


Sex and age genetic overlap between body mass index and attention deficit hyperactivity disorder in twins
 0
0 Abstract
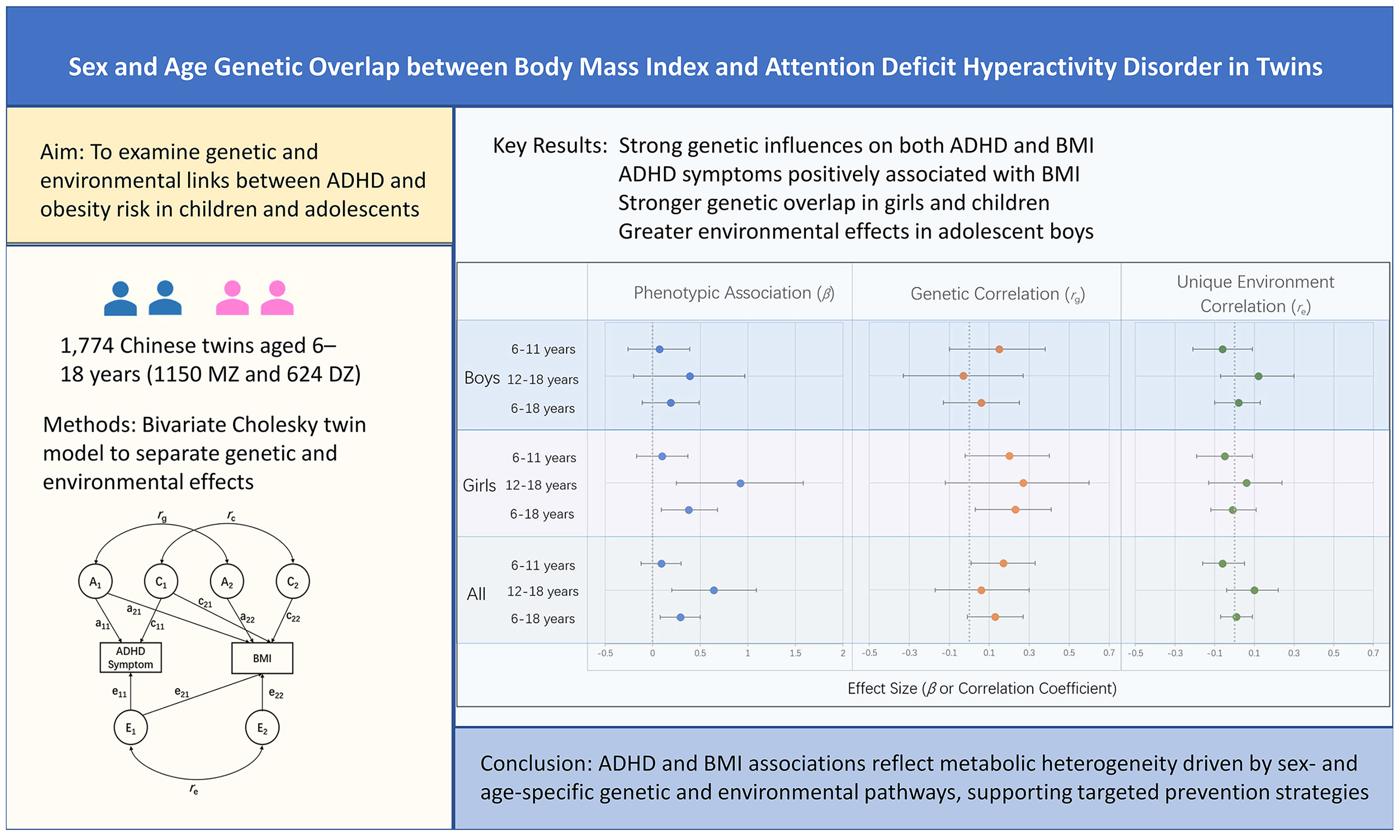
Aim: To examine the genetic and environmental contributions to the association between attention-deficit/hyperactivity disorder (ADHD) symptoms and body mass index (BMI) among children and adolescents, and to assess variation by sex and developmental stage in a non-Western population using a twin design.
Methods: A total of 1,774 same-sex twins aged 6-18 years (1,150 monozygotic and 624 dizygotic) were drawn from the Chinese Child and Adolescent Twin Registry. ADHD symptoms were assessed using the parent-reported Child Behavior Checklist. Univariate and bivariate Cholesky decomposition models were applied to estimate additive genetic, shared environmental, and unique environmental contributions to ADHD symptoms and BMI, as well as their covariance, with analysis stratified by sex and age group (children aged 6-11 years and adolescents aged 12-18 years).
Results: Genetic factors accounted for 46% of the variance in ADHD symptoms and 88% of the variance in BMI. A significant positive phenotypic association was observed between ADHD symptoms and BMI (β = 0.29, P < 0.01), particularly among girls and adolescents. Bivariate twin modeling indicated a modest genetic correlation between ADHD symptoms and BMI in the full sample (rg = 0.13), with higher and statistically significant genetic correlations observed in girls (rg = 0.23) and in children (rg = 0.17). In adolescents, both genetic and unique environmental factors contributed to the association, with relatively greater unique environmental contributions in boys.
Conclusion: These findings indicate etiologically heterogeneous pathways linking ADHD symptoms and BMI across childhood and adolescence by sex and developmental stage, supporting neurobehaviorally informed risk stratification and prevention strategies.
Keywords
INTRODUCTION
Childhood obesity is a major and growing public health concern worldwide, and is associated with broad health and developmental consequences across the life course[1]. According to the World Health Organization, more than 390 million children aged 5-19 years were overweight or obese in 2022, marking a sharp increase over the past few decades[2]. In China, rapid urbanization and socioeconomic transitions have contributed to a rising prevalence of overweight and obesity among children aged 6-17 years, reaching 19%[3,4]. As a result, China now has the largest population of children with obesity worldwide, posing a substantial metabolic and public health burden[5,6].
The etiology of obesity is increasingly recognized as heterogeneous, reflecting complex interactions among biological, behavioral, and environmental factors[7]. While traditional factors such as diet, physical activity, and lifestyle have long been emphasized, emerging evidence highlights the contribution of neurobehavioral characteristics in shaping individual differences in obesity risk[8,9]. In recent years, the association between attention-deficit/hyperactivity disorder (ADHD) and obesity has garnered increasing attention[10-12]. ADHD is among the most prevalent childhood neurodevelopmental disorders. It is characterized by inattention, hyperactivity, and impulsivity, and affects approximately 8.0% of children worldwide[13] and 6.4% in China[14]. A systematic review reported a 40% higher prevalence of obesity among children with ADHD[10], and a recent meta-analysis further supported an increased risk of overweight and obesity (odds ratio 1.56), with higher estimates being observed in Asian populations (3.25)[11]. This comorbidity is associated with compounded adverse health outcomes and an increased healthcare burden[15,16].
Despite growing epidemiological evidence supporting the co-occurrence of ADHD and obesity, the etiological mechanisms underlying this association remain incompletely understood. Both conditions are highly heritable, with estimates of approximately 40%-75% heritability for obesity[17,18] and 30%-80% for ADHD[19,20]. A recent genome-wide association meta-analysis reported a significant genetic correlation between ADHD and obesity (rg = 0.22) and body mass index (BMI; rg = 0.26)[21], suggesting shared genetic liability. At the neurobiological level, dysregulation of dopaminergic pathways involved in appetite, motivation, and reward processing has been proposed as a potential common mechanism linking ADHD symptoms and obesity risk[22]. Genome-wide association and candidate gene studies have identified several loci associated with both conditions, including fat mass and obesity-associated (FTO), melanocortin-4 receptor (MC4R), brain-derived neurotrophic factor (BDNF), and synaptosomal-associated protein 25 (SNAP25), implicating pathways related to energy metabolism, neurotransmitter signaling, and synaptic plasticity[23-26]. Environmental factors, such as family socioeconomic status, parental education level, and parental mental health, also contribute to this comorbidity[27]. In addition, children with ADHD exhibit distinct dietary characteristics, such as higher consumption of junk food[28], unhealthy eating patterns[29], and faster eating rates[30]. Although hyperactivity is a core feature of ADHD, children with this condition engage in less daily physical activity (21% lower odds)[31] and face barriers to participation in school activities[32]. Sleep disturbances, including shorter total sleep time and lower sleep efficiency, are also more prevalent in children with ADHD[33]. Together, these behavioral factors may contribute to increased BMI and obesity risk.
Twin and family studies provide a powerful framework for disentangling the genetic, shared environmental (C), and unique environmental (E) contributions to complex traits and their co-occurrence[34]. To date, only a limited number of twin studies have examined the association between ADHD and obesity, reporting modest to moderate genetic correlations[35-37], with some evidence suggesting stronger associations in females[38,39]. However, existing research has largely focused on adolescents and adults[35-38], with limited attention to childhood[39], a critical developmental period when both ADHD symptoms and obesity risk emerge and evolve. Moreover, genetic and environmental influences on ADHD and obesity may vary across cultural and social contexts[40-42], underscoring the need for research in Asian populations.
This study aimed to examine the association between ADHD and BMI in a large sample of Chinese twins aged 6-18 years. Specifically, the objectives were to: (1) characterize the phenotypic association between ADHD symptoms and BMI; (2) estimate the relative contributions of genetic and environmental factors to each trait; and (3) assess the shared genetic and environmental influences underlying their overlap, with particular attention to differences by sex and age. By clarifying etiological heterogeneity in the association between ADHD symptoms and obesity risk by sex and developmental stages, this study may help inform more targeted public health prevention strategies.
METHODS
Subjects
This study enrolled 1,774 same-sex child and adolescent twins, aged 6-18 years, from the Chinese Child and Adolescent Twin Registry, with participants recruited in Beijing and Shandong Province from March 2010 to January 2022[43]. Data were collected using two methods. First, 542 twins (30.6%) and their parents visited the examination center to complete their respective questionnaires and undergo physical examinations. Second, 1,232 twins (69.4%) received questionnaires through their schools, completed them at home, and returned them to the school. The response rate for this group was 75.6%, and 1,026 twins (83.3%) also underwent physical examinations. The majority of parental questionnaires (67.3%) were completed by mothers, followed by fathers (27.2%) and other guardians (5.5%). Twin pairs were included only if both co-twins had complete data on age, sex, ADHD symptom scores, and BMI (derived from height and weight). Pairs were excluded if either co-twin had a disability, severe illness, or missing data on any variable. Written informed consent was obtained from all participating twins and their parents or legal guardians prior to participation. This study was approved by the Medical Ethics Committee of Peking University (IRB00001052-21146) and Shandong First Medical University (202111170196).
Zygosity determination
Zygosity was determined by DNA analysis (30.6%) or questionnaire-based assessment (69.4%). For DNA-based classification, the probability that a twin pair was monozygotic (MZ) when all genetic markers were concordant was 99.6%[44]. For questionnaire-based classification, zygosity was predicted using an algorithm based on items assessing twin confusion. This algorithm was developed using twin pairs with known zygosity and achieved 89.2% prediction accuracy[45]. The sample consisted of 1,150 MZ twins and 624 dizygotic (DZ) twins, including 556 MZ male twins, 308 DZ male twins, 594 MZ female twins, and 316 DZ female twins.
Measurements
Anthropometric measurements of height and weight for 1,568 twins (88.4%) were conducted by trained professionals at a health examination center following standardized procedures[46]. Height (cm) was measured to the nearest 0.5 cm using a wall-mounted stadiometer, and weight (kg) to the nearest 0.1 kg using a calibrated balance-beam scale. Both measurements were taken with participants wearing light clothing and no shoes. Height and weight data for 206 twins (11.6%) were self-reported. BMI was calculated as weight (kg) divided by height squared (m2). Among the 1,026 school-based respondents with both measured and self-reported BMI, the correlation coefficient was 0.82, indicating acceptable reliability of the self-reported measures. Twins with self-reported and measured anthropometric data did not differ significantly in sex, zygosity, or age distribution.
ADHD symptoms were assessed using the parent-reported Child Behavior Checklist (CBCL)/4-18[47]. The questionnaire comprises 120 items assessing behavioral and emotional problems in children ages 4-18. Parents rated each item on a three-point scale (0 = not true; 1 = sometimes true; 2 = often true). ADHD symptoms were quantified using the Attention Problems Scale, which has shown good convergent validity with structured interview‑based clinical diagnoses and is widely used as a dimensional measure of ADHD symptoms. The Chinese version of the CBCL has demonstrated satisfactory reliability and validity[48].
Statistical analysis
Means and standard deviations for ADHD symptoms and BMI were calculated by sex and age group (children aged 6-11 years and adolescents aged 12-18 years). ADHD symptoms were natural-log-transformed before analysis because of their skewed distribution. Group differences were examined using independent‑samples two-tailed t-tests, and P < 0.05 was considered statistically significant. Phenotypic residuals were derived from whole‑sample linear regression models that adjusted for continuous age and sex and were used in all subsequent analyses. Accordingly, sex‑specific and age‑stratified twin models reflected residual variation after adjustment for overall age and sex effects. Generalized estimating equations were used to estimate the association between BMI and ADHD symptoms while accounting for the non-independence of twin observations. Descriptive and regression analyses were conducted using IBM SPSS Statistics version 27.
Twin correlations for ADHD symptoms and BMI were calculated by sex, age group, and zygosity. Higher correlation in MZ than in DZ twins indicated a genetic influence on the trait’s variance. Quantitative genetic analyses were conducted to estimate additive genetic (A), C, and E contributions to each trait using twin modeling approaches[49]. Univariate ACE models were fitted to estimate variance components for ADHD symptoms and BMI. Bivariate Cholesky decomposition models were applied to assess the extent to which genetic and environmental influences were shared between ADHD symptoms and BMI [Figure 1]. This approach was selected as a flexible, exploratory method to decompose the covariance between traits without imposing strong a priori assumptions about the underlying structure. This was particularly suitable given the limited prior evidence on sex- and age-specific genetic overlap in this population. Quantitative genetic analyses were performed using the structural equation modeling package Mx[50], adjusting for age and sex. Full ACE models were retained to avoid potential bias associated with model reduction[51].
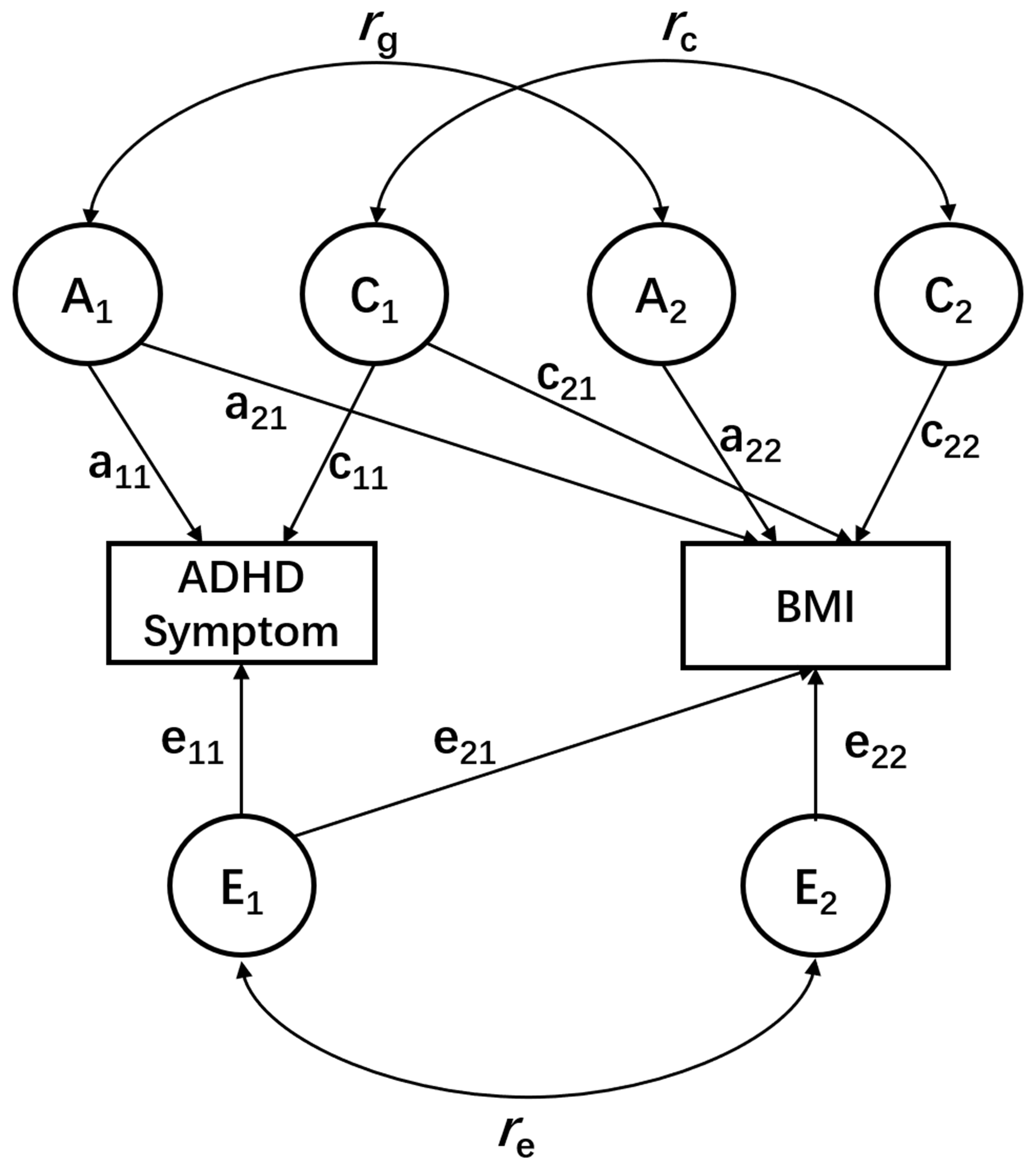
Figure 1. Bivariate Cholesky decomposition twin model for ADHD symptoms and BMI. A, C, and E represent the additive genetic, shared environmental, and unique environmental variance components, respectively. a, c, and e denote the corresponding path coefficients. ADHD symptoms and BMI are two phenotypic measures in a single twin. rg, rc, and re indicate the genetic, shared environmental, and unique environmental correlations between the two traits, respectively. For clarity, only one twin is shown. ADHD: Attention-deficit/hyperactivity disorder; BMI: body mass index.
RESULTS
A total of 1,774 same-sex twins aged 6 to 18 years (mean age, 10.96 ± 3.04 years) were included in the analysis. Descriptive statistics for BMI and ADHD symptoms assessed by the CBCL are presented in Table 1, stratified by age group and sex. Overall, boys showed higher ADHD symptom scores than girls, whereas BMI was higher in boys and adolescents than in children.
Sample characteristics of BMI and ADHD symptoms by age group and sex
| Variables | 6-11 years old | 12-18 years old | All | Total | |||
| Male | Female | Male | Female | Male | Female | ||
| No. | 550 | 610 | 314 | 300 | 864 | 910 | 1,774 |
| Age (years) | 9.02 (1.59) | 9.18 (1.61) | 14.52 (1.84) | 14.4 (1.69) | 11.02 (3.14) | 10.9 (2.95) | 10.96 (3.04) |
| BMI | 17.86 (3.31)*,# | 16.96 (3.02)# | 20.91 (4.1) | 20.44 (3.97) | 18.97 (3.9)* | 18.1 (3.74) | 18.53 (3.84) |
| ADHD symptom | 1.64 (2.08)* | 1.3 (2.11) | 1.43 (2.17) | 1.33 (2.11) | 1.56 (2.11)* | 1.31 (2.11) | 1.43 (2.11) |
Intraclass correlation coefficients for ADHD symptoms and BMI, stratified by sex, age group, and zygosity, are presented in Table 2. Across all sex and age groups, intraclass correlations were consistently higher in MZ twins than in DZ twins for both ADHD symptoms and BMI. In addition, DZ correlations for ADHD symptoms exceeded half of the corresponding MZ correlations across groups.
Intraclass correlation coefficients, adjusted for age group and sex
| Variables | MZ | DZ | All | |||
| MZM | MZF | DZM | DZF | MZ | DZ | |
| 6-11 years old | ||||||
| Twin pairs No. | 169 | 186 | 106 | 119 | 355 | 225 |
| BMI | 0.86 | 0.89 | 0.40 | 0.41 | 0.87 | 0.40 |
| ADHD symptoms | 0.92 | 0.95 | 0.64 | 0.74 | 0.93 | 0.70 |
| 12-18 years old | ||||||
| Twin pairs No. | 109 | 111 | 48 | 39 | 220 | 87 |
| BMI | 0.88 | 0.92 | 0.40 | 0.54 | 0.90 | 0.46 |
| ADHD symptoms | 0.92 | 0.95 | 0.64 | 0.72 | 0.93 | 0.67 |
| All | ||||||
| Twin pairs No. | 278 | 297 | 154 | 158 | 575 | 312 |
| BMI | 0.87 | 0.90 | 0.40 | 0.47 | 0.89 | 0.43 |
| ADHD symptoms | 0.92 | 0.95 | 0.65 | 0.73 | 0.93 | 0.70 |
Univariate ACE models were fitted to estimate the genetic and environmental contributions to BMI and ADHD symptoms [Table 3]. For BMI, A influences accounted for a large proportion of the variance [0.88, 95% confidence interval (CI): 0.72-0.90], whereas E influences accounted for the remaining variance (0.12, 95%CI: 0.10-0.13), with shared environmental estimates close to zero. For ADHD symptoms, A influences accounted for approximately 46% of the variance (0.46, 95%CI: 0.37-0.57), while shared environmental influences accounted for a comparable proportion (0.47, 95%CI: 0.36-0.56), and E influences accounted for a very small proportion (0.07, 95%CI: 0.06-0.08). Similar patterns were observed across sex and age strata, with modest variation in the point estimates.
Estimates of genetic and environmental effects from univariate analyses
| BMI | ADHD symptom | |||||
| A (95%CI) | C (95%CI) | E (95%CI) | A (95%CI) | C (95%CI) | E (95%CI) | |
| Boys | ||||||
| 6-11 years old | 0.86 (0.63-0.89) | 0.00 (0.00-0.23) | 0.14 (0.11-0.18) | 0.46 (0.31-0.68) | 0.45 (0.23-0.61) | 0.09 (0.07-0.11) |
| 12-18 years old | 0.89 (0.65-0.92) | 0.00 (0.00-0.24) | 0.11 (0.08-0.16) | 0.53 (0.30-0.90) | 0.39 (0.02-0.62) | 0.08 (0.06-0.11) |
| subtotal | 0.87 (0.71-0.90) | 0.00 (0.00-0.16) | 0.13 (0.10-0.16) | 0.48 (0.35-0.66) | 0.43 (0.25-0.57) | 0.08 (0.07-0.10) |
| Girls | ||||||
| 6-11 years old | 0.88 (0.63-0.90) | 0.00 (0.00-0.24) | 0.12 (0.10-0.16) | 0.46 (0.33-0.63) | 0.50 (0.32-0.63) | 0.05 (0.04-0.06) |
| 12-18 years old | 0.76 (0.44-0.94) | 0.16 (0.00-0.48) | 0.08 (0.06-0.11) | 0.42 (0.23-0.76) | 0.52 (0.18-0.72) | 0.06 (0.04-0.08) |
| subtotal | 0.80 (0.60-0.91) | 0.09 (0.00-0.30) | 0.10 (0.09-0.13) | 0.44 (0.33-0.59) | 0.51 (0.36-0.62) | 0.05 (0.04-0.06) |
| All | ||||||
| 6-11 years old | 0.87 (0.70-0.89) | 0.00 (0.00-0.17) | 0.13 (0.11-0.16) | 0.46 (0.35-0.59) | 0.48 (0.35-0.58) | 0.07 (0.05-0.08) |
| 12-18 years old | 0.90 (0.66-0.92) | 0.00 (0.00-0.24) | 0.10 (0.08-0.12) | 0.49 (0.32-0.72) | 0.45 (0.21-0.61) | 0.07 (0.05-0.09) |
| Total | 0.88 (0.72-0.90) | 0.00 (0.00-0.16) | 0.12 (0.10-0.13) | 0.46 (0.37-0.57) | 0.47 (0.36-0.56) | 0.07 (0.06-0.08) |
Associations between ADHD symptoms and BMI were examined, and estimates from the regression and bivariate twin models are presented in Table 4 and summarized in Figure 2. In the full sample, ADHD symptoms were positively associated with BMI (β = 0.29, 95%CI: 0.08-0.50). Subgroup analyses indicated that this association was more pronounced among girls and adolescents, with the strongest association observed in girls aged 12-18 years (β = 0.92, 95%CI: 0.25-1.58). Bivariate twin modeling estimated a modest genetic correlation between ADHD symptoms and BMI in the full sample (rg = 0.13, 95%CI: -0.01-0.27). Higher and statistically significant genetic correlations were observed in girls (rg = 0.23, 95%CI: 0.03-0.41) and in children (rg = 0.17, 95%CI: 0.01-0.33). In adolescents, both genetic and E factors contributed to the association between ADHD symptoms and BMI. The estimated E correlations were relatively larger than those in younger children, although they did not reach statistical significance.
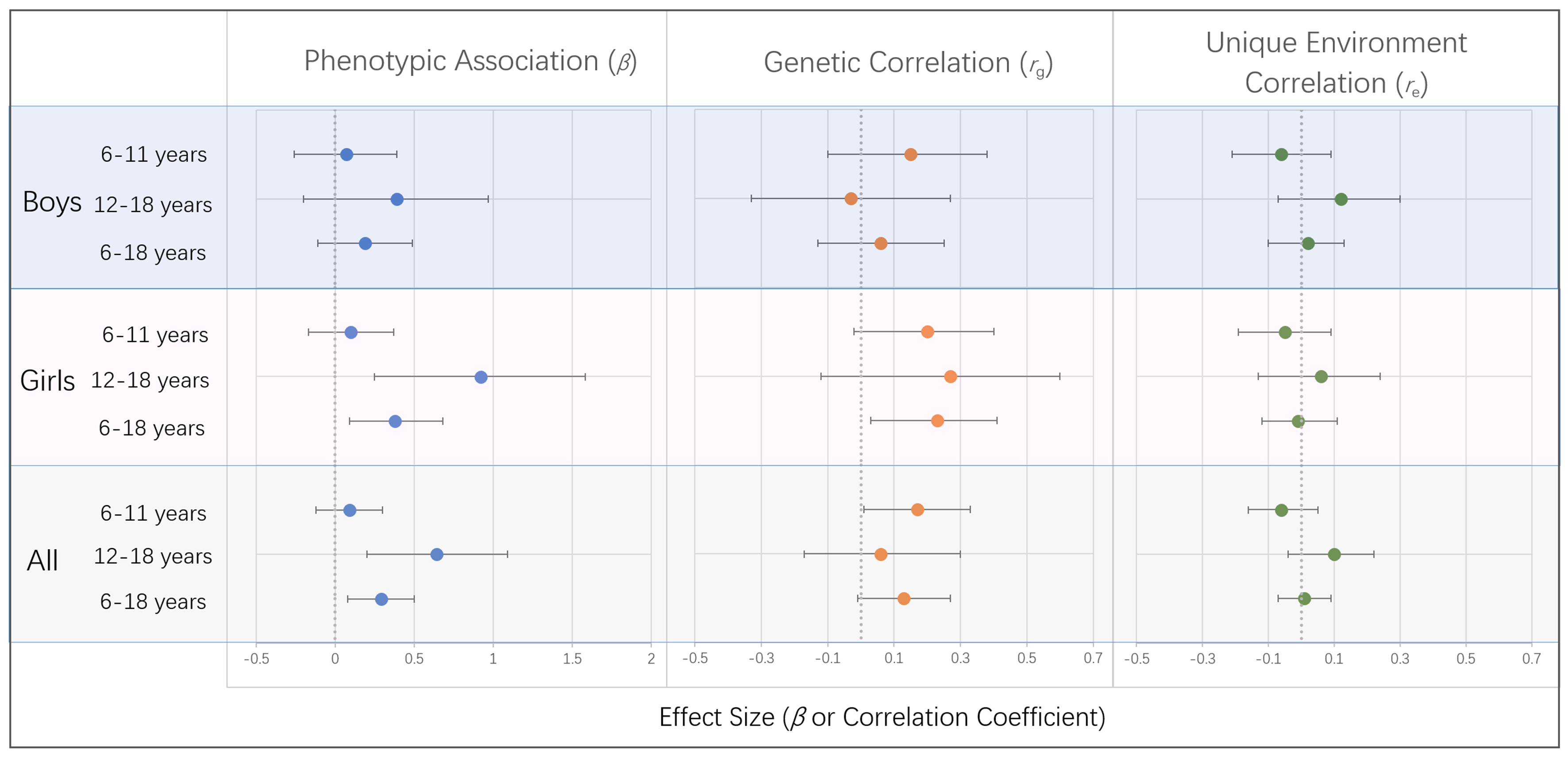
Figure 2. Sex- and Age-Specific Associations of ADHD Symptoms With BMI. Points represent effect estimates, and horizontal bars indicate 95%CI. Phenotypic associations are expressed as regression coefficients (β), while genetic and unique environmental correlations are expressed as rg and re, respectively. Statistical significance is inferred when the 95%CI does not include zero. Sample sizes for each subgroup are provided in Table 1. ADHD: Attention-deficit/hyperactivity disorder; BMI: body mass index; CI: confidence interval.
Estimates of genetic and environmental effects from bivariate analyses
| Regression | Component correlation | ||||
| Coefficient β (95%CI) | P | r g (95%CI) | r c (95%CI) | r e (95%CI) | |
| Boys | |||||
| 6-11 years old | 0.07 (-0.26-0.39) | 0.694 | 0.15 (-0.10-0.38) | -1.00 (-1.00-1.00) | -0.06 (-0.21-0.09) |
| 12-18 years old | 0.39 (-0.20-0.97) | 0.199 | -0.03 (-0.33-0.27) | 1.00 (-1.00-1.00) | 0.12 (-0.07-0.30) |
| subtotal | 0.19 (-0.11-0.49) | 0.216 | 0.06 (-0.13-0.25) | -1.00 (-1.00-1.00) | 0.02 (-0.10-0.13) |
| Girls | |||||
| 6-11 years old | 0.10 (-0.17-0.37) | 0.453 | 0.20 (-0.02-0.40) | -1.00 (-1.00-1.00) | -0.05 (-0.19-0.09) |
| 12-18 years old | 0.92 (0.25-1.58) | 0.007 | 0.27 (-0.12-0.60) | 0.10 (-1.00-1.00) | 0.06 (-0.13-0.24) |
| subtotal | 0.38 (0.09-0.68) | 0.011 | 0.23 (0.03-0.41) | -0.15 (-1.00-1.00) | -0.01 (-0.12-0.11) |
| All | |||||
| 6-11 years old | 0.09 (-0.12-0.30) | 0.407 | 0.17 (0.01-0.33) | -1.00 (-1.00-1.00) | -0.06 (-0.16-0.05) |
| 12-18 years old | 0.64 (0.20-1.09) | 0.005 | 0.06 (-0.17-0.30) | 1.00 (-1.00-1.00) | 0.10 (-0.04-0.22) |
| Total | 0.29 (0.08-0.50) | 0.008 | 0.13 (-0.01-0.27) | -1.00 (-1.00-1.00) | 0.01 (-0.07-0.09) |
DISCUSSION
This study investigated the genetic and environmental factors underlying the association between ADHD symptoms and BMI in a large sample of Chinese twins aged 6-18 years. We observed a modest genetic overlap between ADHD symptoms and BMI in the overall sample, with stronger and statistically significant genetic correlations in girls and younger children. These findings are consistent with previous evidence suggesting shared genetic liability between ADHD and BMI and extend the literature by highlighting the importance of sex and developmental stage in shaping this association in a non-Western population.
Our findings provide a detailed characterization of the association between ADHD symptoms and BMI, highlighting variation across sex and developmental stage. We report a statistically significant positive phenotypic association between ADHD symptoms and BMI, consistent with a growing body of literature linking ADHD to obesity and related metabolic outcomes[10,41,52]. Previous studies have reported mixed evidence regarding sex- and age-specific patterns in this association. For example, meta-analyses by
Bivariate twin analyses suggest a modest genetic overlap between ADHD symptoms and BMI, with higher and statistically significant genetic correlations observed in girls. This female-specific pattern of shared genetic liability is consistent with prior twin research, including studies of Swedish adolescents that reported stronger genetic overlap in girls[38], as well as evidence that genetic correlations are present in females across childhood and adolescence[39]. These sex-specific genetic patterns provide population-level support for hypothesized neurobehavioral mechanisms linking ADHD and obesity risk. Prior molecular genetics and neuroimaging studies have suggested partial overlap in polygenic risk and neural circuits involved in reward processing and self-regulation linking ADHD-related impulsivity with BMI[37]. Pubertal hormonal changes in females, particularly fluctuations in estrogen, may further interact with these genetic susceptibilities to influence attention regulation, emotional processing, and reward sensitivity, thereby increasing vulnerability to impulsivity-related eating behaviors and obesity risk[56,57]. By contrast, higher levels of hyperactivity in males may be associated with greater energy expenditure, potentially attenuating weight gain during certain developmental periods[23]. Together, these findings help contextualize the observed sex differences and highlight specific neurobehavioral pathways that warrant further investigation.
In addition to sex-specific genetic patterns, the relative contributions of genetic and environmental factors also varied by developmental stages. During childhood, genetic factors accounted for a larger proportion of the association in both sexes, whereas environmental contributions were relatively modest. In adolescence, genetic influences remained evident in girls, while E contributions became relatively more pronounced in boys. This sex-specific developmental pattern is consistent with longitudinal evidence indicating that higher ADHD symptom scores in girls were associated with steeper increases in BMI trajectories from childhood into late adolescence[58]. Developmental changes during adolescence, including increased autonomy and shifting environmental exposures, may interact with neurobehavioral traits related to ADHD and obesity risk. Such interactions occur within a broader context of shared genetic and early-life environmental liability linking ADHD and obesity[27,35]. Together, these developmental patterns are consistent with broader evidence that hyperactivity-related behaviors in males tend to decline after childhood, whereas impulsivity and inattention in females may persist into adolescence. Such sex-specific developmental differences may coincide with periods of heightened behavioral and metabolic susceptibility[59], potentially contributing to heterogeneity in obesity risk.
Consistent with previous literature, boys exhibited higher levels of ADHD symptoms than girls, reflecting well-established sex differences in symptom presentation[59]. Concomitantly, boys and adolescents had higher BMIs, in line with normative developmental patterns of weight gain[60]. Twin correlations and univariate genetic analyses confirmed substantial genetic contributions to both ADHD symptoms and BMI, consistent with prior twin studies[61,62]. The heritability estimate for ADHD symptoms in this study was modestly lower than that in our previous report[43]. This may reflect differences in sample composition, including questionnaire-based zygosity determination and the restriction to same-sex twin pairs. Shared environmental influences were evident for ADHD symptoms but minimal for BMI, suggesting that family and school environments may shape ADHD-related behaviors more strongly than body weight. This pattern may partly reflect contextual influences in collectivist settings such as China, where shared social environments may exert a stronger influence on behavioral traits[40]. In addition, because ADHD symptoms were assessed using parent-reported CBCL data, with the same parent often rating both twins, the relatively high shared environmental variance for ADHD symptoms may have been inflated by rater effects, such as parental response style or reporting bias, a concern particularly relevant in single-informant designs[63,64].
Several limitations should be noted. First, ADHD symptoms were assessed using parent-reported CBCL data, which, although widely validated, may be subject to reporting bias and does not provide clinician-based diagnostic confirmation. Therefore, the findings should be interpreted as reflecting dimensional ADHD-related symptoms rather than clinically diagnosed ADHD, which may limit generalizability to clinical populations. In addition, 11.6% of the BMI data were self-reported. Despite a high correlation with measured anthropometrics (r = 0.82), self-report may underestimate BMI because of underreported weight or overreported height, potentially attenuating the observed association. Second, ADHD subtypes were not distinguished, limiting insights into subtype-specific mechanisms. In addition, information on ADHD treatment status was not available, precluding evaluation of treatment effects on the association between ADHD symptoms and BMI. Third, epigenetic processes, gene-environment interactions, and gene-environment correlations were not examined. Therefore, the estimated variance components may not fully capture the complex interplay between genetic liability and environmental exposure, particularly for ADHD symptoms. Fourth, important environmental and behavioral factors related to BMI, such as physical activity and dietary patterns, were not directly evaluated, limiting interpretation of the underlying mechanisms of the association between ADHD symptoms and BMI. Fifth, analyses were restricted to same-sex twin pairs, precluding direct tests of sex differences in genetic architecture using opposite-sex comparisons and potentially limiting the generalizability of the sex-specific findings. Sixth, the sample was drawn from Beijing and Shandong and therefore may lack national representativeness; it did not include urban-rural information, which may limit the broader applicability of the findings. Finally, although this study represents one of the largest twin samples of Chinese children and adolescents to date, the sample size, especially in stratified analyses, may have limited statistical power to detect more nuanced effects.
In summary, this large twin study conducted in an Asian population advances understanding of the association between ADHD and BMI by delineating etiologically heterogeneous pathways shaped by sex and developmental stage. Genetic influences predominated in childhood, whereas in adolescence, genetic effects remained stronger in females, while environmental influences appeared more prominent in males. These findings underscore the importance of incorporating sex and developmental stage into etiological models of childhood obesity risk and support more differentiated prevention strategies. Interventions addressing environmental and behavioral factors may be particularly relevant for boys, whereas strategies emphasizing neurobehavioral regulation may hold greater promise for girls.
DECLARATIONS
Acknowledgments
We sincerely thank all participating twins and their families, and the support from the Chinese Child and Adolescent Twin Registry.
Authors’ contributions
Conceptualization: Chen TJ, Song Y, Chang Z
Methodology: Chen TJ, Guo T, Li Y, Chang Z
Data collection: Guo T, Li Y, Chen TJ
Formal analysis: Chen TJ, Guo T
Writing - original draft: Chen TJ
Writing - review and editing: Song Y, Chang Z
Supervision: Song Y
All authors approved the final submitted manuscript.
Availability of data and materials
The data supporting the findings of this study are available from the Chinese Child and Adolescent Twin Registry upon reasonable request and with permission from the data custodians. Due to ethical and privacy considerations, the data are not publicly available.
AI and AI-assisted tools statement
During the preparation of this manuscript, the AI tool DeepSeek (version 3.2, released 2025-12-01) was used solely for language editing. The tool did not influence the study design, data collection, analysis, interpretation, or the scientific content of the work. All authors take full responsibility for the accuracy, integrity, and final content of the manuscript.
Financial support and sponsorship
This work was supported by National Key R&D Program of China (2024YFC3308300) and National Natural Science Foundation of China (81001249).
Conflicts of interest
Song Y is the Guest Editor of the special issue entitled “Metabolic Heterogeneity in Childhood Obesity and Preventive Strategy” in the journal Metabolism and Target Organ Damage. Song Y was not involved in the editorial handling, peer review or editorial decision-making for this manuscript. Chang Z received lecture honoraria from Takeda Pharmaceuticals, outside the submitted work. The other authors declare that there are no conflicts of interest.
Ethical approval and consent to participate
This study was approved by the Medical Ethics Committee of Peking University (IRB00001052-21146) and Shandong First Medical University (202111170196). Written informed consent was obtained from all participating twins and their parents or legal guardians prior to participation.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Zhang X, Liu J, Ni Y, et al. Global prevalence of overweight and obesity in children and adolescents: a systematic review and meta-analysis. JAMA Pediatr. 2024;178:800-13.
2. World Health Organization. Obesity and overweight. Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight. [Last accessed on 5 Jun 2026].
3. Yuan C, Dong Y, Chen H, et al. Determinants of childhood obesity in China. Lancet Public Health. 2024;9:e1105-14.
4. Pan XF, Wang L, Pan A. Epidemiology and determinants of obesity in China. Lancet Diabetes Endocrinol. 2021;9:373-92.
5. Song X, Zhou B, Baird S, et al. Trends and predictions to 2030 in demographic structures and metabolic health for children and adolescents in China: analysis of national school health surveys from 2000 to 2019. Lancet Child Adolesc Health. 2025;9:530-43.
6. Yuan C, Dong Y, Chen H, et al. Public health interventions against childhood obesity in China. Lancet Public Health. 2024;9:e1115-24.
7. Liu P, Zhang M, Li A, et al. Heterogeneity of obesity and its predictive factors: a narrative review of recent human and rodent studies. Obes Rev. 2026;27:e70024.
8. Nelson TD, Stice E. Contextualizing the neural vulnerabilities model of obesity. Nutrients. 2023;15:2988.
9. Carnell S, Thapaliya G, Jansen E, Chen L. Biobehavioral susceptibility for obesity in childhood: Behavioral, genetic and neuroimaging studies of appetite. Physiol Behav. 2023;271:114313.
10. Cortese S, Moreira-Maia CR, St Fleur D, Morcillo-Peñalver C, Rohde LA, Faraone SV. Association between ADHD and obesity: a systematic review and meta-analysis. Am J Psychiatry. 2016;173:34-43.
11. Zhu Y, Wang NN, Pan D, Wang S. Risk of overweight and obesity in children and adolescents with attention-deficit/hyperactivity disorder: a systematic review and meta-analysis. Child Obes. 2024;20:119-27.
12. Marcelli I, Capece U, Caturano A. Bridging ADHD and metabolic disorders: insights into shared mechanisms and clinical implications. Diabetology. 2025;6:40.
13. Ayano G, Demelash S, Gizachew Y, Tsegay L, Alati R. The global prevalence of attention deficit hyperactivity disorder in children and adolescents: an umbrella review of meta-analyses. J Affect Disord. 2023;339:860-6.
14. Liu J, Jiang Z, Li F, et al. Prevalence and comorbidity of attention deficit hyperactivity disorder in Chinese school-attending students aged 6-16: a national survey. Ann Gen Psychiatry. 2025;24:23.
15. Libutzki B, Ludwig S, May M, Jacobsen RH, Reif A, Hartman CA. Direct medical costs of ADHD and its comorbid conditions on basis of a claims data analysis. Eur Psychiatry. 2019;58:38-44.
16. French B, Nalbant G, Wright H, et al. The impacts associated with having ADHD: an umbrella review. Front Psychiatry. 2024;15:1343314.
17. Bouchard C. Genetics of obesity: what we have learned over decades of research. Obesity. 2021;29:802-20.
18. Khusainova R, Minniakhmetov I, Vasyukova O, et al. Genetic landscape of obesity in children: research advances and prospects. J Obes. 2025;2025:9186826.
19. Kranz TM, Grimm O. Update on genetics of attention deficit/hyperactivity disorder: current status 2023. Curr Opin Psychiatry. 2023;36:257-62.
20. Kleppesto TH, Eilertsen EM, van Bergen E, et al. Intergenerational transmission of ADHD behaviors: genetic and environmental pathways. Psychol Med. 2024;54:1309-17.
21. Demontis D, Walters RK, Martin J, et al.; ADHD Working Group of the Psychiatric Genomics Consortium (PGC), Early Lifecourse & Genetic Epidemiology (EAGLE) Consortium, 23andMe Research Team. Discovery of the first genome-wide significant risk loci for attention deficit/hyperactivity disorder. Nat Genet. 2019;51:63-75.
22. Seymour KE, Reinblatt SP, Benson L, Carnell S. Overlapping neurobehavioral circuits in ADHD, obesity, and binge eating: evidence from neuroimaging research. CNS Spectr. 2015;20:401-11.
23. Hanć T, Cortese S. Attention deficit/hyperactivity-disorder and obesity: a review and model of current hypotheses explaining their comorbidity. Neurosci Biobehav Rev. 2018;92:16-28.
24. Demontis D, Walters GB, Athanasiadis G, et al.; ADHD Working Group of the Psychiatric Genomics Consortium, iPSYCH-Broad Consortium. Genome-wide analyses of ADHD identify 27 risk loci, refine the genetic architecture and implicate several cognitive domains. Nat Genet. 2023;55:198-208.
25. Bahrami S, Steen NE, Shadrin A, et al. Shared genetic loci between body mass index and major psychiatric disorders: a genome-wide association study. JAMA Psychiatry. 2020;77:503-12.
26. Mota NR, Poelmans G, Klein M, et al. Cross-disorder genetic analyses implicate dopaminergic signaling as a biological link between Attention-Deficit/Hyperactivity Disorder and obesity measures. Neuropsychopharmacology. 2020;45:1188-95.
27. Chen Q, Kuja-Halkola R, Sjölander A, et al. Shared familial risk factors between attention-deficit/hyperactivity disorder and overweight/obesity - a population-based familial coaggregation study in Sweden. J Child Psychol Psychiatry. 2017;58:711-8.
28. Khazdouz M, Safarzadeh R, Hejrani B, et al. The association between junk foods consumption and attention deficit hyperactivity disorder in children and adolescents: a systematic review and meta-analysis of observational studies. Eur Child Adolesc Psychiatry. 2025;34:825-34.
29. Pinto S, Correia-de-Sá T, Sampaio-Maia B, Vasconcelos C, Moreira P, Ferreira-Gomes J. Eating patterns and dietary interventions in ADHD: a narrative review. Nutrients. 2022;14:4332.
30. Wang X, Yue X, Wang L, Jia F, Li H. Eating behavior and sleep habit problems and their correlation with symptoms in children with ADHD comorbid with overweight or obesity. Child Adolesc Psychiatry Ment Health. 2025;19:99.
31. Mercurio LY, Amanullah S, Gill N, Gjelsvik A. Children with ADHD engage in less physical activity. J Atten Disord. 2021;25:1187-95.
32. Kara K, Kaya Kara O, Kose B, et al. School participation, supports and barriers of children with and without attention deficit hyperactivity disorder. BMJ Paediatr Open. 2025;9:e002917.
33. Xian P, Sheng X, Liu S, Liu Z, Guo X. Sleep dysregulation in ADHD children: a systematic review and meta-analysis. Psychol Med. 2025;55:e321.
34. Hagenbeek FA, Hirzinger JS, Breunig S, et al. Maximizing the value of twin studies in health and behaviour. Nat Hum Behav. 2023;7:849-60.
35. Karhunen V, Bond TA, Zuber V, et al. The link between attention deficit hyperactivity disorder (ADHD) symptoms and obesity-related traits: genetic and prenatal explanations. Transl Psychiatry. 2021;11:455.
36. Liu CY, Schoeler T, Davies NM, et al. Are there causal relationships between attention-deficit/hyperactivity disorder and body mass index? Evidence from multiple genetically informed designs. Int J Epidemiol. 2021;50:496-509.
37. Barker ED, Ing A, Biondo F, et al.; IMAGEN Consortium. Do ADHD-impulsivity and BMI have shared polygenic and neural correlates? Mol Psychiatry. 2021;26:1019-28.
38. Javaras KN, Munn-Chernoff MA, Diemer EW, et al. Shared genetic factors contributing to the overlap between attention-deficit/hyperactivity disorder symptoms and overweight/obesity in Swedish adolescent girls and boys. Twin Res Hum Genet. 2022;25:226-33.
39. Do EK, Haberstick BC, Williams RB, et al. The role of genetic and environmental influences on the association between childhood ADHD symptoms and BMI. Int J Obes. 2019;43:33-42.
40. Zheng Y, Pingault JB, Unger JB, Rijsdijk F. Genetic and environmental influences on attention-deficit/hyperactivity disorder symptoms in Chinese adolescents: a longitudinal twin study. Eur Child Adolesc Psychiatry. 2020;29:205-16.
41. Cortese S. The association between ADHD and obesity: intriguing, progressively more investigated, but still puzzling. Brain Sci. 2019;9:256.
42. Zhang S, Huang Y, Zaid M, Tong L. ADHD symptoms and obesity in Chinese children and adolescents: a longitudinal study with abnormal eating behaviors as moderating factors. J Atten Disord. 2022;26:1452-63.
43. Chen TJ, Ji CY, Wang SS, Lichtenstein P, Larsson H, Chang Z. Genetic and environmental influences on the relationship between ADHD symptoms and internalizing problems: a Chinese twin study. Am J Med Genet B Neuropsychiatr Genet. 2016;171:931-7.
44. Chen TJ, Ji CY, Hu YH. Genetic and environmental influences on serum lipids and the effects of puberty: a Chinese twin study. Acta Paediatr. 2009;98:1029-36.
45. Gao W, Li L, Cao W, et al. Determination of zygosity by questionnaire and physical features comparison in Chinese adult twins. Twin Res Hum Genet. 2006;9:266-71.
46. CNSSCH Research Group. Report on the 2010 Chinese National Survey on Students’ Constitution and Health. Beijing: China Higher Education Press; 2012. Available from: https://www.bzfxw.com/soft/sort011/jiankang/800282.html. [Last accessed on 5 Jun 2026].
47. Achenbach TM. Manual for the Child Behavior Checklist/4-18 and 1991 Profile. Burlington, VT: University of Vermont, Department of Psychiatry; 1991. Available from: https://archive.org/details/manualforchildbe0000ache_g2r5. [Last accessed on 5 Jun 2026].
48. Leung PW, Kwong SL, Tang CP, et al. Test-retest reliability and criterion validity of the Chinese version of CBCL, TRF, and YSR. J Child Psychol Psychiatry. 2006;47:970-3.
49. Neale MC, Maes HHM. Methodology for genetic studies of twins and families. Dordrecht: Kluwer Academic Publishers; 2004. Available from: http://ibgwww.colorado.edu/workshop2006/cdrom/HTML/book2004a.pdf. [Last accessed on 5 Jun 2026].
50. Neale MC. Mx: Statistical Modeling. 6th Edition. Richmond, VA: Virginia Commonwealth University; 2004.
51. Sullivan PF, Eaves LJ. Evaluation of analyses of univariate discrete twin data. Behav Genet. 2002;32:221-7.
52. O’Hara VM, Curran JL, Browne NT. The co-occurrence of pediatric obesity and ADHD: an understanding of shared pathophysiology and implications for collaborative management. Curr Obes Rep. 2020;9:451-61.
53. Nigg JT, Johnstone JM, Musser ED, Long HG, Willoughby MT, Shannon J. Attention-deficit/hyperactivity disorder (ADHD) and being overweight/obesity: new data and meta-analysis. Clin Psychol Rev. 2016;43:67-79.
54. Rodgers RF, Laveway K, Campos P, de Carvalho PHB. Body image as a global mental health concern. Glob Ment Health. 2023;10:e9.
55. Nolan LJ, Higgs S. The role of irrational beliefs in the relationship between attention deficit hyperactivity disorder (ADHD) symptoms and disordered eating in two general student samples. Appetite. 2024;195:107229.
56. Eng AG, Nirjar U, Elkins AR, et al. Attention-deficit/hyperactivity disorder and the menstrual cycle: Theory and evidence. Horm Behav. 2024;158:105466.
57. Osianlis E, Thomas EHX, Jenkins LM, Gurvich C. ADHD and sex hormones in females: a systematic review. J Atten Disord. 2025;29:706-23.
58. Reed C, Cortese S, Golm D, Brandt V. Longitudinal associations between attention-deficit/hyperactivity and weight from birth to adolescence. J Am Acad Child Adolesc Psychiatry. 2025;64:1192-200.
59. Babinski DE. Sex differences in ADHD: review and priorities for future research. Curr Psychiatry Rep. 2024;26:151-6.
60. Heiskala A, Tucker JD, Choudhary P, et al. Timing based clustering of childhood BMI trajectories reveals differential maturational patterns; Study in the Northern Finland Birth Cohorts 1966 and 1986. Int J Obes. 2025;49:872-80.
61. Knyspel J, Morneau-Vaillancourt G, Eley TC. Using bifactor twin modeling to assess the genetic and environmental dimensionality of adult ADHD symptoms. Behav Genet. 2025;55:1-11.
62. Silventoinen K, Li W, Jelenkovic A, et al. Changing genetic architecture of body mass index from infancy to early adulthood: an individual based pooled analysis of 25 twin cohorts. Int J Obes. 2022;46:1901-9.
63. Rhee SH, Waldman ID. Genetic and environmental influences on antisocial behavior: a meta-analysis of twin and adoption studies. Psychol Bull. 2002;128:490-529.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Special Topic
Copyright

Data & Comments
Data
0













Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].