatin receptor ligands are unable to provide biochemical control[91]. As a second line of defense, the GH receptor antagonist pegvisomant can be introduced in the treatment plan.
Medical management of HS in veterinary medicine remains difficult. Somatostatin analogs have shown success in human medicine but its use in veterinary patients remains limited. The GH receptor antagonist pegvisomant has not been tested in dogs or cats due to species differences in protein and receptor structure.
Most commonly used medical interventional drugs for functional pituitary disease for human and veterinary patients are listed in Figure 7.
Pituitary-targeted therapies
Somatostatin and dopamine agonists
An ideal medical strategy for PDH would involve direct targeting of the pituitary adenoma. Both dopamine (DA) and somatostatin (SST) exert inhibitory effects on pituitary function. Current research focuses on three receptor subtypes: dopamine receptor subtype 2 (DRD2), and somatostatin receptor subtypes 2 (SSTR2) and 5 (SSTR5). In canine corticotroph adenomas, SSTR2 is the predominant receptor, whereas DRD2 and particularly SSTR5 are expressed at much lower levels[158]. This receptor distribution differs from human corticotroph adenomas, where DRD2 and SSTR5 predominate[158]. These interspecies differences are important when translating therapeutic findings between dogs and humans.
Cabergoline
Cabergoline, a dopamine agonist targeting DRD2, has shown only modest in vitro efficacy in canine corticotroph cells, consistent with the moderate DRD2 expression in these adenomas[158]. Nonetheless, in vivo studies have demonstrated that approximately 43% of dogs treated with cabergoline exhibit clinical improvement, including reduced clinical signs, decreased pituitary adenoma size, and lower urinary cortisol excretion[159]. In human medicine, cabergoline has been explored and found effective as a treatment for CD and acromegaly in selected patients[48,91]. In cats however, evidence is sparse and contradictory. A case series involving 90 cats with HS reported no therapeutic benefit, while another study found glycemic control (35% of cases) and normalizing of the IGF concentrations (26% of cases)[160,161]. In a small study of 25 dogs with PDH, cabergoline with or without trilostane failed to improve clinical signs when compared to trilostane alone, but may have some effect on pituitary tumor growth[162].
Pasireotide
Pasireotide is a somatostatin analog that binds SST receptors 1, 2, 3, and 5[163]. In dogs with PDH, it reduced plasma ACTH concentration and improved clinical signs without severe adverse effects[164]. In another study of nine dogs with macroadenomas, tumor volume decreased in six but increased in three, with no neurologic or other adverse effects[165]. In humans, pasireotide is approved as second-line therapy for CD when surgery fails or is not possible[43]. Because canine pituitary tumors causing PDH express SST2 strongly, analogs with higher SST2 affinity than pasireotide may be more effective, as shown in vitro[158].
Octreotide
Octreotide is a synthetic somatostatin analog that exhibits high binding affinity for somatostatin receptor subtype 2 (SSTR2) and moderate affinity for subtype 5 (SSTR5). Given the relatively high expression of SSTR2 in canine corticotroph adenomas, octreotide has been shown to significantly suppress ACTH secretion in cultured canine corticotroph cells in vitro, with greater efficacy than either pasireotide or cabergoline[158]. These findings suggest that long-acting formulations of octreotide may represent a promising therapeutic option for the management of PDH in dogs.
Lanreotide
Lanreotide is a synthetic somatostatin analog with a similar SSTR affinity and safety profile to that of octreotide and is also available as a long acting formulation[93]. It has not yet been investigated in dogs or cats.
Dopamine-somatostatin chimeras
Although both dopamine agonists and somatostatin analogs have demonstrated efficacy in the treatment of human pituitary adenomas, a substantial proportion of patients exhibit limited or no response. A novel therapeutic strategy involves the use of dopamine–somatostatin chimeric compounds. These agents promote heterodimerization of dopamine and somatostatin receptors, thereby facilitating the formation of a hybrid receptor with potentially enhanced signaling efficacy[166].
ACTH synthesis inhibitors
Retinoic acid
Pro-opiomelanocortin (POMC), the precursor of ACTH, is transcriptionally regulated by multiple transcription factors. Retinoic acid influences the binding activity of these transcription factors to their DNA recognition sites, thereby suppressing ACTH synthesis. In canine studies, administration of retinoic acid has been associated with reductions in plasma ACTH concentrations, urinary cortisol excretion, pituitary gland size, and with clinical improvement in PDH[167]. Furthermore, human studies have demonstrated that 9-cis retinoic acid, an active isomer of retinoic acid, can activate the dopamine receptor D2 (DRD2) promoter, thereby enhancing the responsiveness of pituitary adenomas to dopaminergic therapies[168]. In a small open trial, isotretinoin acid (13-cis-retinoic acid) was found to be effective and safe, in patients with CD and mild hypercortisolism[169].
Adrenal-targeted therapies
Steroidogenesis enzyme inhibitors [Figure 8]
Sterol-O-acyl-transferase 1 inhibitors and mitotane
Mitotane (o,p’-DDD) has been employed in the treatment of canine PDH for several decades. It functions as an adrenocorticolytic agent, inducing progressive necrosis and atrophy of adrenocortical tissue. Mitotane additionally inhibits key steroidogenic enzymes, including cytochrome P450 cholesterol side-chain cleavage enzyme (CYP11A1) and CYP11B1[170], thereby contributing to reduced cortisol synthesis. Moreover, it induces cytochrome P450 3A4 (CYP3A4), leading to increased metabolic clearance of cortisol[171]. Reported adverse effects include anorexia, lethargy, weakness, and diarrhea; if untreated, these may progress to life-threatening hypoadrenocorticoid crisis.
Recent studies have demonstrated that one of mitotane’s primary mechanisms is the inhibition of sterol-O-acyl-transferase 1 (SOAT1)[172]. SOAT1 catalyzes the esterification of free cholesterol in adrenocortical cells; its inhibition results in accumulation of free cholesterol, which is cytotoxic, induces endoplasmic reticulum stress, and promotes apoptosis[172]. Interestingly, dogs exhibit greater sensitivity to mitotane compared with other species, rendering them a useful model for further exploration of SOAT1 inhibition. The development of more selective SOAT1 inhibitors with adrenocorticolytic properties but fewer off-target toxicities may represent a promising therapeutic approach for PDH. Although effective, mitotane has largely been replaced by trilostane due to the latter’s comparable efficacy, safer handling, and reduced incidence of adverse effects.
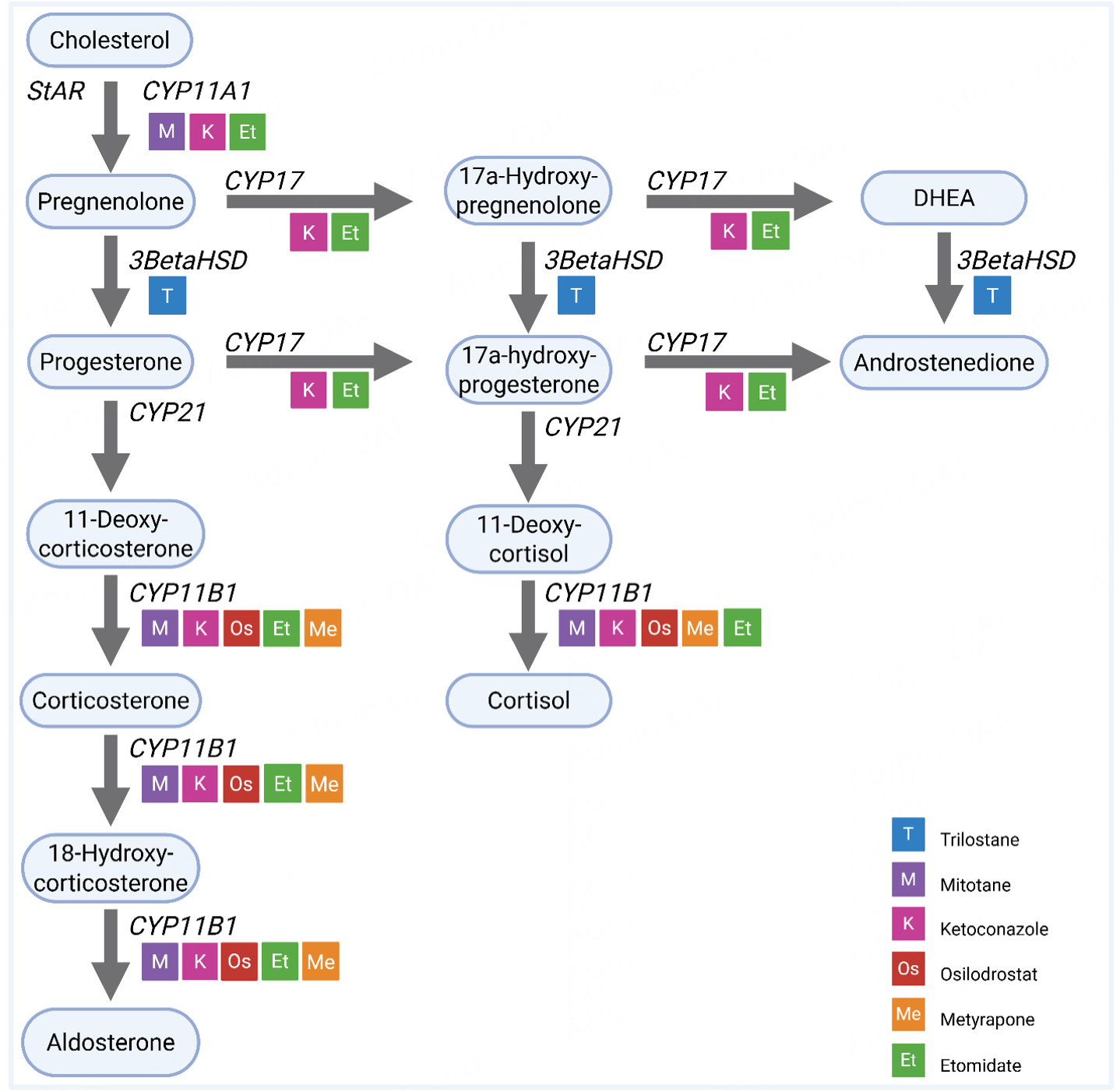
Figure 8. Steroidogenic acute regulatory protein (StAR).Cytochrome P450 cholesterol side-chain cleavage enzyme (CYP) 11A1, 11B1, 17, 21. Steroidogenic enzyme 3β-hydroxysteroid dehydrogenase (3BetaHSD). (Created in BioRender. van Stee L (2026) https://BioRender.com/5avxvms).
Trilostane
Currently, trilostane is the drug of choice for dogs with PDH. Trilostane is a synthetic steroid analog that competitively inhibits the steroidogenic enzyme 3β-hydroxysteroid dehydrogenase (HSD3B2), which is required for the production of both glucocorticoids and mineralocorticoids. Trilostane therefore inhibits both cortisol production, which results in less negative feedback and a compensatory increase in plasma ACTH concentration, and aldosterone production, which causes a compensatory increase in plasma renin activity[155]. Additionally, trilostane possibly also inhibits other enzymes in the steroidogenesis cascade, such as 11β-hydroxylase (CYP11B1).
There is a significant interindividual variation in the optimal trilostane dose. For successful management of PDH with trilostane, frequent monitoring is essential. Trilostane is usually well tolerated, but the main adverse effect that can occur is (transient) hypocortisolism, possibly combined with or followed by complete hypoadrenocorticism, i.e., hypocortisolism and hypoaldosteronism[173]. Although trilostane effectively controls the clinical signs of glucocorticoid excess in dogs with PDH, it does not directly affect the growth of the pituitary tumor. While this seems less relevant for dogs initially presented with nonenlarged pituitary glands, the pituitary tumor may exhibit growth over time, and prolonged treatment may lead to the pituitary tumor progression[152,153]. The median survival times of dogs with PDH treated with trilostane have been reported to be 662-852 days (range, 2-3210)[154-157].
(Levo)Ketoconazole
Ketoconazole, a synthetic imidazole derivative originally developed as an antifungal agent, exerts inhibitory effects on multiple cytochrome P450 enzymes, including CYP11A1, CYP17A1, and CYP11B1[65], thereby suppressing cortisol biosynthesis. While ketoconazole has been applied in canine PDH management, its use has been limited due to suboptimal efficacy and a higher incidence of adverse effects compared with trilostane. Levoketoconazole, the purified enantiomer of racemic ketoconazole, has demonstrated greater potency in inhibiting cortisol synthesis with reduced hepatotoxicity in both in vitro and in vivo studies in humans with CD[174].
Metyrapone
Metyrapone is a potent steroidogenesis inhibitor that specifically blocks 11β-hydroxylase, effectively reducing cortisol production[175]. In human medicine, metyrapone is primarily used for preoperative stabilization in patients with CD and may also be considered in refractory cases. Metyrapone has not been tested in veterinary patients with PDH yet.
Osilodrostat
Osilodrostat was originally developed as a treatment for hypertension, cardiac failure and renal disease. When tested on human patients with hypertension, not only serum aldosterone levels dropped, but also the cortisol response to synthetic ACTH. Osilodrostat is an inhibitor of 11β-hydroxylase and exhibits a potent reduction of cortisol production. It has a high efficacy and good safety profile and appears to show sustained effect during long term treatment of CD[176]. It inhibits CYP11B2 and CYP11B1[174]. Osilodrostat has not been tested in veterinary patients with PDH yet.
Etomidate
Etomidate is an intravenous imidazole derivative, used in anesthesia as an induction agent and inhibits CYP11B1, CYP17A1 and CYP11A1 in a dose dependent manner[174]. It rapidly acts and lowers cortisol efficiently on a low dose within 11 hours after infusion. Its efficacy in decreasing serum cortisol levels in emergency cases is second to none[174]. Its application is therefore specifically for cases that suffer from acute and/or life threatening complications of CD, enabling up to 80.9% of patients to survive and receive a definite treatment[177,178]. Etomidate has not been tested in veterinary patients with PDH yet.
Adrenocorticotropic hormone pathway modulators
Melanocortin 2 receptor antagonists
The melanocortin 2 receptor (MC2R), the exclusive receptor for Adrenocorticotropic hormone (ACTH), is expressed solely within the adrenal cortex[179]. A selective MC2R antagonist has considerable therapeutic potential for PDH, as it would directly counteract ACTH-mediated adrenal overstimulation. However, receptor selectivity is essential, as unintended activity at other melanocortin receptors could precipitate undesirable adverse effects. Continued research is warranted to develop highly selective MC2R antagonists suitable for clinical use, as these drugs are currently only tested in veterinary medicine in vitro[180].
Steroidogenic factor-1 (SF-1) inverse agonists
Steroidogenic factor-1 (SF-1) is an orphan nuclear receptor that regulates adrenal development, growth, and steroidogenesis[181]. ACTH enhances SF-1 transcriptional activity, stimulating expression of genes encoding steroidogenic enzymes. Hyperactivation of SF-1 has been implicated in PDH pathophysiology, and its inhibition may represent a novel therapeutic avenue for disease management[182].
Peripheral receptor targeted therapy
Cortisol receptor antagonists
Mifepristone
Mifepristone is a competitive glucocorticoid and progesterone receptor antagonist, and is also known as RU 486. It is an older drug, that was first introduced as a treatment option for Cushing’s syndrome in 1985, and is currently considered as an adjuvant therapy[150]. It is approved by the United States Food and Drug Administration (FDA) in 2012 to control hyperglycemia secondary to hypercortisolism. In particular for patients who are diagnosed with type 2 diabetes mellitus or glucose intolerance and are considered not to be a surgical candidate, or failed prior surgery[183]. Significant clinical improvement has been reported in 87% of patients. ACTH and cortisol levels remain unchanged, and will need monitoring over time. Side effects reported in human medicine include cortisol withdrawal symptoms, antiprogesterone effects (endometrial thickening and vaginal bleeding), and changes in thyroid function marked by an increase in TSH and decrease in T4, alongside hypertension and hypokalemia[183]. As mifepristone is likely to improve insulin resistance, dosage of antidiabetic drugs like insulin, may need to be adjusted[183]. Safe and effective use of mifepristone requires clinical judgment and close patient monitoring to ensure optimal clinical outcomes[184]. It can also be used as a “bridge” therapy in patients receiving pituitary radiotherapy and as pre-hypophysectomy treatment in high-risk patients[185]. The half-life time of mifepristone in humans (~85 h) needs to be considered as it will take up to 2 weeks’ time to be cleared from circulation[180]. Mifepristone has not been tested in veterinary patients with PDH yet.
Growth hormone receptor antagonists
Pegvisomant
Pegvisomant is a polyethylene glycol (PEG)-modified analog of human GH that acts as a competitive antagonist at the GH receptor. At present, it remains the only commercially available pharmacological agent targeting GH excess in the treatment of acromegaly in humans. Due to species specificity of growth hormone and its receptor, pegvisomant cannot be applied in dogs or cats[186]. However, a related compound has been developed for dogs and successfully tested in vitro[186].
Translational potential of orphan drugs
At present, pharmacological options for the medical management of pituitary disease in companion animals remain limited. For PDH, treatment mainly involves trilostane and, in selected cases, mitotane. In contrast, medical management of HS in cats (and dogs) is largely limited to symptomatic treatment only. It is here, where orphan drugs and human medical experience can make the difference; especially for those cases in which a curative intent treatment is not available or achievable. Figure 7 displays the drugs currently used in the treatment of both HS and PDH in dogs and cats and their human companions.
Common challenges associated with the use of orphan drugs in veterinary medicine include limited availability, high cost, and regulatory restrictions. Some of the drugs described above have already been used in veterinary medicine for other indications, although they are often replaced by newer agents with fewer adverse effects. Examples include cabergoline for the treatment of pseudopregnancy, ketoconazole for the treatment of fungal skin infections, and etomidate as an anesthetic induction agent in dogs and cats.
Cabergoline has shown efficacy in selected human patients with acromegaly or CD and dogs with PDH[48,91,159]. Trials in cats with HS have not demonstrated significant improvement in clinical signs, with results ranging from no benefit overall, to reasonable effect on only a small part of the animals treated[160,161].
Ketoconazole has been suggested as an alternative to mitotane in the past and is able to improve clinical signs in dogs as a single drug treatment for PDH, with a reported median survival time of 25 months in a cohort of 48 dogs[187]. However, following the introduction of trilostane, that has a high safety profile, the use of ketoconazole in veterinary medicine was never fully explored[153-157,173]. In human medicine, (levo)ketoconazole is used both as monotherapy and as part of combination therapy in CD[48]. Combination therapy is typically implemented when monotherapy fails to achieve adequate disease control or when adverse effects necessitate dose reduction. In such cases, drugs such as ketoconazole, cabergoline, pasireotide, metyrapone, and mitotane may be used in combination with two or more agents[48]. Combination therapy in PDH may warrant greater consideration in veterinary medicine, as failure to respond to the standard-of-care treatment with trilostane presents a significant therapeutic challenge, particularly when definitive treatment in the form of transsphenoidal hypophysectomy is not available. A recent study evaluated combination therapy in dogs with PDH by combining trilostane with cabergoline. Although the authors did not report a significant improvement in clinical signs compared with trilostane monotherapy, they suggested that cabergoline may have a potential effect on reducing tumor growth[162]. As current medical treatment with trilostane in dogs with PDH does not address the growth of the pituitary mass, the addition of cabergoline may be beneficial in cases where tumor progression is a concern[162].
Drugs that may become of interest for the treatment of canine PDH and feline HS in the near future are the somatostatin agonists. These drugs are a mainstay in human medicine for the treatment of CD and acromegaly. While pasireotide has already shown in vivo efficacy in the treatment of PDH in dogs, the affinity to SSTR2 of octreotide and lanreotide make these drugs more interesting in this species, due to the strong expression of this receptor withing their pituitary adenomas[158,164-165]. In cats, early investigation on the efficacy of octreotide on lowering GH and blood glucose levels in cats with HS showed marked but variable decrease of both parameters[188]. In the almost 2 decades onwards, little progress was made. More recently, pasireotide has been evaluated for its effect on HS in few clinical case series with promising results in both short acting and long acting pasireotide[189,190]. Still, large clinical trials are lacking in both canine and feline medicine.
Peripheral receptor targeted therapy may be an interesting option for all species in both PDH/CD and HS/acromegaly. Mifepristone, is a typical orphan drug with a primary registration as an early pregnancy termination agent in human medicine. Although in the past it has been registered for the treatment of Cushing’s syndrome in human patients too, it is now again being considered as an adjuvant treatment for its glucocorticoid receptor antagonism[150]. In theory, this drug may have similar effects in dogs and cats, though the primary effect (i.e., anti-progestagen) of mifepristone in cats appears to be inferior when compared to the veterinary alternative aglepristone[191]. However, mifepristone was effective in a small study on pregnancy termination in 5 beagle dogs, suggesting species variation in receptor affinity in at least the main target receptor[192]. The species specific anti-glucocorticoid receptor affinity of mifepristone remains unknown and will need further investigation[191,192].
Veterinary patients may play a more prominent role in the development of orphan drugs for rare pituitary diseases in humans. This is particularly relevant as disease progression in these animals closely parallels that observed in humans, while occurring naturally. Integrating veterinary patient care into the early phases of human drug development could therefore benefit both species. Furthermore, the implementation of novel ex vivo and cell-based testing strategies may allow veterinary patient models to support more targeted and individualized treatment development, while reducing reliance on experimental small and large animal models (the 3R’s)[193-196] [Figure 9]. At a time when more individualized treatment strategies are in demand, organoid and organ-on-a-chip technologies may ultimately become routine diagnostic and translational research tools. These platforms provide an ethically responsible, sophisticated, and potentially cost-effective approach to studying and treating rare pituitary tumors.
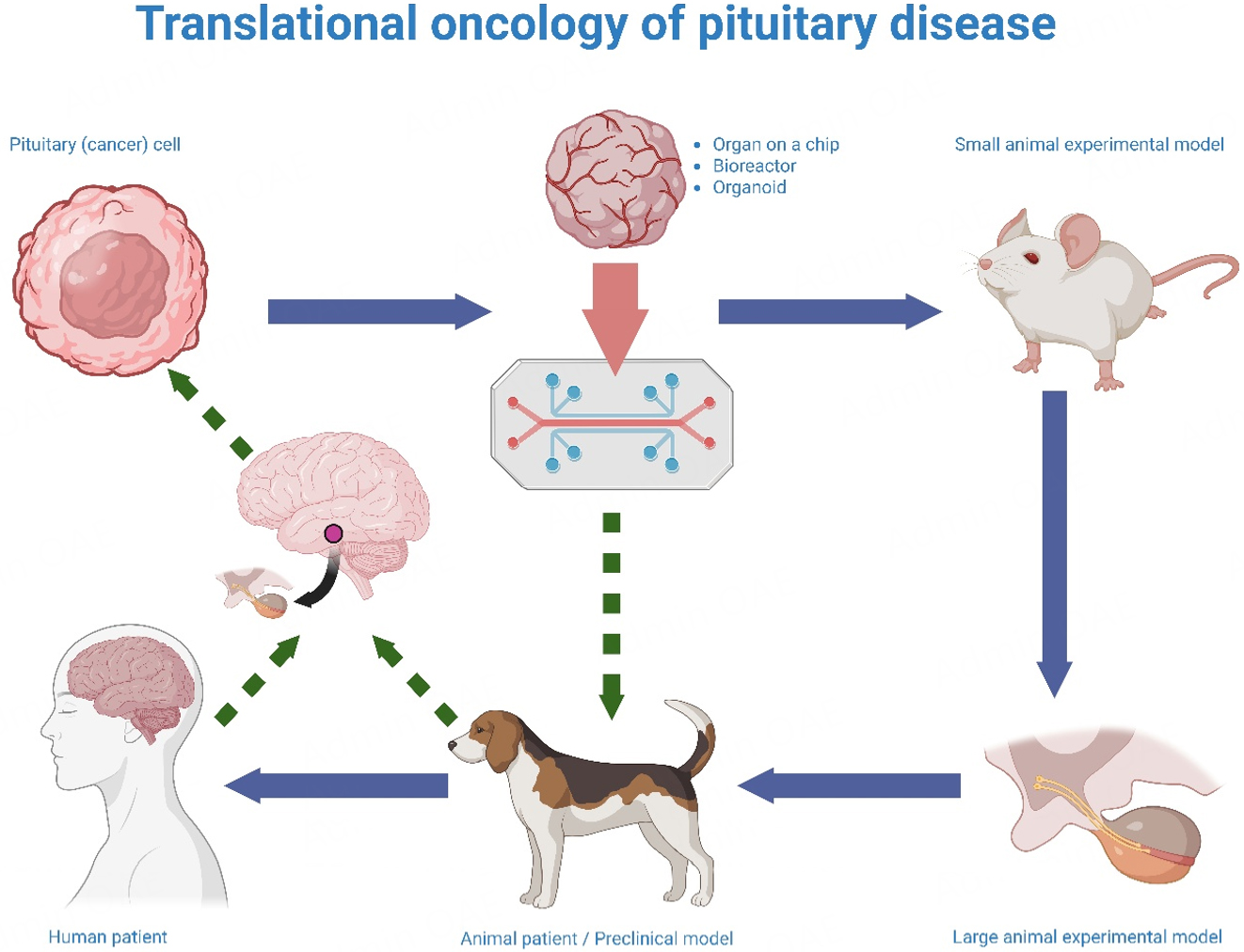
Figure 9. Translational modeling of pituitary neoplasia using patient-derived systems. Tumor tissue or single cells obtained from donor animals or patients (e.g., dogs or humans) with pituitary neoplasia can be used to generate organoids, organ-on-a-chip platforms, or bioreactor models. These systems enable investigation of novel therapeutic modalities in patient-derived tumor populations within controlled microenvironments that more closely recapitulate in vivo tumor behavior and treatment response, while reducing reliance on laboratory animals in accordance with the 3Rs (Replacement, Reduction, Refinement). Comparative animal patients with naturally occurring disease analogous to human pathology may be incorporated at later translational stages. Dogs, cats, and horses develop spontaneous pituitary neoplasms that often resemble human disease, supporting their role in comparative and translational research. (Created in BioRender. van Stee L. (2026) https://BioRender.com/i5zja56).
CONCLUSION
Transsphenoidal surgery remains a cornerstone in the treatment of pituitary disorders in both humans and companion animals. While pharmacotherapeutic interventions are continuously evolving, surgical or radiotherapeutic management should be considered for treatment of functional masses with curative intent, particularly for patients with large pituitary masses, acromegaly, or CD. Radiotherapy remains a good treatment of choice, however, it does not consistently eliminate the underlying endocrine disorder, on top of carrying a significant risk of inducing hypopituitarism and damage to surrounding anatomical structures. Given the limited availability of specialized surgical facilities in veterinary medicine, combined radiotherapy and medical management currently represent the more feasible therapeutic option, although expanding access to surgical expertise remains a critical goal. In refractory cases or following recurrent tumor growth after hypophysectomy, a multimodal approach as suggested in human treatment protocols may provide additional clinical benefit[32,48,91,93]. Combining medical management, and radiation therapy, with or without a second surgical procedure, may be optimal. In cases of pituitary nonfunctioning adenomas or silent pituitary masses, both surgery and radiotherapy are a valid option. Surgery may provide a faster decompression, while radiation therapy is more available overall.
As in human medicine, the development of specialized veterinary centers that offer multidisciplinary expertise will be essential to meet the growing demand for advanced care in these complex cases. Knowledge transfer should extend beyond surgical techniques to encompass preoperative assessment, advanced pituitary imaging, 3D multiplanar reconstruction for localization, intraoperative visualization, intensive care unit management, and long-term postoperative care. Establishing such integrated care models in veterinary practice will mirror established protocols in human medicine and improve clinical outcomes.
The role of translational medicine is particularly significant in this context. By adapting and refining established methodologies from human medicine for veterinary use, clinicians can capitalize on proven strategies while avoiding unnecessary risks associated with untested experimental techniques. Advances in surgical training, including the use of high-fidelity simulations and in vitro models, provide opportunities for veterinarians to develop and maintain technical proficiency without reliance on ethically problematic in vivo or ex vivo practice. These approaches also enable repeated, standardized training, enhancing surgical dexterity and preparedness.
Further progress in treatment of pituitary masses in companion animals will depend on the standardization of diagnostic work-up and postoperative follow-up, as well as the establishment of collaborative frameworks for data collection and sharing; processes already successfully implemented in human medicine[97,120]. The accumulation of larger datasets will facilitate the development of patient-specific treatment protocols and contribute to improved clinical outcomes.
Ultimately, the optimal management of pituitary disease in companion animals requires a multimodal strategy encompassing diagnostic evaluation, surgical and/or radiotherapeutic intervention, pharmacotherapy, and postoperative care. A collaborative, multidisciplinary treatment team—including specialists in internal medicine, radiology, anesthesia, critical care, and surgery—is indispensable. Such an integrated approach fosters a safe and effective treatment environment, ensuring the highest standard of care for veterinary patients.
DECLARATIONS
Acknowledgments
We would like to thank Remko van Deijk for granting permission to reuse his illustration of transoral endoscopy of the pituitary fossa in the dog [Figure 5]. The illustration was created using Adobe Photoshop CS5 and Adobe Illustrator CS5 (Adobe Inc.). The graphical abstract was created in BioRender. van Stee L. (2026) https://BioRender.com/bjhguoy.
Authors’ contributions
Made substantial contributions to conception and original draft, revision, editing and visual contributions, correspondence with the editorial office: van Stee L
Made substantial contributions to conception and original draft, editing, revision and correspondence with the editorial office:
Made substantial contributions to the original draft, revision, editing and visual contributions:
Made substantial contributions to the original draft, editing, revision and visual contributions: Galac S, Kooistra H
Availability of data and materials
Not applicable.
AI and AI-assisted tools statement
Not applicable.
Financial support and sponsorship
None.
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Galac S, Fracassi, F. Canine endocrinology. In: CH 23: hypothalamus and pituitary gland: anatomy and physiology. Edra Publishing US LLC, 2024; pp. 107-10.
2. Rijnberk A, Kooistra HS. Chapter 2: Hypothalamus-pituitary system. In: Clinical endocrinolongy of dogs and cats, an illustrated text. Schlütersche, 2010; pp. 13-54.
5. Del Magno S, Fracassi F, Grinwis GC, et al. Sequential treatment of a large pituitary corticotroph neoplasm and associated neurological signs in a dog. J Am Anim Hosp Assoc. 2019;55:e552-02.
6. Steele MME, Lawson JS, Scudder C, et al. Transsphenoidal hypophysectomy for the treatment of hypersomatotropism secondary to a pituitary somatotroph adenoma in a dog. J Vet Intern Med. 2024;38:351-7.
7. Blokland-Post K, Grinwis G, Tellegen A, Meij B. Transsphenoidal hypophysectomy as a treatment for Rathke's cleft cyst in a dog. Vet Record Case Rep. 2022;10:e427.
8. Lehner L, Garamvölgyi R, Jakab C, Kerekes Z, Czeibert K. A recurrent suprapituitary ependymal cyst managed by endoscopy-assisted transsphenoidal surgery in a canine: a case report. Front Vet Sci. 2019;6:112.
9. Hyde BR, Martin LG, Chen AV, et al. Clinical characteristics and outcome in 15 dogs treated with transsphenoidal hypophysectomy for nonfunctional sellar masses. Vet Surg. 2022;52:69-80.
10. Martin L, Owen T, Chen-Allen A, Turner A, Carrera-Justiz S, Bruyette D. Clinical characteristics and outcome in dogs treated with transsphenoidal hypophysectomy for non-functional sellar masses. J Vet Intern Med. 2016;30:1941.
11. Owen T, Chen A, Martin L. Why, when, how and post-operative care of dogs undergoing transphenoidal hypophysectomy for large sellar masses. J Vet Intern Med 2016;30:1939. Available from: https://academic.oup.com/jvim/article/30/6/1929/8449772?login=false [Last accessed on 2 Jun 2026].
12. Owen TJ, Martin LG, Chen AV. Transsphenoidal surgery for pituitary tumors and other sellar masses. Vet Clin N Am Anim Pract. 2018;48:129-51.
13. Corsello A, Di Dalmazi G, Pani F, et al. Dandy: his contributions to pituitary surgery in the context of the overall Johns Hopkins Hospital experience. Pituitary. 2017;20:683-91.
14. Meij B, Voorhout G, Gerritsen R, Grinwis G, Ijzer J. Lymphocytic hypophysitis in a dog with diabetes insipidus. J Comp Pathol. 2012;147:503-7.
15. Rzechorzek NM, Liuti T, Stalin C, Marioni-Henry K. Restored vision in a young dog following corticosteroid treatment of presumptive hypophysitis. BMC Vet Res. 2017;13:63.
16. Bertolini G, Rossetti E, Caldin M. Pituitary apoplexy-like disease in 4 dogs. J Vet Intern Med. 2007;21:1251.
17. Tanaka S, Suzuki S, Oishi M, Soeta S, Namiki R, Hara Y. Adrenocorticotropic hormone-producing pituitary adenoma with pituitary apoplexy treated by surgical decompression: a case report. BMC Vet Res. 2022;18:397.
18. Galli G, Bertolini G, Dalla Serra G, Menchetti M. Suspected pituitary apoplexy: clinical presentation, diagnostic imaging findings and outcome in 19 dogs. Vet Sci. 2022;9:191.
19. Woelfel CW, Mariani CL, Nolan MW, et al. Presumed pituitary apoplexy in 26 dogs: clinical findings, treatments, and outcomes. J Vet Intern Med. 2023;37:1119-28.
20. Barnhart KF, Edwards JF, Storts RW. Symptomatic granular cell tumor involving the pituitary gland in a dog: a case report and review of the literature. Vet Pathol. 2001;38:332-6.
21. Ishino H, Takekoshi S, Teshima T, Uchida K, Sakonju I, Hara Y. Hyperadrenocorticism caused by a pituitary ganglioglioma in a dog. Vet Pathol. 2019;56:609-13.
22. Polledo L, Grinwis GCM, Graham P, Dunning M, Baiker K. Pathological findings in the pituitary glands of dogs and cats. Vet Pathol. 2018;55:880-8.
23. Miller MA, Bruyette DS, Scott-Moncrieff JC, et al. Histopathologic findings in canine pituitary glands. Vet Pathol. 2018;55:871-9.
24. Snyder J, Lipitz L, Skorupski K, Shofer F, Van Winkle T. Secondary intracranial neoplasia in the dog: 177 cases (1986-2003). J Vet Intern Med. 2008;22:172-7.
25. Gutierrez-Quintana R, Carrera I, Dobromylskyj M, Patterson-Kane J, Ortega M, Wessmann A. Pituitary metastasis of pancreatic origin in a dog presenting with acute-onset blindness. J Am Anim Hosp Assoc. 2013;49:403-6.
26. Tamura S, Tamura Y, Suzuoka N, Ohoka A, Hasegawa T, Uchida K. Multiple metastases of thyroid cancer in the cranium and pituitary gland in two dogs. J Small Anim Pract. 2006;48:237-9.
27. Menchetti M, De Risio L, Galli G, et al. Neurological abnormalities in 97 dogs with detectable pituitary masses. Vet Q. 2019;39:57-64.
28. Zou D, Yang Y, Gao R, et al. Long-term pituitary function following transsphenoidal surgery for non-functional pituitary neuroendocrine tumor with apoplexy: a single-center retrospective analysis. Sci Rep. 2025;15:19226.
29. Miller MA, Piotrowski SL, Donovan TA, et al. Feline pituitary adenomas: correlation of histologic and immunohistochemical characteristics with clinical findings and case outcome. Vet Pathol. 2020;58:266-75.
30. Wang MTM, Meyer JA, Danesh-Meyer HV. Neuro-ophthalmic evaluation and management of pituitary disease. Eye. 2024;38:2279-88.
31. Shah A, Mohamed Elsanafiry M. Diaphragma sellae: anatomical and surgical implication in surgery for pituitary adenomas - Highlighting contributions by Goel. J Craniovertebr Junction Spine. 2018;9:135.
32. Meij BP, Van Stee LL. Transsphenoidal surgery for pituitary tumors. Vet Clin N Am Anim Pract. 2025;55:95-118.
33. Teshima T, Hara Y, Shigihara K, et al. Coexistence of corticotroph adenoma and thyrotroph hyperplasia in a dog. J Vet Med Sci. 2009;71:93-8.
34. Lillehei KO, Travers S, Barkhoudarian G, Oyesiku NM, Germano IM, Ormond DR. Congress of neurological surgeons systematic review and evidence-based guidelines for the role of surgery for patients with functioning pituitary adenomas. Neurosurgery. 2025;97:24-35.
35. Makarenko S, Alzahrani I, Karsy M, Deopujari C, Couldwell WT. Outcomes and surgical nuances in management of giant pituitary adenomas: a review of 108 cases in the endoscopic era. J Neurosurg. 2022;137:635-46.
36. Khan DZ, Hanrahan JG, Baldeweg SE, Dorward NL, Stoyanov D, Marcus HJ. Current and future advances in surgical therapy for pituitary adenoma. Endocr Rev. 2023;44:947-59.
37. Jho H, Carrau RL. Endoscopic endonasal transsphenoidal surgery: experience with 50 patients. J Neurosurg. 1997;87:44-51.
38. Micko A, Agam MS, Brunswick A, et al. Treatment strategies for giant pituitary adenomas in the era of endoscopic transsphenoidal surgery: a multicenter series. J Neurosurg. 2022;136:776-85.
40. Nieman LK, Biller BMK, Findling JW, et al. Treatment of cushing's syndrome: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2015;100:2807-31.
41. Puig-Domingo M, Bernabéu I, Picó A, et al. Pasireotide in the personalized treatment of acromegaly. Front Endocrinol. 2021;12:648411.
42. Riley G, Scheyer N, Klein M, et al. Prognostic indicators in pituitary adenoma surgery: a comprehensive analysis of surgical outcomes and complications. Front Endocrinol. 2024;14:1327404.
43. Simeoli C, Auriemma RS, Tortora F, et al. The treatment with pasireotide in Cushing’s disease: effects of long-term treatment on tumor mass in the experience of a single center. Endocrine. 2015;50:725-40.
44. Starke RM, Williams BJ, Vance ML, Sheehan JP. Radiation therapy and stereotactic radiosurgery for the treatment of Cushing's disease: an evidence-based review. Curr Opin Endocrinol Diabetes Obes. 2010;17:356-64.
45. Tabaee A, Anand VK, Barrón Y, et al. Endoscopic pituitary surgery: a systematic review and meta-analysis: Clinical article. J Neurosurg. 2009;111:545-54.
46. Tang OY, Hsueh WD, Eloy JA, Liu JK. Giant pituitary adenoma - special considerations. Otolaryngol Clin North Am. 2022;55:351-79.
47. Wattson DA, Tanguturi SK, Spiegel DY, et al. Outcomes of proton therapy for patients with functional pituitary adenomas. Int J Radiat Oncol Biol Phys. 2014;90:532-9.
48. Fleseriu M, Auchus R, Bancos I, et al. Consensus on diagnosis and management of Cushing’s disease: a guideline update. Lancet Diabetes Endocrinol. 2021;9:847-75.
49. Meij BP. Hypophysectomy as a treatment for canine and feline cushing's disease. Vet Clin N Am Anim Pract. 2001;31:1015-41.
50. Sanders K, Kooistra H, Galac S. Treating canine Cushing’s syndrome: current options and future prospects. Vet J. 2018;241:42-51.
51. Brand A, Agolli L, Tas KT, et al. Long-term outcomes of modern radiation therapy for pituitary adenoma - different techniques: single institute experience. J Neurooncol. 2025;175:1039-50.
53. Cucu AI, Costea CF, Perciaccante A, Donell ST, Bianucci R. The evolution of pituitary gland surgery from the ancients to the millennials. World Neurosurg. 2023;180:52-65.
54. Horsley V. Abstracts of the brown lectures, delivered at the University of London. Lecture III: functional nervous disorders due to loss of thyroid gland and pituitary body. Lancet. 1886:3-5.
55. Horsley V. Address in surgery: on the technique of operations on the central nervous system. BMJ. 1906;2:411-23.
57. Cushing H. The pituitary body and its disorders; clinical states produced by disorders of the hypophysis cerebri. An amplification of the Harvey lecture for December, 1910. Available from: https://archive.org/details/pituitarybodyits00cushuoft/page/n9/mode/2up [Last accessed on 12 Jun 2026].
58. Cushing H. Partial hypophysectomy for acromegaly. With remarks on the function of the hypophysis. Ann Surg. 1909;50:1002-17.
59. Cushing H. Studies in intracranial physiology & surgery. The Cameron Prize Lectures. Oxford University Press; 1926, pp. 52-103.
61. Artico M, Pastore FS, Fraioli B, Giuffrè R. The contribution of davide giordano (1864-1954) to pituitary surgery: the transglabellar-nasal approach. Neurosurgery. 1998;42:909-11.
62. Cope VZ. The pituitary fossa, and the methods of surgical approach thereto. Br J Surg. 1916;4:107-44.
64. Macfarlane J, Bashari WA, Senanayake R, et al. Advances in the imaging of pituitary tumors. Endocrinol Metab Clin North Am. 2020;49:357-73.
65. Creemers SG, Hofland LJ, Lamberts SW, Feelders RA. Cushing’s syndrome: an update on current pharmacotherapy and future directions. Expert Opin Pharmacother. 2015;16:1829-44.
66. De Nijs L, Fomekong E, Maiter D, Raftopoulos C. Surgical treatment of cushing’s disease: the lessons learned. In: Di Rocco C, editors. Advances and technical standards in neurosurgery. Cham: Springer Nature Switzerland; 2025. pp. 47-73.
67. Esposito D, Olsson DS, Ragnarsson O, Buchfelder M, Skoglund T, Johannsson G. Non-functioning pituitary adenomas: indications for pituitary surgery and post-surgical management. Pituitary. 2019;22:422-34.
68. Liu JK, Das K, Weiss MH, Laws ER, Couldwell WT. The history and evolution of transsphenoidal surgery. J Neurosurg. 2001;95:1083-96.
69. Lubberink AA. Diagnosis and treatment of canine cushing’s syndrome. Tijdschr Diergeneeskd. 1989;114:37S-9.
70. Meij BP, Voorhout G, Ingh TSVD, Hazewinkel HA, Verlaat JWV. Transsphenoidal hypophysectomy in beagle dogs: evaluation of a microsurgical technique. Vet Surg. 2008;26:295-309.
71. Meij BP, Voorhout G, Van Den Ingh TS, Rijnberk A. Transsphenoidal hypophysectomy for treatment of pituitary-dependent hyperadrenocorticism in 7 cats. Vet Surg. 2004;30:72-86.
72. Meij BP, Auriemma E, Grinwis G, Buijtels JJCWM, Kooistra HS. Successful treatment of acromegaly in a diabetic cat with transsphenoidal hypophysectomy. J Feline Med Surg. 2010;12:406-10.
73. Meij B, Van Der Vlugt-Meijer R, Van Den Ingh T, Rijnberk A. Somatotroph and corticotroph pituitary adenoma (double adenoma) in a cat with diabetes mellitus and hyperadrenocorticism. J Comp Pathol. 2004;130:209-15.
74. Meij BP, Van Der Vlugt-Meijer RH, Van Den Ingh TSGAM, Flik G, Rijnberk A. Melanotroph pituitary adenoma in a cat with diabetes mellitus. Vet Pathol. 2005;42:92-7.
75. Rivenburg R, Owen TJ, Martin LG, Chen AV. Pituitary surgery: changing the paradigm in veterinary medicine in the United States. J Am Anim Hosp Assoc. 2021;57:73-80.
76. Cappabianca P, Cavallo LM, De Divitiis O, Solari D, Esposito F, Colao A. Endoscopic pituitary surgery. Pituitary. 2008;11:385-90.
77. Das A, Sidiqi B, Mennillo L, et al. Automated surgical skill assessment in endoscopic pituitary surgery using real-time instrument tracking on a high-fidelity bench-top phantom. Healthc Technol Lett. 2024;11:336-344.
78. Das A, Khan DZ, Psychogyios D, et al. PitVis-2023 challenge: workflow recognition in videos of endoscopic pituitary surgery. Med Image Anal. 2025:106;103716.
79. Mao Z, Das A, Islam M, et al. PitSurgRT: real-time localization of critical anatomical structures in endoscopic pituitary surgery. Int J Comput Assist Radiol Surg. 2024;19:1053-60.
80. Mamelak AN, Owen TJ, Bruyette D. Transsphenoidal surgery using a high definition video telescope for pituitary adenomas in dogs with pituitary dependent hypercortisolism: methods and results. Vet Surg. 2014;43:369-79.
81. Van Stee LL, Van Rijn SJ, Galac S, Meij BP. Challenges of transsphenoidal pituitary surgery in severe brachycephalic dogs. Front Vet Sci. 2023;10:1154617.
82. Hanson JM, Teske E, Voorhout G, Galac S, Kooistra HS, Meij BP. Prognostic factors for outcome after transsphenoidal hypophysectomy in dogs with pituitary-dependent hyperadrenocorticism. J Neurosurg. 2007;107:830-40.
83. Lehner L, Czeibert K, Csöndes J, et al. Endoscope-guided transsphenoidal removal of a hypophyseal tumour in a dog. Case study. Magyar Állatorvosok Lapja. 2018;140:535-50. Available from: https://univet.hu/wp-content/uploads/2018/12/MAL-2018-09_content.pdf [Last accessed on 2 Jun 2026].
84. Escauriaza L, Fenn J, Mccue J, et al. A 3-dimensional printed patient-specific surgical guide to facilitate transsphenoidal hypophysectomy in dogs. Front Vet Sci. 2022;9:930856.
85. Roh Y, Kim D, Jeong S, Lee H. Evaluation of the accuracy of three-dimensionally printed patient-specific guides for transsphenoidal hypophysectomy in small-breed dogs. Am J Vet Res. 2022;83:465-72.
86. Santos ERDS, Viana FR, Gonçalves PE, Lima MAC, Lyra CAM, Santos BFDO. Precision in neuronavigation systems: a systematic review and meta-analysis. Arq Bras Neurocir. 2024;43:e325-36.
87. Owen TJ, Chen AV, Frey S, Martin LG, Kalebaugh T. Transsphenoidal surgery: accuracy of an image-guided neuronavigation system to approach the pituitary fossa (sella turcica). Vet Surg. 2018;47:664-71.
88. Van Rijn S, Galac S, Tryfonidou M, et al. The influence of pituitary size on outcome after transsphenoidal hypophysectomy in a large cohort of dogs with pituitary-dependent hypercortisolism. J Vet Intern Med. 2016;30:989-95.
89. Guignat L, Bertherat J. Long-term follow-up and predictors of recurrence of Cushing's disease. J Neuroendocrinol. 2022;34:e13186.
90. Balomenaki M, Vassiliadi DA, Tsagarakis S. Cushing’s disease: risk of recurrence following trans-sphenoidal surgery, timing and methods for evaluation. Pituitary. 2022;25:718-21.
91. Giustina A, Barkhoudarian G, Beckers A, et al. Multidisciplinary management of acromegaly: a consensus. Rev Endocr Metab Disord. 2020;21:667-78.
92. Law HA, Law AJ, Short TG, et al. Pituitary surgery in New Zealand: a single neurosurgeon case series of 1,224 operations. J Clin Neurosci. 2025;138:111388.
93. Fleseriu M, Biller BMK, Freda PU, et al. A pituitary society update to acromegaly management guidelines. Pituitary. 2020;24:1-13.
94. Fenn J, Kenny PJ, Scudder CJ, et al. Efficacy of hypophysectomy for the treatment of hypersomatotropism-induced diabetes mellitus in 68 cats. J Vet Intern Med. 2021;35:823-33.
95. Van Bokhorst KL, Galac S, Kooistra HS, et al. Evaluation of hypophysectomy for treatment of hypersomatotropism in 25 cats. J Vet Intern Med. 2021;35:834-42.
96. Janelle F, Blanquez-Yeste V, Tran T, et al. Challenges and opportunities for new intraoperative optical techniques in the surgical treatment of pituitary adenomas: a review. J Biomed Opt. 2025;30:080901.
97. Khan DZ, Valetopoulou A, Das A, et al. Artificial intelligence assisted operative anatomy recognition in endoscopic pituitary surgery. NPJ Digit Med. 2024;7:314.
98. Paul R, Johansson R, Kiuru A, et al. Imaging of canine cancers with 18F-2-fluoro-2-deoxy-D-glucose (FDG) suggests further applications for cancer imaging in man. Nucl Med Commun. 1984;5:641-6.
99. Son Y, Kim D, Kang J, et al. High-resolution fluorodeoxyglucose positron emission tomography and magnetic resonance imaging findings of a pituitary microtumor in a dog. Ir Vet J. 2015;68:22.
100. Hansen AE, Mcevoy F, Engelholm SA, Law I, Kristensen AT. FDG PET/CT imaging in canine cancer patients. Vet Radiol Ultrasound. 2010;52:201-6.
101. Yun T, Koo Y, Kim S, et al. Characteristics of 18F-FDG and 18F-FDOPA PET in an 8-year-old neutered male Yorkshire Terrier dog with glioma: long-term chemotherapy using hydroxyurea plus imatinib with prednisolone and immunoreactivity for PDGFR-β and LAT1. Vet Q. 2021;41:163-71.
102. Zhang J, Shi Z, Kang Y, Wu B, Liu X, Zhu H. The application of augmented reality technology in endoscopic pituitary adenoma surgery via nasal approach. Gland Surg. 2025;14:1318-35.
103. Gieger TL, Magestro L, Walz J, Yoshikawa H, Nolan MW. Outcomes of stereotactic radiation therapy versus fractionated radiation therapy in 44 dogs with pituitary masses: a multi-institutional retrospective study (2016-2022). Vet Comp Oncol. 2024;22:429-36.
104. Mondal SB, O’brien CM, Bishop K, Fields RC, Margenthaler JA, Achilefu S. Repurposing molecular imaging and sensing for cancer image-guided surgery. J Nucl Med. 2020;61:1113-22.
105. Litvack ZN, Zada G, Laws ER. Indocyanine green fluorescence endoscopy for visual differentiation of pituitary tumor from surrounding structures: Clinical article. J Neurosurg. 2012;116:935-41.
106. Olesrud I, Halvorsen IJ, Storaker MA, Heck A, Dahlberg D, Wiedmann MKH. Indocyanine green fluorescence in endoscopic transsphenoidal resection of pituitary neuroendocrine tumors: a systematic review. Acta Neurochir. 2025;167:92.
107. Vergeer RA, Theunissen REP, Van Elk T, et al. Fluorescence-guided detection of pituitary neuroendocrine tumor (PitNET) tissue during endoscopic transsphenoidal surgery available agents, their potential, and technical aspects. Rev Endocr Metab Disord. 2022;23:647-57.
108. Staartjes VE, Togni-Pogliorini A, Stumpo V, Serra C, Regli L. Impact of intraoperative magnetic resonance imaging on gross total resection, extent of resection, and residual tumor volume in pituitary surgery: systematic review and meta-analysis. Pituitary. 2021;24:644-56.
109. Wilkie N, Mcsorley G, Creighton C, Sanderson D, Muirhead T, Bressan N. Mixed reality for veterinary medicine: case study of a canine femoral nerve block. In: 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC); 2020 Jul 20-24; Montreal, QC, Canada; pp. 6074-7.
110. Aghapour M, Bockstahler B. State of the art and future prospects of virtual and augmented reality in veterinary medicine: a systematic review. Animals. 2022;12:3517.
111. Li C, Zheng Y, Yuan Y, Li H. Augmented reality navigation-guided pulmonary nodule localization in a canine model. Transl Lung Cancer Res. 2021;10:4152-60.
112. Shimada M, Kurihara K, Tsujii T. Prototype of an augmented reality system to support animal surgery using HoloLens 2. In: 2022 IEEE 4th Global Conference on Life Sciences and Technologies (LifeTech); 2022 Mar 7-9; Osaka, Japan; pp. 335-7.
113. Zhou C, Zhu M, Shi Y, et al. Robot-assisted surgery for mandibular angle split osteotomy using augmented reality: preliminary results on clinical animal experiment. Aesthetic Plast Surg. 2017;41:1228-36.
114. Hunt JA, Heydenburg M, Anderson SL, Thompson RR. Does virtual reality training improve veterinary students’ first canine surgical performance? Vet Rec. 2020;186:562.
115. Ioannou I, Kazmierczak E, Stern L. Comparison of oral surgery task performance in a virtual reality surgical simulator and an animal model using objective measures. In: 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC); 2015 Aug 25-29; Milan, Italy; pp. 5114-7.
116. Baskaran V, Štrkalj G, Štrkalj M, Di Ieva A. Current applications and future perspectives of the use of 3D printing in anatomical training and neurosurgery. Front Neuroanat. 2016;10:69.
117. Riutort KT, Clifton W, Damon A, Dove C, Clendenen SR. Construction of an affordable lumbar neuraxial block model using 3D printed materials. Cureus. 2019;11:e6033.
118. Pearce P, Novak J, Wijesekera A, et al. Properties and implementation of 3-dimensionally printed models in spine surgery: a mixed-methods review with meta-analysis. World Neurosur. 2023;169:57-72.
119. Vakharia VN, Vakharia NN, Hill CS. Review of 3-dimensional printing on cranial neurosurgery simulation training. World Neurosur. 2016;88:188-98.
120. Khan DZ, Newall N, Koh CH, et al. Video-based performance analysis in pituitary surgery - part 2: artificial intelligence assisted surgical coaching. World Neurosur. 2024;190:e797-808.
121. Huang J, He R, Khan DZ, et al. Surgical AI copilot: energy-based fourier gradient low-rank adaptation for surgical LLM agent reasoning and planning. arXiv. 2025:arXiv:2503.09474.
122. Iqbal MJ, Javed Z, Sadia H, et al. Clinical applications of artificial intelligence and machine learning in cancer diagnosis: looking into the future. Cancer Cell Int. 2021;21:270.
123. Jones OT, Matin RN, Van Der Schaar M, et al. Artificial intelligence and machine learning algorithms for early detection of skin cancer in community and primary care settings: a systematic review. Lancet Digit Health. 2022;4:e466-76.
124. Liu J, Lei J, Ou Y, et al. Mammography diagnosis of breast cancer screening through machine learning: a systematic review and meta-analysis. Clin Exp Med. 2022;23:2341-56.
125. Kent MS, Rosseel M. Updates on radiation therapy for pituitary tumors. Vet Clin N Am Anim Pract. 2025;55:119-33.
126. Kent MS, Bommarito D, Feldman E, et al. Survival, neurologic response, and prognostic factors in dogs with pituitary masses treated with radiation therapy and untreated dogs. J Vet Intern Med. 2007;21:1027-33.
127. Brearley MJ, Polton GA, Littler RM, Niessen SJM. Coarse fractionated radiation therapy for pituitary tumours in cats: a retrospective study of 12 cases. Vet Comp Oncol. 2006;4:209-17.
128. de Fornel P, Delisle F, Devauchelle P, Rosenberg D. Effects of radiotherapy on pituitary corticotroph macrotumors in dogs: a retrospective study of 12 cases. Can Vet J. 2007;48:481-6.
129. Rapastella S, Morabito S, Sharman M, et al. Effect of pituitary-dependent hypercortisolism on the survival of dogs treated with radiotherapy for pituitary macroadenomas. J Vet Intern Med. 2023;37:1331-40.
130. Hansen KS, Zwingenberger AL, Théon AP, Kent MS. Long-term survival with stereotactic radiotherapy for imaging-diagnosed pituitary tumors in dogs. Vet Radiol Ultrasound. 2018;60:219-32.
131. Marcinowska A, Warland J, Brearley M, Dobson J. Comparison of two coarse fractionated radiation protocols for the management of canine pituitary macrotumor: an observational study of 24 dogs. Vet Radiol Ultrasound. 2015;56:554-62.
132. Kaser-Hotz B, Rohrer CR, Stankeova S, Wergin M, Fidel J, Reusch C. Radiotherapy of pituitary tumours in five cats. J Small Anim Pract. 2002;43:303-7.
133. Körner M, Roos M, Meier VS, et al. Radiation therapy for intracranial tumours in cats with neurological signs. J Feline Med Surg. 2018;21:765-71.
134. Mayer MN, Greco DS, LaRue SM. Outcomes of pituitary tumor irradiation in cats. J Vet Intern Med. 2006;20:1151-4.
135. Sellon R, Fidel J, Houston R, Gavin P. Linear-accelerator-based modified radiosurgical treatment of pituitary tumors in cats: 11 cases (1997-2008). J Vet Intern Med. 2009;23:1038-44.
136. Sawada H, Mori A, Lee P, Sugihara S, Oda H, Sako T. Pituitary size alteration and adverse effects of radiation therapy performed in 9 dogs with pituitary-dependent hypercortisolism. Res Vet Sci. 2018;118:19-26.
137. Goossens MMC, Feldman EC, Theon AP, Koblik PD. Efficacy of cobalt 60 radiotherapy in dogs with pituitary-dependent hyperadrenocorticism. J Am Vet Med Assoc. 1998;212:374-6.
138. Théon AP, Feldman EC. Megavoltage irradiation of pituitary macrotumors in dogs with neurologic signs. J Am Vet Med Assoc. 1998;213:225-31.
139. Wormhoudt TL, Boss M, Lunn K, et al. Stereotactic radiation therapy for the treatment of functional pituitary adenomas associated with feline acromegaly. J Vet Intern Med. 2018;32:1383-91.
140. Bley CR, Sumova A, Roos M, Kaser-Hotz B. Irradiation of brain tumors in dogs with neurologic disease. J Vet Intern Med. 2005;19:849-54.
141. Gieger TL, Nolan MW. Treatment outcomes and target delineation utilizing CT and MRI in 13 dogs treated with a uniform stereotactic radiation therapy protocol (16 Gy single fraction) for pituitary masses: (2014-2017). Vet Comp Oncol. 2020;19:17-24.
142. Mariani CL, Schubert TA, House RA, et al. Frameless stereotactic radiosurgery for the treatment of primary intracranial tumours in dogs. Vet Comp Oncol. 2013;13:409-23.
143. Park P, Chandler WF, Barkan AL, et al. The role of radiation therapy after surgical resection of nonfunctional pituitary macroadenomas. Neurosur. 2004;55:100-7.
144. Green S, Lehrer EJ, Cifarelli CP, et al. Congress of neurological surgeons systematic review and evidence-based guidelines for the role of radiosurgery for patients with functioning pituitary adenomas. Neurosurgery. 2025;97:S36-43.
145. Minniti G, Flickinger J. The risk/benefit ratio of radiotherapy in pituitary tumors. Best Pract Res Clin Endocrinol Metab. 2019;33:101269.
146. Morsink NC, Klaassen NJM, Meij BP, et al. Case report: radioactive holmium-166 microspheres for the intratumoral treatment of a canine pituitary tumor. Front Vet Sci. 2021;8:748247.
148. Kelsall A, Newell-Price J. Cushing's disease-from Minnie G to key issues in the early 21st century. Lancet Diabetes Endocrinol. 2019;7:959-64.
149. Luton JP, Mahoudeau JA, Bouchard P, et al. Treatment of Cushing's disease by o,p′DDD: survey of 62 cases. N Engl J Med. 1979;300:459-64.
150. Carmichael JD, Fleseriu M. Mifepristone: is there a place in the treatment of Cushing’s disease? Endocrine. 2012;44:20-32.
151. Schofield I, Brodbelt DC, Wilson ARL, et al. Survival analysis of 219 dogs with hyperadrenocorticism attending primary care practice in England. Vet Rec. 2020;186:333-60.
152. Patel J, Eloy JA, Liu JK. Nelson's syndrome: a review of the clinical manifestations, pathophysiology, and treatment strategies. Neurosurg Focus. 2015;38:E14.
153. Teshima T, Hara Y, Takekoshi S, et al. Trilostane-induced inhibition of cortisol secretion results in reduced negative feedback at the hypothalamic–pituitary axis. Domest Anim Endocrinol. 2009;36:32-44.
154. Fracassi F, Corradini S, Floriano D, et al. Prognostic factors for survival in dogs with pituitary-dependent hypercortisolism treated with trilostane. Vet Rec. 2015;176:49.
155. Galac S, Buijtels JJ, Mol JA, Kooistra HS. Effects of trilostane on the pituitary-adrenocortical and renin–aldosterone axis in dogs with pituitary-dependent hypercortisolism. Vet J. 2010;183:75-80.
156. García San José P, Arenas Bermejo C, Alonso-Miguel D, et al. Survival of dogs with pituitary-dependent hyperadrenocorticism treated twice daily with low doses of trilostane. Vet Rec. 2022;191:e1630.
157. Nagata N, Kojima K, Yuki M. Comparison of survival times for dogs with pituitary-dependent hyperadrenocorticism in a primary-care hospital: treated with trilostane versus untreated. J Vet Intern Med. 2017;31:22-8.
158. De Bruin C, Hanson JM, Meij BP, et al. Expression and functional analysis of dopamine receptor subtype 2 and somatostatin receptor subtypes in canine cushing’s disease. Endocrinology. 2008;149:4357-66.
159. Castillo V, Gómez N, Lalia J, Cabrera Blatter M, García J. Cushing’s disease in dogs: cabergoline treatment. Res Vet Sci. 2008;85:26-34.
160. Scudder CJ, Hazuchova K, Gostelow R, et al. Pilot study assessing the use of cabergoline for the treatment of cats with hypersomatotropism and diabetes mellitus. J Feline Med Surg. 2020;23:131-7.
161. Miceli DD, García JD, Pompili GA, et al. Cabergoline treatment in cats with diabetes mellitus and hypersomatotropism. J Feline Med Surg. 2022;24:1238-44.
162. Golinelli S, Fracassi F, Pöppl AG, et al. Addition of cabergoline to trilostane treatment for dogs with pituitary-dependent hypercortisolism. J Vet Intern Med. 2024;38:1-864. Available from: https://cris.unibo.it/handle/11585/955590 [Last accessed on 12 Jun 2026].
163. Weckbecker G, Briner U, Lewis I, Bruns C. SOM230: a new somatostatin peptidomimetic with potent inhibitory effects on the growth hormone/insulin-like growth factor-I axis in rats, primates, and dogs. Endocrinology. 2002;143:4123-30.
164. Castillo V, Theodoropoulou M, Stalla J, et al. Effect of SOM230 (Pasireotide) on corticotropic cells: action in dogs with Cushing’S disease. Neuroendocrinology. 2011;94:124-36.
165. Lottati M, Bruyette DS. Outcomes of the addition of pasireotide to traditional adrenal-directed treatment for dogs with pituitary-dependent hyperadrenocorticism secondary to macroadenoma: 9 cases (2013-2015). J Am Vet Med Assoc. 2018;252:1403-8.
166. Jaquet P, Gunz G, Saveanu A, et al. Efficacy of chimeric molecules directed towards multiple somatostatin and dopamine receptors on inhibition of GH and prolactin secretion from GH-secreting pituitary adenomas classified as partially responsive to somatostatin analog therapy. Eur J Endocrinol. 2005;153:135-41.
167. Castillo V, Giacomini D, Páez-Pereda M, et al. Retinoic acid as a novel medical therapy for Cushing’S disease in dogs. Endocrinology. 2006;147:4438-44.
168. Occhi G, Regazzo D, Albiger NM, et al. Activation of the dopamine receptor type-2 (DRD2) promoter by 9-cis retinoic acid in a cellular model of Cushing's disease mediates the inhibition of cell proliferation and ACTH secretion without a complete corticotroph-to-melanotroph transdifferentiation. Endocrinology. 2014;155:3538-49.
169. Vilar L, Albuquerque JL, Lyra R, et al. The role of isotretinoin therapy for Cushing’s disease: results of a prospective study. Int J Endocrinol. 2016;2016:1-9.
170. Young RB, Bryson MJ, Sweat ML, Street JC. Complexing of DDT and o,p'DDD with adrenal cytochrome P-450 hydroxylating systems. J Steroid Biochem. 1973;4:585-91.
171. Kroiss M, Quinkler M, Lutz WK, Allolio B, Fassnacht M. Drug interactions with mitotane by induction of CYP3A4 metabolism in the clinical management of adrenocortical carcinoma. Clin Endocrinol. 2011;75:585-91.
172. Sbiera S, Leich E, Liebisch G, et al. Mitotane inhibits sterol-o-Acyl transferase 1 triggering lipid-mediated endoplasmic reticulum stress and apoptosis in adrenocortical carcinoma cells. Endocrinology. 2015;156:3895-908.
173. King J, Morton J. Incidence and risk factors for hypoadrenocorticism in dogs treated with trilostane. Vet J. 2017;230:24-9.
174. Fleseriu M, Castinetti F. Updates on the role of adrenal steroidogenesis inhibitors in Cushing’s syndrome: a focus on novel therapies. Pituitary. 2016;19:643-53.
175. Daniel E, Aylwin S, Mustafa O, et al. Effectiveness of metyrapone in treating Cushing's syndrome: a retrospective multicenter study in 195 patients. J Clin Endocrinol Metab. 2015;100:4146-54.
176. Newell-Price J, Fleseriu M, Pivonello R, et al. Improved clinical outcomes during long-term osilodrostat treatment of cushing disease with normalization of late-night salivary cortisol and urinary free cortisol. J Endocr Soc. 2025;9:bvae201.
177. Feelders RA, Hofland LJ, De Herder WW. Medical treatment of cushing’s syndrome: adrenal-blocking drugs and ketaconazole. Neuroendocrinology. 2010;92:111-5.
178. Muthukuda DT, Liyanaarachchi KD, Jayawickreme KP, et al. Etomidate in severe cushing syndrome: a systematic review. J Endocr Soc. 2025;9:bvaf039.
179. Mountjoy KG, Robbins LS, Mortrud MT, Cone RD. The cloning of a family of genes that encode the melanocortin receptors. Science. 1992;257:1248-51.
180. Sanders K, Mol JA, Kooistra HS, Galac S. Melanocortin 2 receptor antagonists in canine pituitary-dependent hypercortisolism: in vitro studies. Vet Res Commun. 2018;42:283-8.
181. Schimmer BP, White PC. Minireview: steroidogenic factor 1: its roles in differentiation, development, and disease. Mol Endocrinol. 2010;24:1322-37.
182. Sanders K, Mol J, Slob A, Kooistra H, Galac S. Steroidogenic factor-1 inverse agonists as a treatment option for canine hypercortisolism: in vitro study. Domest Anim Endocrinol. 2018;63:23-30.
183. Brown DR, East HE, Eilerman BS, et al. Clinical management of patients with Cushing syndrome treated with mifepristone: consensus recommendations. Clin Diabetes Endocrinol. 2020;6:18.
185. Castinetti F, Fassnacht M, Johanssen S, et al. Merits and pitfalls of mifepristone in Cushing's syndrome. Eur J Endocrinol. 2009;160:1003-10.
186. Van Stee L. The growth inhibitory effect of of anti growth hormone (G144K) on canine mammary carcinomasDSpace/Manakin Repository. Available from: https://research-portal.uu.nl/en/publications/the-growth-inhibitory-effect-of-of-anti-growth-hormone-g144k-on-c/ [Last accessed on 12 Jun 2026].
187. Lien Y, Huang H. Use of ketoconazole to treat dogs with pituitary-dependent hyperadrenocorticism: 48 cases (1994-2007). J Am Vet Med Assoc. 2008;233:1896-901.
188. Slingerland L, Voorhout G, Rijnberk A, Kooistra H. Growth hormone excess and the effect of octreotide in cats with diabetes mellitus. Domest Anim Endocrinol. 2008;35:352-61.
189. Scudder CJ, Gostelow R, Forcada Y, Schmid HA, Church D, Niessen SJ. Pasireotide for the medical management of feline hypersomatotropism. J Vet Intern Med. 2015;29:1074-80.
190. Gostelow R, Scudder C, Keyte S, et al. Pasireotide long-acting release treatment for diabetic cats with underlying hypersomatotropism. J Vet Intern Med. 2017;31:355-64.
191. Ay SS, Aslan S, Önyay F, et al. Effect of oral misoprostol, alone or in combination with aglepristone, on mid-term pregnancy termination in cats. J Feline Med Surg. 2018;21:714-22.
192. Concannon PW, Yeager A, Frank D, Iyampillai A. Termination of pregnancy and induction of premature luteolysis by the antiprogestagen, mifepristone, in dogs. Reproduction. 1990;88:99-104.
193. Dijkstra KK, Van Den Berg JG, Weeber F, et al. Patient-derived organoid models of human neuroendocrine carcinoma. Front Endocrinol. 2021;12:627819.
194. Van Den Berg MF, Timmermans-Sprang EPM, Viets FC, et al. Canine adrenomedullary and pheochromocytoma organoids: a novel in vitro model. Endocrinology. 2025;166:bqaf114.
195. Ginai M, Elsby R, Hewitt CJ, Surry D, Fenner K, Coopman K. The use of bioreactors as in vitro models in pharmaceutical research. Drug Discov Today. 2013;18:922-35.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Special Topic
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].