


Primary sclerosing encapsulating peritonitis with cryptorchidism in an older man: case report and literature review
 0
0 Abstract
We report a case of primary sclerosing encapsulating peritonitis (SEP) in a 70-year-old male, initially presenting as recurrent incomplete intestinal obstruction. Concomitant cryptorchidism was consistent with an underlying developmental cause. The patient also had subclinical type A atrophic gastritis and hypothyroidism. The diagnosis of primary SEP requires the exclusion of secondary causes and relies on a synthesis of imaging, surgical, and pathological findings. The patient underwent successful surgical intervention, including adhesion lysis and partial ileocecal resection, resulting in symptomatic relief and a favorable recovery. Primary SEP is a rare condition with non-specific symptoms, predominantly intestinal obstruction, making preoperative diagnosis difficult and misdiagnosis common. Heightened awareness and meticulous imaging analysis are essential for timely and accurate diagnosis.
Keywords
INTRODUCTION
Sclerosing encapsulating peritonitis (SEP) is a rare chronic fibroinflammatory condition of the peritoneum[1,2] and an uncommon cause of intestinal obstruction. Its etiology remains unclear but has been associated with various factors, including developmental anomalies, gender, intraperitoneal chemotherapy, beta-blocker use, chronic peritoneal dialysis, liver cirrhosis, tuberculosis, neoplasms, shunt or bypass surgery, liver transplantation, and autoimmune diseases[3-12]. Due to its low incidence and lack of specific clinical features—typically presenting as recurrent partial or complete intestinal obstruction—SEP often poses diagnostic challenges, leading to difficult preoperative identification and a high rate of misdiagnosis. In the present case, after excluding infectious, drug-related, peritoneal dialysis-related, neoplastic, amyloidosis, and autoimmune causes, along with a comprehensive analysis of preoperative imaging, intraoperative laparotomy findings, and postoperative pathology, the patient was diagnosed with primary SEP (also called “abdominal cocoon”) and concomitant cryptorchidism. The coexisting cryptorchidism suggested an underlying developmental cause, given that embryonic fibrotic processes may lead to both widespread peritoneal adhesions and disrupt testicular descent[13]. It was unclear whether the coexisting atrophic gastritis and subclinical hypothyroidism contributed to the patient’s clinical presentation or complicated the management of the primary disease. It was noted that the Type A atrophic gastritis and subclinical hypothyroidism observed in this patient were likely incidental autoimmune comorbidities rather than direct complications of SEP.
Cases of SEP were originally reported in adolescent girls, but have subsequently been described in younger men, often in tropical and subtropical environments. To our knowledge, SEP has not been previously reported in an older man with a delayed diagnosis of cryptorchidism.
CASE HISTORY & EXAMINATION
A 70-year-old male patient was admitted to the Department of Gastroenterology on December 6, 2024, due to recurrent abdominal distension and pain accompanied by nausea and vomiting for three months. The symptoms began in August 2024 without an identifiable cause, were primarily localized around the umbilicus, and presented as paroxysmal colic that did not radiate to the lumbodorsal region and were exacerbated after meals. Each episode lasted from several minutes to over ten minutes and was accompanied by nausea and vomiting of gastric contents, which were non-projectile. There was no hematemesis, diarrhea, hematochezia, chills, or fever. The patient had sought treatment at several local hospitals. Gastroscopy showed no significant abnormalities, while abdominal Computed Tomography (CT) indicated incomplete small bowel obstruction. The clinical diagnosis was incomplete small intestinal obstruction. He received unspecified Western and traditional Chinese medications, yet his paroxysmal abdominal pain persisted. On December 3, 2024, he was admitted to another hospital. A plain CT scan of the abdomen and pelvis revealed dilation of the jejunum and proximal ileum, edema and wall thickening of some small bowel loops in the left upper abdomen, multiple enlarged lymph nodes at the mesenteric root, and fluid accumulation in the abdomen and pelvis, suggesting incomplete intestinal obstruction. The patient was subsequently transferred to our hospital for further management and was admitted with the outpatient diagnosis of abdominal pain and vomiting under investigation. His past medical history included two inguinal hernia repairs. As these procedures were confined to the extraperitoneal inguinal region, a causal relationship with the subsequent development of SEP was deemed unlikely. He reported no smoking or alcohol use and denied a history of hypertension, diabetes, or special drug use.
Vital signs on admission were within normal limits: temperature 36.8 ℃, respirations 20 breaths/min, pulse 87 bpm, and blood pressure 90/68 mmHg. He appeared emaciated and poorly nourished, with no jaundice or petechiae on the skin or mucous membranes. Cardiopulmonary auscultation was unremarkable. The abdomen was slightly distended with visible intestinal patterns and peristaltic waves, and loss of the subcutaneous fat pad. Palpation revealed a soft abdomen with periumbilical tenderness but no rebound tenderness, hepatosplenomegaly, or shifting dullness. Mild edema was noted in both lower extremities.
The results of the laboratory tests were summarized in Table 1. Blood chemistry and hematological testing were largely unremarkable except for mild non-regenerative anemia (hemoglobin, 92 g/L) and hypoalbuminemia (albumin, 25.1 g/L), findings most likely attributable to the patient’s subclinical hypothyroidism and chronic intestinal disease.
The tested parameters of the patient
| Laboratory examinations | Parameter | Value | Unit | Reference value |
| Blood routine | White blood cell count | 4.35 | 109/L | 4.0-10 |
| Neutrophil ratio | 53.8 | % | 50-70 | |
| Red blood cell count | 2.89 | 1012/L | 3.5-5.5 | |
| Hemoglobin | 92 | g/L | 120-160 | |
| Hematocrit | 26.0 | % | 35-50 | |
| Platelet | 163 | 109/L | 100-300 | |
| Biochemical data | Total protein | 48.0 | g/L | 60-80 |
| Albumin | 25.1 | g/L | 35-55 | |
| Globulin | 22.9 | g/L | 20-30 | |
| Potassium | 3.4 | mmol/L | 3.5-5.5 | |
| Total bilirubin | normal | / | / | |
| Calcium | 1.93 | mmol/L | 2.25-2.58 | |
| Serum gastrin | 888 | ng/L | 15-105 | |
| Other results | IgG and IgM | normal | / | / |
| IgA | 639.0 | mg/dL | 76-390 | |
| Free triiodothyronine | 1.57 | pg/mL | 2.3-4.2 | |
| TSH | 6.893 | μIU/mL | 0.35-4.94 | |
| TSH (retest) | 12.653 | μIU/mL | 0.35-4.94 | |
| PGI | 80.51 | μg/L | 70-165 | |
| PGII | 11.04 | μg/L | 3-15 |
An electrocardiogram showed no significant abnormalities. A plain abdominal radiograph revealed findings suggestive of incomplete intestinal obstruction. Thyroid ultrasonography was reported as category 1. Gastroscopy revealed reflux esophagitis (Los Angeles grade B), suspected type A atrophic gastritis, and localized antral erosion; the 13C-urea breath test was negative. Histopathological examination of the gastric antrum indicated superficial gastritis with mild inflammation (+), no activity (-), no intestinal metaplasia, and Contrast-enhanced abdominal CT, no dysplasia; the gastric body showed mild atrophic gastritis with inflammation (+), activity (+), no intestinal metaplasia, and no dysplasia. Contrast-enhanced chest CT showed minor fibrotic lesions in both lungs and calcification of the aorta and coronary arteries. Contrast-enhanced abdominal CT suggested changes consistent with an abdominal cocoon (sclerosing encapsulating peritonitis) complicated by low-grade incomplete intestinal obstruction [Figure 1]. Consequently, the diagnoses of incomplete small intestinal obstruction, hypoalbuminemia, type A atrophic gastritis, and subclinical hypothyroidism were established, with no other autoimmune comorbidities identified; however, abdominal cocoon was suggested as a possible cause of the obstruction.
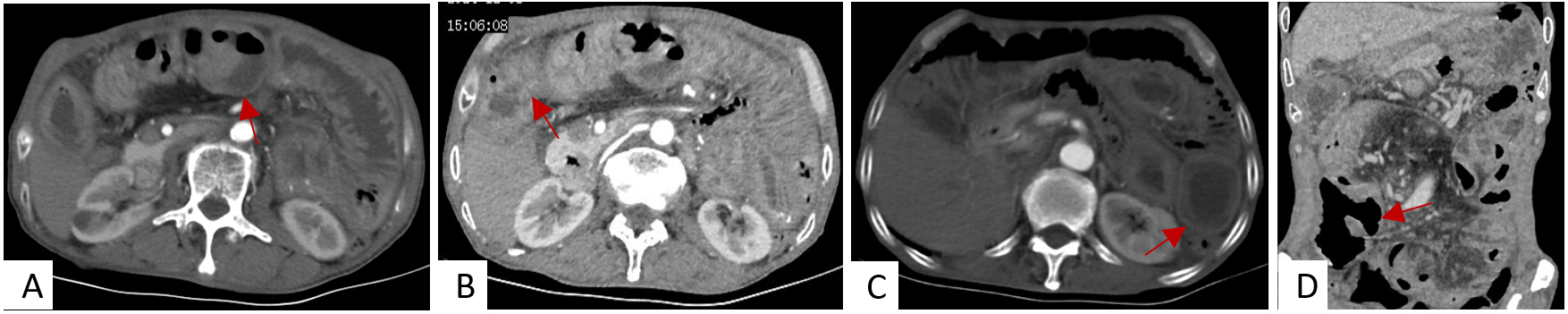
Figure 1. Contrast-enhanced CT of the abdomen shows thickening and dilatation of the small intestinal wall in the right middle and lower abdomen. The contrast-enhanced scan reveals obvious enhancement of the encapsulated intestinal tube, with a strip-like peritoneal shadow surrounding it. These findings are consistent with abdominal cocoon with low-grade incomplete intestinal obstruction. (A-C): axial view, (D): coronal view, the arrow indicated the abnormality.
As his symptoms did not improve with conservative medical management, a multidisciplinary consultation recommended exploratory laparotomy, which was performed on December 17, 2024. Intraoperative findings included 300 mL of clear yellow ascites. The liver, gallbladder, stomach, spleen, transverse colon, descending colon, and sigmoid colon appeared normal, with no significant adhesions in the upper abdomen and a normal greater omentum. The entire small intestine was dilated, measuring approximately 250 cm in length. The upper jejunum was slightly dilated with mild wall thickening, and the bowel gradually became more dilated distally with progressive wall thickening. Approximately 40 cm of the distal ileum had a thickened, rigid wall with a pale surface and a maximum diameter of about 6 cm. The mesentery of this segment was thickened, and the serosa of both the intestine and mesentery was thickened and covered by a dense, white fibrous capsule, with no obvious peristalsis [Figure 2]. About 30 cm of the terminal ileum was densely adherent to the right lower quadrant abdominal wall, and the cecum and ascending colon were adherent to the posterolateral aspect of the terminal ileal mesentery. The planned procedure was lysis of adhesion combined with partial ileal and cecal resection and anastomosis. During the operation, an undescended testis was identified in the right lower quadrant retroperitoneum, presenting as a mass measuring approximately

Figure 2. Intraoperative photograph showing a segment of the distal ileum. The intestinal wall is thickened and stiff, with a pale serosal surface. The affected small intestine and its mesentery appear to be encased in a whitish membranous capsule. No obvious peristalsis is observed in this segment.
Postoperative pathological examination of the resected ileum and cecum revealed chronic inflammation, mild reduction of intrinsic intestinal glands, and no evidence of ulceration. Extensive fibrous hyperplasia and hyaline degeneration were observed, and lymphocytic infiltration with other inflammatory exudates was present in some areas of fibro-hyaline change. No granulomas or multinucleated giant cells were identified despite extensive sampling, findings consistent with abdominal cocoon [Figure 3]. The appendix and ileocecal mesenteric lymph nodes showed chronic inflammation. Postoperative pathological examination of the cryptorchidism specimen revealed reduced seminiferous tubules with degeneration, atrophy, and loss of most spermatogenic cells, absence of sperm in the lumen, thickened basement membranes, and interstitial edema, consistent with cryptorchidism.
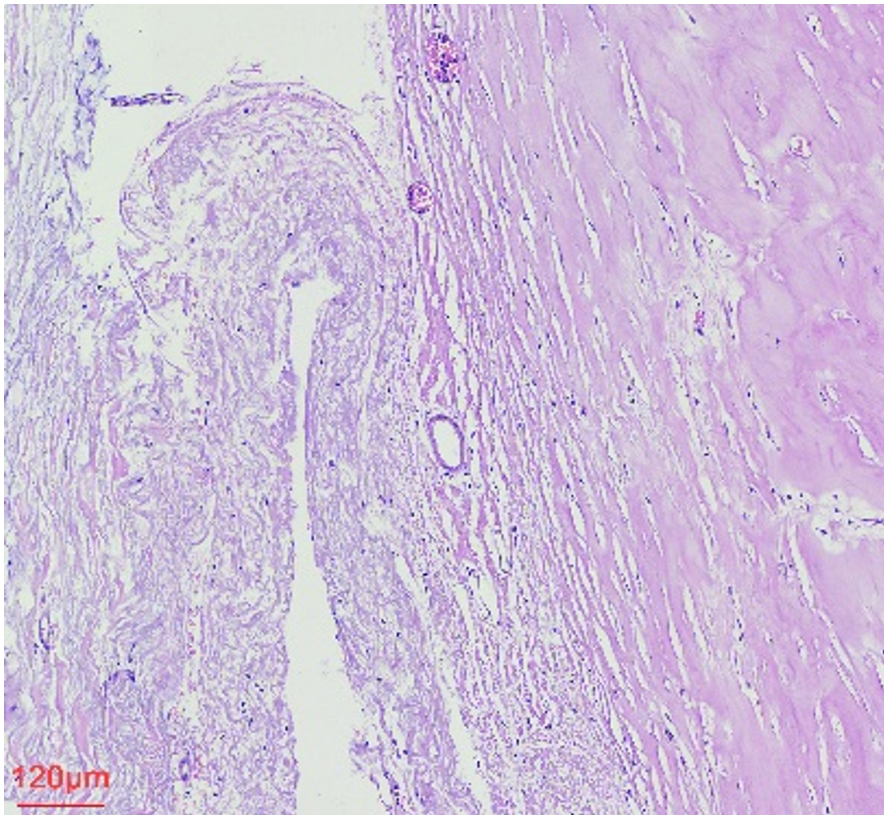
Figure 3. HE staining revealed extensive fibrous hyperplasia and hyaline degeneration (10×). In some areas, this was accompanied by lymphocytic and other inflammatory exudation.
After excluding infectious (e.g., tuberculosis), drug-related (e.g., chemotherapy, beta-blockers), peritoneal dialysis-related, neoplastic, amyloidosis, and autoimmune etiologies, the final diagnosis was incomplete small intestinal obstruction caused by primary sclerosing encapsulating peritonitis. Right cryptorchidism, discovered intraoperatively and confirmed by pathology, was identified as a comorbidity. Based on a comprehensive analysis of the medical history, laboratory data, imaging features, intraoperative findings, and postoperative pathology, the patient was diagnosed with primary sclerosing encapsulating peritonitis complicated by cryptorchidism, which was highly likely attributed to congenital developmental abnormalities. Gastroscopy revealed thinning of the gastric body mucosa along the greater curvature with visible vessels and localized antral erosion. Pathology confirmed mild atrophic gastritis in the gastric body and superficial gastritis in the antrum, which, together with hypergastrinemia and hypopepsinogenemia, supported the diagnosis of type A atrophic gastritis. Concurrently, thyroid function tests showed decreased free triiodothyronine and elevated thyroid-stimulating hormone, while thyroid ultrasound revealed no significant nodules or structural abnormalities, consistent with subclinical hypothyroidism. Given the absence of symptoms related to type A atrophic gastritis and subclinical hypothyroidism, no specific treatment was initiated. Given the recurrent intestinal obstruction and clear surgical indications, lysis of adhesions combined with partial ileal and cecal resection and anastomosis was performed after obtaining informed consent from the family.
OUTCOME & FOLLOW-UP
At the six-month postoperative evaluation, the patient’s symptoms had resolved, and he was noted to have recovered well without significant discomfort at the most recent follow-up.
DISCUSSION
SEP is a rare chronic fibroinflammatory disease of the peritoneum and a rare cause of intestinal obstruction. SEP is extremely rare clinically[14]. Its etiology is considered to likely involve congenital developmental abnormalities, given the shared embryonic origin of the urogenital system and adjacent abdominal/pelvic walls. Secondary SEP, by contrast, is more commonly encountered[15]. Its etiology and pathogenesis remain poorly understood, but may be associated with congenital developmental abnormalities, gender, region, drugs (intraperitoneal chemotherapy, beta-blockers, fungi), chronic peritoneal dialysis, liver cirrhosis, tuberculosis, tumors, shunt or bypass surgery, living donor liver transplantation, autoimmune diseases (systemic lupus erythematosus, Sjögren’s syndrome, IgG4-related sclerosing encapsulating peritonitis) and other factors[3-12]. This disease has a low incidence, mostly occurring in adolescent females, with a male/female ratio of 1:5.8, the peak age is 16-48 years old, and 80% are under 25 years old[16]. Studies have shown[17] that the median age of primary SEP patients is 48 (29-69) years old, and the median age of secondary SEP patients is 34.5 (24-64) years old. There are few reports of primary SEP in elderly individuals, and the few that exist are limited to sporadic case reports. The present case, involving an elderly patient, underscores the rarity of this condition in this age group. Clinical manifestations are recurrent intestinal obstruction symptoms, including abdominal distension, abdominal pain, vomiting, anorexia and weight loss, which are usually non-specific. Some patients may have bloody ascites, fever, elevated C-reactive protein and hypoalbuminemia. Clinical classification[16]: simple small intestinal encapsulation, which is common clinically, divided into partial small intestinal encapsulation and total small intestinal encapsulation; non-hollow organ encapsulation such as liver, spleen, uterus and its appendages; multi-organ encapsulation such as stomach, colon, liver, spleen, uterus and its appendages, bladder, etc.
Imaging examination, especially enhanced CT scan, is the most effective method for preoperative diagnosis of SEP[16,17]. It requires experienced radiologists to read the films to have high diagnostic significance. It is often manifested as small intestines clustered together, surrounded by low-density fibrous encapsulation, presenting as cocoon-like or crescent-shaped. Enhanced scan shows obvious enhancement of the encapsulated intestinal tubes, which is the most characteristic manifestation for the diagnosis of SEP[16,18]. Laparoscopy or surgical exploration finding that the intestinal tube is encapsulated by fibrosis to form a “cocoon” shape is the gold standard for the diagnosis of SEP[19,20]. Postoperative histopathology showing fibrous tissue hyperplasia accompanied by hyaline degeneration on the serosal surface of the small intestine can confirm the diagnosis[21]. The symptoms, signs, and laboratory findings of SEP are nonspecific, making preoperative diagnosis challenging. Preoperative imaging diagnosis is therefore essential to reduce the risk of misdiagnosis and missed diagnosis.
Management of SEP depends on the underlying etiology, with surgical excision of the fibrous membrane often proving effective. Asymptomatic patients do not need surgical treatment. Conservative treatment includes fasting, gastrointestinal decompression, parenteral or enteral nutrition, somatostatin, etc., while eliminating the inducing factors of secondary causes. For patients with primary SEP who have recurrent intestinal obstruction or ineffective conservative treatment, most scholars advocate surgical treatment, using outer membrane dissection and intestinal adhesion lysis. The postoperative prognosis for patients with SEP is generally favorable, with complete recovery typically attained by excision of the fibrous membrane and adhesiolysis[13]. Additional evaluation for potential secondary causes[3,5,9,22-31] was unrevealing in this patient. The coexistence of SEP and type A atrophic gastritis initially raised suspicion for an underlying autoimmune process, but this was not supported by subsequent laboratory and clinical data. The gastritis was ultimately regarded as an incidental, subclinical finding. In summary, this case was diagnosed as primary sclerosing encapsulating peritonitis with cryptorchidism, type A atrophic gastritis, and subclinical hypothyroidism.
DECLARATIONS
Authors’ contributions
Conceptualization, data curation, project administration: Chen Y
Investigation, supervision, validation: Wang Z
Investigation, writing - original draft: Han M
Conceptualization, project administration, supervision: Yan Z, Liu Y
Project administration, supervision, validation, visualization: Guo Y, Xie W, Zhou H
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
AI and AI-assisted tools statement
Not applicable.
Financial support and sponsorship
This work was supported by the Hengyang Guiding Plan Project (Hyzdxjh202203).
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
This case report has been reviewed by the Ethics Committee of the 922 Hospital of the Joint Logistics Support Force of the Chinese People’s Liberation Army and was granted exemption from formal ethical approval. Informed consent from the patient was obtained.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Vipudhamorn W, Juthasilaparut T, Sutharat P, et al. Unraveling the enigma of sclerosing encapsulating peritonitis: a comprehensive review. Ann Coloproctol. 2025;41:175-89.
2. Mekann Bouv-Hez M, Charissoux A, Bouvier S, Mathonnet M, Christou N. From abdominal pain to a diagnosis of primary sclerosing encapsulating peritonitis and its management, a case report. Acta Chir Belg. 2021;122:420-3.
3. Kang D, Sun L, Zhang X. Research progress of tamoxifen in the treatment of encapsulated peritoneal sclerosis. New Med. 2024;55:30-4. Available from: https://qikan.cqvip.com/Qikan/Article/Detail?id=7111267754 [Last accessed on 3 Jun 2026].
4. Mccrory MA, Heard MA, Wright JG, Roche KF. Sclerosing encapsulating peritonitis: a rare cause of bowel obstruction. Am Surg. 2023;89:3496-8.
5. Gupta S, Woodrow G. Successful treatment of fulminant encapsulating peritoneal sclerosis following fungal peritonitis with tamoxifen. Clin Nephrol. 2007;68:125-9.
6. Kim BS, Choi HY, Ryu D, et al. Clinical characteristics of dialysis related sclerosing encapsulating peritonitis: multi-center experience in Korea. Yonsei Med J. 2005;46:104.
7. Aliyev V, Yagi S, Hammad A, et al. Sclerosing encapsulating peritonitis after living-donor liver transplantation: a case series, Kyoto experience. Ann Hepatobiliary Pancreat Surg. 2018;22:144.
8. Ni Z, Chen Q, Huang C, Wang S, Huang Q. Sclerosing encapsulating peritonitis as a rare cause of intestinal obstruction after the treatment of peritoneal mesothelioma: a case report and review of the literature. Transl Cancer Res TCR. 2021;10:3074-80.
9. Ayoub M, Ouazni M, Achraf M, Sanae A, Mehdi S. Surgical management of sclerosing encapsulating peritonitis (SEP) secondary to tuberculosis: a case report and review of the literature. Int J Surg Case Rep. 2024;115:109292.
10. Osama M, Roy S, Rawat S, Rao S. IgG4 related sclerosing encapsulating peritonitis with cocoon formation: an unusual and undescribed presentation. Indian J Pathol Microbiol. 2022;65:683.
11. Koak Y, Gertner D, Forbes A, Ribeiro BF. Idiopathic sclerosing peritonitis. Eur J Gastroenterol Hepatol. 2008;20:148-50.
12. Mishra S, Chaudhary K, Tyagi S, Mishra P, Misra V. Primary sclerosing encapsulating peritonitis. Indian J Pathol Microbiol. 2023;67:182-4.
13. Yue B, Cui Z, Kang W, et al. Abdominal cocoon with bilateral cryptorchidism and seminoma in the right testis: a case report and review of literature. BMC Surg. 2019;19:167.
14. Alsadery HA, Busbait S, Alblowi A, Alsawidan M, Albisher HM, Alshammary S. Abdominal cocoon syndrome (idiopathic sclerosing encapsulating peritonitis): an extremely rare cause of small bowel obstruction—Two case reports and a review of literature. Front Med. 2022;9:1003775.
15. Machado NO. Sclerosing encapsulating peritonitis: review. Sultan Qaboos Univ Med J. 2016;16:e142-51.
16. Gao Q, Liang C, Liu Z. Clinical characteristics and imaging diagnosis of primary sclerosing encapsulating peritonitis. Int J Med Radiol. 2008;31:251-2.
17. Bozan MB, Kanat BH, Yazar FM, et al. A diagnostic dilemma for acute abdomen: sclerosing encapsulating peritonitis (abdominal cocoon syndrome); A retrospective cohort study. Arch Iran Med. 2021;24:447-52.
18. Duman E, Aslan A, Gunduz N, Inan I. Sclerosing encapsulated peritonitis: typical imaging findings for easy diagnosis. Ann Saudi Med. 2018;38:230-2.
19. Xu J, Wu X, Liu Ji, et al. Surgical treatment of 7 cases of sclerosing encapsulated peritonitis. Chin J Curr Adv Gen Surg. ;25:417-20. Available from: http://dianda.cqvip.com/Qikan/Article/Detail?id=7107328232 [Last accessed on 3 Jun 2026].
20. Wei F, Lin Z. Pay attention to the prevention and treatment of encapsulated sclerosing peritonitis. J Clin Nephrol. 2012;12:342-4.
21. Cheng B, Zhao D, Wu Y. Clinical characteristics and progress in diagnosis and treatment of abdominal cocoon. Chin J Dig. 2012;32:68-70.
22. Bozkurt D, Cetin P, Sipahi S, et al. The effects of renin-angiotensin system inhibition on regression of encapsulating peritoneal sclerosis. Perit Dial Int. 2008;28:S38-42.
23. Koçak G, Azak A, Astarcı HM, et al. Effects of renin‐angiotensin‐aldosterone system blockade on chlorhexidine gluconate‐induced sclerosing encapsulated peritonitis in rats. Ther Apher Dial. 2012;16:75-80.
24. Wong CF, Beshir S, Khalil A, et al. Successful treatment of encapsulating peritoneal sclerosis with azathioprine and prednisolone. Perit Dial Int. 2005;25:285-7.
25. Bozkurt D, Sipahi S, Cetin P, et al. Does immunosuppressive treatment ameliorate morphology changes in encapsulating peritoneal sclerosis? Perit Dial Int. 2009;29:S206-10.
26. Lafrance J, Létourneau I, Ouimet D, et al. Successful treatment of encapsulating peritoneal sclerosis with immunosuppressive therapy. Am J Kidney Dis. 2008;51:e7-10.
27. Mondello S, Mazzon E, Di Paola R, et al. Thalidomide suppresses sclerosing encapsulating peritonitis in a rat experimental model. Shock. 2009;32:332-9.
28. Sachdev A, Usatoff V, Thaow C. Sclerosing encapsulating peritonitis and methotrexate. Aust N Z J Obstet Gynaecol. 2006;46:58-9.
29. Bozkurt D, Bicak S, Sipahi S, et al. The effects of colchicine on the progression and regression of encapsulating peritoneal sclerosis. Perit Dial Int. 2008;28:S53-7.
30. Duman S, Bozkurt D, Sipahi S, et al. Effects of everolimus as an antiproliferative agent on regression of encapsulating peritoneal sclerosis in a rat model. Adv Perit Dial. 2008;24:104-10.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].