


Long-term prognosis of fulminant myocarditis: a multicenter prospective cohort study in China
 0
0 Abstract
Introduction: Comparative data on long-term outcomes (> 5 years) between fulminant myocarditis (FM) and non-fulminant myocarditis (NFM) remain limited, particularly under contemporary treatment strategies in China.
Aim: To compare long-term clinical outcomes between FM and NFM patients and to evaluate the prognostic value of persistent troponin I elevation.
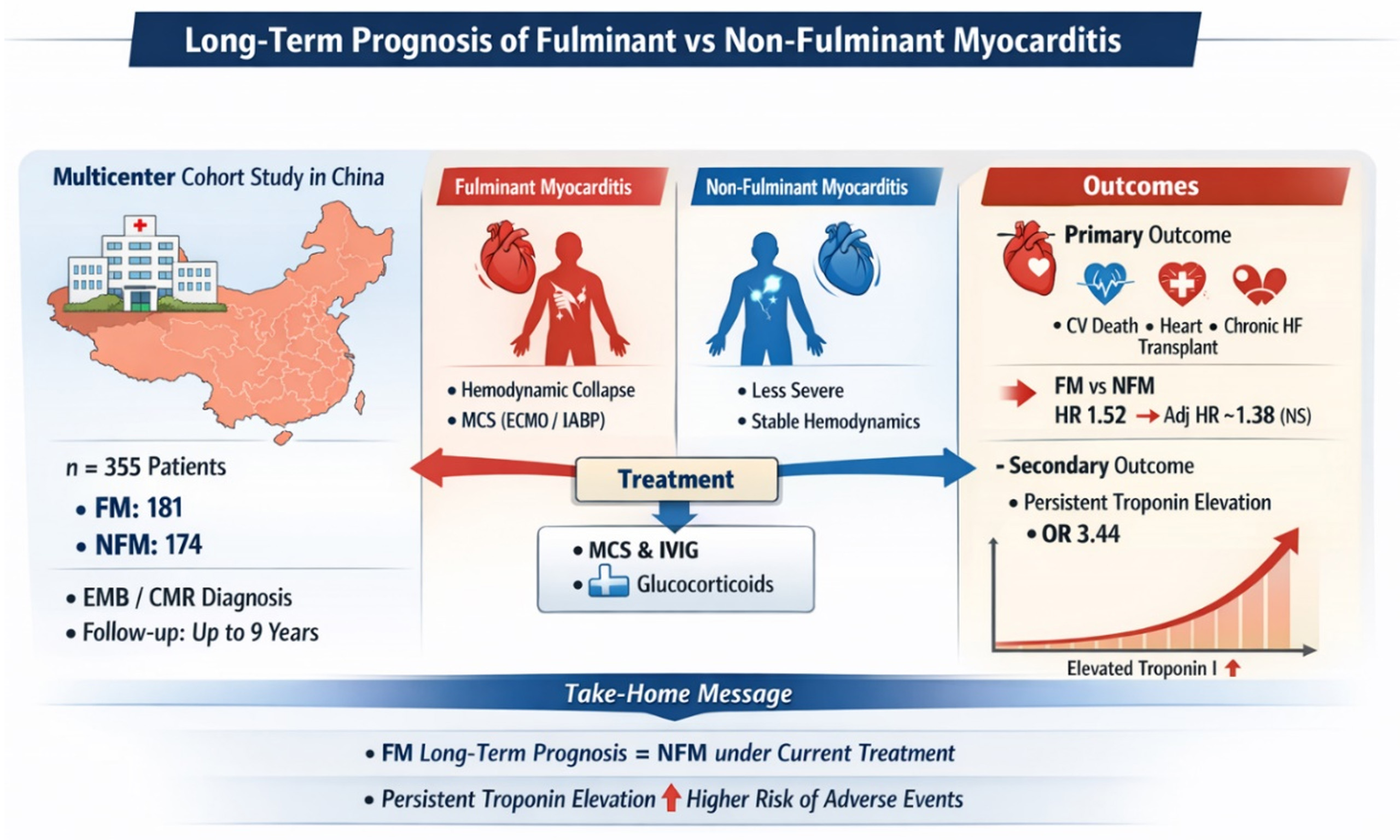
Methods and Results: In this multicenter prospective cohort study, 355 patients with myocarditis confirmed by endomyocardial biopsy or cardiac magnetic resonance were enrolled (181 FM, 174 NFM). The primary composite endpoint included cardiovascular death, heart transplantation, chronic heart failure, or cardiac structural abnormalities. The secondary outcome was persistent troponin I elevation (> 34.2 pg/mL at 1 month). Directed acyclic graphs guided covariate selection in Cox regression models. In the unadjusted analysis, FM was associated with a higher risk of the primary outcome compared with NFM [hazard ratio (HR) 1.52, 95% confidence interval (CI) 1.10-2.11; P = 0.011]. After adjustment for age, sex, and time from symptom onset to hospitalization, this association was attenuated and no longer statistically significant (HR 1.38, 95%CI 0.98-1.94; P = 0.062). Findings were consistent in propensity score-matched and age ≥ 15 years subgroups. FM patients had a higher likelihood of persistent troponin elevation [odds ratio (OR) 3.44, 95%CI 2.01-6.03; P < 0.001]. Persistent troponin elevation was positively associated with increased risk of the primary outcome.
Conclusion: Under current treatment strategies in China, FM was not associated with a significantly higher long-term risk compared with NFM. However, limited statistical power may influence this finding. Persistent troponin elevation is associated with a worse prognosis.
Keywords
INTRODUCTION
Myocarditis refers to localized or widespread inflammation of the myocardium, triggered by multiple etiologies. Among its subtypes, fulminant myocarditis (FM) stands as the most severe manifestation[1-3]. In patients with FM, the condition commonly exhibits a rapid progression, leading to refractory shock or life-threatening arrhythmias, ultimately resulting in a notably increased mortality rate[2-4]. The major cause of FM is viral infection, which can directly affect the heart or elicit an immune response, ultimately leading to acute heart failure[5,6].
We treated Chinese FM patients according to a “Life Support-Based Comprehensive Treatment Regimen”, which emphasizes early and aggressive mechanical circulatory support (MCS), timely immunomodulatory therapy with essential doses of glucocorticoids and intravenous immunoglobulin (IVIG), and standardized supportive care. Importantly, cytotoxic immunosuppressive agents (e.g., azathioprine or cyclophosphamide) were not routinely administered unless specific indications, such as virus-negative inflammatory cardiomyopathy, were confirmed, and this regimen was associated with a dramatic reduction in in-hospital mortality[7-9]. However, investigations pertaining to long-term prognosis remain limited, especially lacking long-term follow-up data from China under Chinese guidelines. A study has pointed out that patients with FM have a higher long-term survival rate without the need for heart transplantation compared to those with non-fulminant myocarditis (NFM)[10]. However, this notion has been challenged by the study of Ammirati et al., which indicated that patients with FM exhibited higher long-term mortality and increased heart transplant rates in comparison to those with NFM[11,12].
Consequently, the true picture remains unclear. This study seeks to address this gap by examining cardiogenic death, heart transplantation, and the heart’s function and structure in patients with FM versus those with NFM over a long-term follow-up period in China, under Chinese guidelines[13].
METHODS
Study design and population
This study was conducted as a prospective, multicenter cohort study. Five tertiary hospitals located in China collaborated in the research and gathered pertinent cases. The project received approval from the Institutional Review Board at Tongji Hospital during its meeting on February 2, 2016, and was assigned the unique identifier TJ-C20160202 (the research in this paper meets the ethical standards of the project). All participating centers secured local Institutional Review Board approval for the enrollment of patients with FM and NFM. The study strictly adhered to the ethical guidelines in the Declaration of Helsinki and the International Conference on Harmonization Guidelines for Good Clinical Practice.
Given the absence of a universally accepted definition of FM, previous studies have used heterogeneous criteria. Some investigations have defined FM primarily based on clinical presentation requiring inotropes or MCS[14,15], which may introduce subjectivity due to treatment-related decision-making and institutional practice variation. To improve objectivity and reproducibility, we adopted criteria grounded in the 2013 European Society of Cardiology (ESC) Working Group Position Statement and further incorporated quantitative indicators of disease severity, including: (1) hemodynamic compromise requiring MCS or vasoactive drugs; and (2) at least one of the following objective markers: diffuse myocardial edema on cardiac magnetic resonance (≥ 50% ventricular segments with T2 ratio ≥ 2.0) or early multiorgan failure [sequential organ failure assessment (SOFA) score ≥ 2 in ≥ 2 systems within 72 h]. This composite definition was designed to reflect both the acute hemodynamic instability and the systemic inflammatory severity characteristic of FM. NFM required: Acute myocarditis cases (symptom duration < 4 weeks) not meeting FM criteria. Among the patients who consented to undergo endomyocardial biopsy (EMB), we proceeded with the examination to obtain a more definitive diagnosis and provide pathological information.
Patients with FM and NFM were consistently enrolled in the study from April 1, 2016, to December 31, 2024. The inclusion criteria for this study were as follows: (1) Histological confirmation of acute myocarditis in accordance with the Dallas criteria[16] or alternatively, myocarditis confirmed by cardiac magnetic resonance (CMR) imaging based on the Lake Louise Criteria (LLC 2009)[17]; (2) Acute presentation of the disease, defined as the onset of cardiac symptoms within 30 days prior to hospital admission; (3) The treatment provided during hospitalization must adhere to the identical standards established by Tongji Hospital. The exclusion criteria of this study were as follows: (1) Patients who died during hospitalization; (2) Patients with any other disease that could potentially cause changes in the structure and function of the heart.
Study endpoint and patient follow-up
The primary composite endpoint included long-term (greater than 1 month, not paying attention to the situation during the hospitalization period) cardiovascular death, heart transplantation, chronic heart failure {defined as left ventricular ejection fraction < 50% with New York Heart Association [NYHA] class ≥ II}[18], and structural cardiac abnormalities (left ventricular end-diastolic diameter > 5.5 cm or left atrial diameter > 4 cm for males; > 5.0 cm or > 3.5 cm for females, respectively). All cardiac structural measurements were obtained through standardized transthoracic echocardiography performed by experienced sonographers according to current guidelines[19]. The secondary endpoint focused on persistent troponin elevation
All patients were scheduled for outpatient follow-up visits at intervals: 1 month, 3 months, 6 months, and
Statistical analysis
This study aimed to compare the incidence of primary endpoint events between patients with FM and those with NFM. Based on historical clinical data from Tongji Hospital, the incidence of primary outcome events was 45% among FM and 30% among NFM. The study was designed with a significance level of 0.05, a power of 80%, and a 1:1 ratio for the two groups. For the two-sided test, the sample size was calculated using[20,21]:
Where Zα represents the Z-score corresponding to the significance level (α = 0.05), Zβ represents the Z-score corresponding to the power of 80% (β = 0.20), p1 and p2 are the proportions of the primary outcome event in the FM and NFM groups, respectively, and q = 1 − p, where p refers to an average proportion of the primary outcome event. This formula was used to determine the required sample size for the study. The result indicating that the required sample size for each group is n = 163, leading to a total sample size of 326 for the study, was determined through statistical calculations.
Considering a 5% patient dropout rate, we should enroll 344 patients. Additionally, since this study primarily calculates hazards risk based on regression analysis, it is necessary to ensure at least 10 events per variable (EPV) for modeling. Based on the directed acyclic graph (DAG), we plan to adjust for a maximum of
After discovering that the missing data amounted to less than 5% and was determined to be Missing at Random, we opted for multiple imputation utilizing the predictive mean matching method[22,23].
Continuous variables were presented as median with interquartile range (IQR) for non-normally distributed data. To assess statistical differences between groups, we employed the Mann-Whitney U test for non-normally distributed variables. Categorical variables were summarized using frequencies (percentages) and compared between groups using the Chi-square (χ2) test or Fisher’s exact test, depending on their applicability. A two-sided P-value of less than 0.05 was deemed statistically significant in all cases.
Main analysis: Recognizing the limitations of purely data-driven variable selection strategies (e.g., selecting covariates based on statistical significance in univariate analyses), we adopted a causal inference framework using DAGs based on prior clinical knowledge and published literature. DAGs allow explicit specification of assumed causal relationships between exposure, confounders, mediators, and outcomes[24,25]. This approach helps avoid inappropriate adjustment for mediators or collider variables, which may otherwise introduce bias. Therefore, age and sex were identified as minimal sufficient adjustment variables, while variables such as treatment strategies, complications, and laboratory markers were considered potential mediators and were not included in the primary adjusted model. Three models were constructed: Model 1 (Crude): Isolated association between myocarditis type (FM vs. NFM) and outcomes. Model 2 (Minimally Adjusted): Incorporated age and sex as the confounders (primary analysis). Model 3 (Comprehensive adjusted): Evaluated time from onset to hospital admission (TFOHA) given its dual potential as either a mediator or context-dependent confounder. Several clinically relevant variables, including length of stay (LOS), complications, laboratory parameters, and treatment strategies, were intentionally excluded from adjustment as they were identified through DAG as likely mediators (consequences rather than causes of myocarditis severity). Treatment strategies were particularly avoided as covariates since they represent confounding by indication, being intrinsically linked to the underlying disease severity or type of myocarditis.
Supplementary analyses: Survival analyses were performed using Kaplan-Meier curves with log-rank testing for unadjusted comparisons between groups. To account for potential confounding, we adopted a two-stage modeling approach: First, covariates were screened through univariate Cox regression (significance threshold P < 0.05). Significant predictors were then incorporated into multivariate Cox proportional hazards models to estimate adjusted HR with 95% confidence intervals (CIs). For secondary outcomes, we similarly employed univariate followed by multivariate logistic regression to derive adjusted odds ratios (ORs) with 95%CI. For the primary outcome only, subgroup analyses were performed, including variables such as age, sex, TFOHA, LOS, smoking status, drinking status, and cardiac troponin I at admission.
Explore analyses: Given the potential association between persistent troponin elevation and primary outcomes, we conducted comprehensive exploratory analyses. These included multi-model adjusted Cox regression and Kaplan-Meier survival analyses treating persistent troponin elevation (secondary outcome) as an independent variable and the composite primary endpoint as the dependent variable. We further quantified this relationship using restricted cubic splines (RCS) to allow for non-linear associations.
Sensitivity analyses: To assess the robustness of our findings, we performed sensitivity analyses in two distinct subpopulations: (1) The age-restricted cohort (≥ 15 years) to minimize developmental confounding; (2) A propensity score-matched (PSM) cohort [1:1 matching on age and sex with a caliper width of
RESULTS
Study population
Figure 1 outlines the process of patient inclusion, screening, and follow-up. Among all the patients initially included, 13 individuals (all with FM) died due to cardiovascular causes. The final analysis enrolled
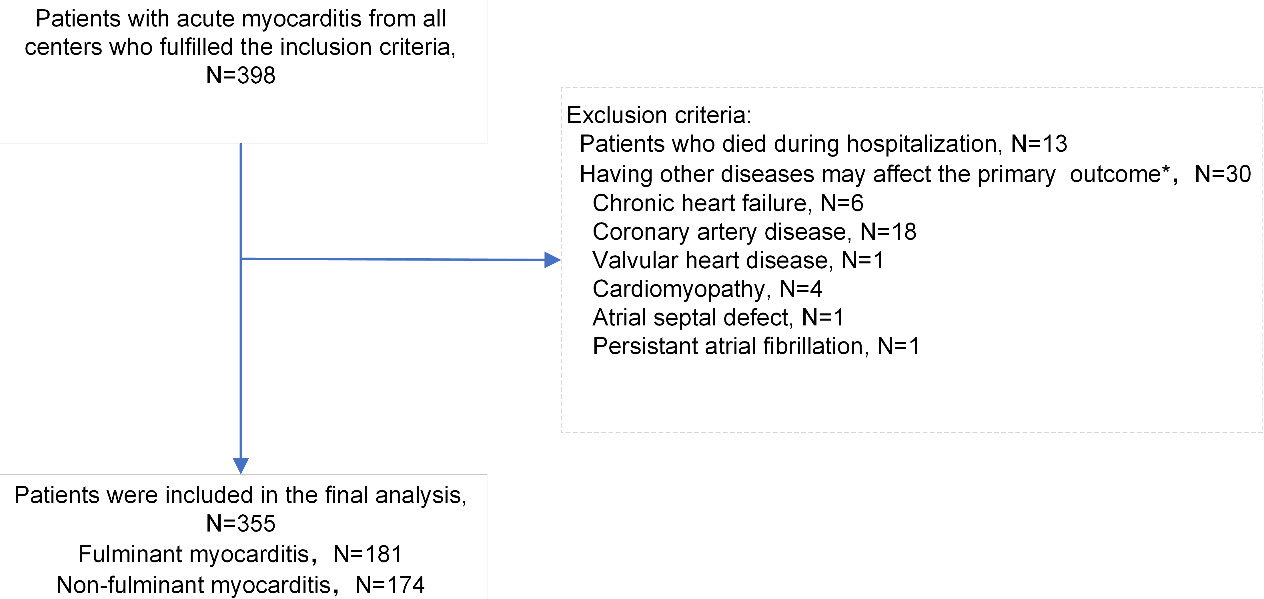
Figure 1. Flow diagram illustrating the selection of patients included in the entire cohort. * The primary composite endpoint included cardiovascular death, heart transplantation, chronic heart failure {defined as left ventricular ejection fraction < 50% with New York Heart Association [NYHA] class ≥ II}, and structural cardiac abnormalities (left ventricular end-diastolic diameter > 5.5 cm or left atrial diameter > 4 cm for males; > 5.0 cm or > 3.5 cm for females, respectively). A total of 30 patients were included in the category “Having other diseases may affect the primary outcome”. The sum of the subcategories is 31 because one patient suffered from both chronic heart failure and coronary artery disease.
Clinical characteristics of patients admitted with proven FM and NFM
| Characteristics | FM (181) | NFM (174) | P |
| Female | 93 (51.4) | 42 (24.1) | < 0.001 |
| Age, y | 34.00 [21.00, 50.00] | 23.50 [17.00, 37.75] | < 0.001 |
| TFOHA, d | 3.00 [2.00, 6.00] | 3.00 [1.25, 4.00] | 0.005 |
| LOS, d | 12.00 [9.00, 16.00] | 7.00 [5.00, 9.75] | < 0.001 |
| Smoking status | 0.49 | ||
| Never | 148 (81.8) | 148 (85.1) | |
| Former or current | 33 (18.2) | 26 (14.9) | |
| Drinking status | 0.761 | ||
| Never | 167 (92.3) | 158 (90.8) | |
| Former or current | 14 (7.7) | 16 (9.2) | |
| ECG at admission | |||
| ST-T segment abnormalities | 125 (69.1) | 67 (38.5) | < 0.001 |
| Advanced AV block | 34 (18.8) | 2 (1.1) | < 0.001 |
| VT/VF | 20 (11.0) | 0 (0.0) | < 0.001 |
| Cardiac arrest | 18 (9.9) | 0 (0.0) | < 0.001 |
| Echocardiography at admission | |||
| LVEF | 30.00 [24.00, 45.00] | 57.00 [51.00, 61.00] | < 0.001 |
| Admission laboratory tests | |||
| cTnI, pg/mL | 19249.20 [3875.20, 43350.70] | 2996.50 [506.42, 8632.97] | < 0.001 |
| NT-proBNP, pg/mL | 5402.00 [2029.00, 10620.00] | 469.00 [183.25, 1304.75] | < 0.001 |
| ALT, U/L | 57.00 [30.00, 143.00] | 25.00 [18.00, 43.00] | < 0.001 |
| AST, U/L | 136.00 [64.00, 289.00] | 47.50 [30.00, 86.75] | < 0.001 |
| Scr, umol/L | 77.00 [61.00, 106.00] | 72.00 [61.00, 87.00] | 0.079 |
| Serum potassium, mmol/L | 4.18 [3.82, 4.55] | 3.95 [3.72, 4.26] | < 0.001 |
| LDH, U/L | 487.00 [318.00, 764.00] | 250.00 [181.50, 335.00] | < 0.001 |
| CRP, mg/L | 27.50 [8.00, 76.70] | 14.65 [4.05, 54.62] | 0.008 |
| ESR, mm/H | 9.00 [5.00, 19.00] | 8.00 [4.00, 16.00] | 0.125 |
| CMR* | 160 (88.4) | 151 (86.8) | 0.764 |
| EMB& | 70 (38.7) | 46 (26.4) | 0.019 |
| Primary outcome$ | 89 (49.2) | 63 (36.2) | 0.018 |
| Time to event | 18.00 [6.00, 48.00] | 36.00 [6.00, 54.00] | 0.007 |
| Secondary outcome# | 71 (39.2) | 26 (14.9) | < 0.001 |
Supplementary Table 1 provides detailed clinical profiles of patients who reached the composite endpoint of cardiovascular death or heart transplantation.
Table 2 illustrates the treatment strategies employed for patients during their hospital stay. In comparison to the NFM group, the FM group exhibited a significantly higher utilization of intra-aortic balloon pump (IABP), with 169 (93.4%) versus 0 patients, P < 0.001. Similarly, a higher proportion of patients in the FM group used extracorporeal membrane oxygenation (ECMO), specifically 55 (30.4%) compared with 0 patients in the NFM group, P < 0.001. Moreover, a higher proportion of patients received immunoglobulin treatment in the FM group (136, 96.5%) compared to the NFM group (106, 73.1%), P < 0.001. Similarly, a greater number of patients in the FM group received glucocorticoids with 140 patients (99.3%) compared to 130 patients (89.7%), P = 0.001.
In-hospital treatment in patients admitted with proven FM and acute NFM
| Characteristics | FM (181) | NFM (174) | P |
| Temporary MCS devices | |||
| IABP | 169 (93.4) | 0 (0.0) | < 0.001 |
| Days | 5.00 [3.00, 7.00] | 0.00 [0.00, 0.00] | < 0.001 |
| ECMO | 55 (30.4) | 0 (0.0) | < 0.001 |
| Days | 0.00 [0.00, 3.00] | 0.00 [0.00, 0.00] | < 0.001 |
| Pacemaker | 61 (33.7) | 0 (0.0) | < 0.001 |
| Days | 0.00 [0.00, 4.00] | 0.00 [0.00, 0.00] | < 0.001 |
| Other support devices | |||
| CRRT | 45 (24.9) | 1 (0.6) | < 0.001 |
| Hours | 0.00 [0.00, 0.00] | 0.00 [0.00, 0.00] | < 0.001 |
| CPR/Defibrillation | 28 (15.5) | 0 (0.0) | < 0.001 |
| Immunoregulatory therapy | |||
| Immunoglobulin | 178 (98.3) | 119 (68.4) | < 0.001 |
| Glucocorticoids | 181 (100.0) | 152 (87.4) | < 0.001 |
| Other drugs therapy | |||
| Inotropes | 97 (53.6) | 0 (0.0) | < 0.001 |
| Antiviral drugs | 175 (96.7) | 147 (84.5) | < 0.001 |
| ACEI/ARB | 115 (63.5) | 79 (45.4) | 0.001 |
| Beta blockers * | 109 (60.2) | 91 (52.3) | 0.162 |
Regression analysis of primary and secondary outcomes
To better differentiate confounders from mediators, we developed a DAG [Supplementary Figure 1] and employed a multi-model adjustment approach as the main analysis. In the unadjusted model (Model 1), patients with FM demonstrated a significantly higher risk of the primary outcome compared to NFM patients (HR 1.52, 95%CI 1.10-2.11). After adjustment for sex and age in Model 2, the association attenuated to a marginal risk increase (adjusted HR 1.40, 95%CI 1.00-1.97), which was no longer statistically significant. Further adjustment for TFOHA in Model 3 yielded an HR of 1.57 (95%CI 0.97 to 2.52), maintaining the non-significant trend [Figure 2A]. For the secondary outcome, all three models demonstrated consistent statistically significant trends. After adjustment for sex, age, and TFOHA, the OR was 3.44 (95%CI 2.01-6.03). Detailed results are presented in Figure 2B.
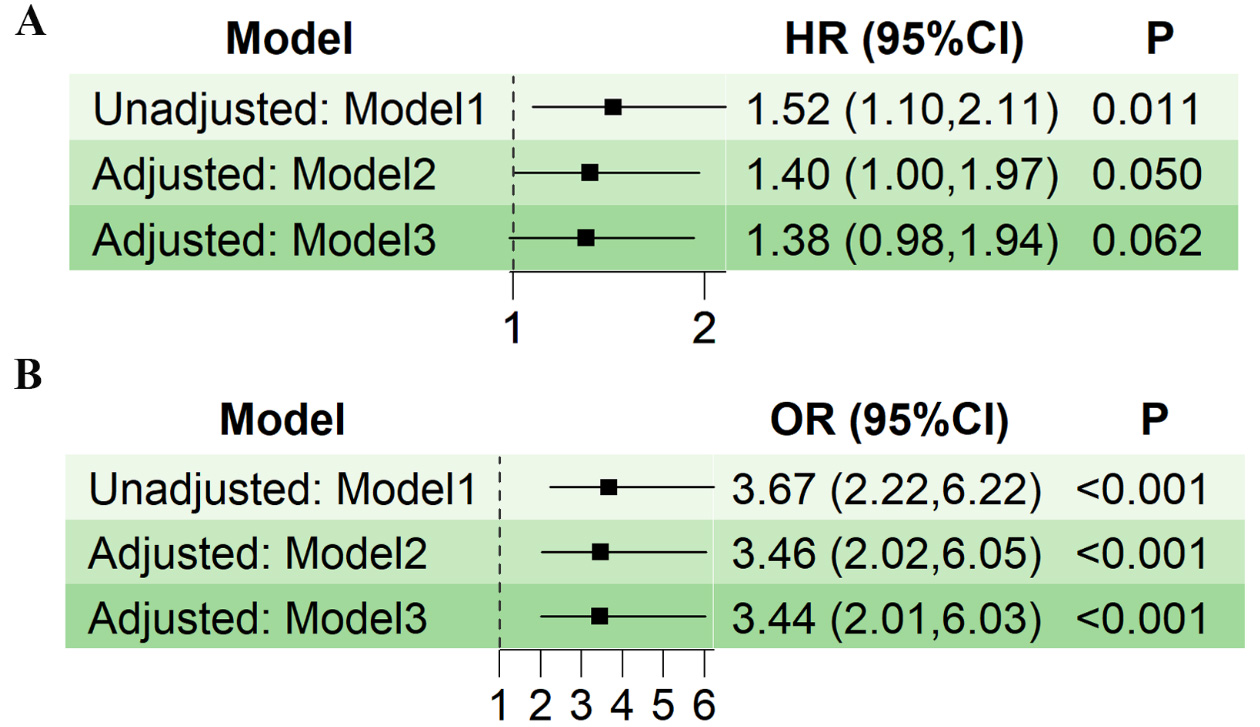
Figure 2. Forest plots comparing outcomes between fulminant and non-fulminant myocarditis using progressively adjusted models. Model 1 shows unadjusted associations, Model 2 adjusts for age and sex, and Model 3 additionally incorporates time from symptom onset to hospitalization. Analyses employed marginal effect Cox regression (for time-to-event outcomes) and logistic regression (for binary endpoints), with robust variance estimation to account for study-level clustering. Results are presented as hazard ratio (HR) or odds ratio (OR) with 95% confidence interval (CI). (A) The primary outcome is examined in the entirety of the patient population; (B) The secondary outcome is evaluated in the entirety of the patient population.
In supplementary analyses, survival analysis demonstrates a significantly higher risk of the primary composite endpoint in FM patients than in NFM patients (log-rank P = 0.010; Figure 3). The detailed information of univariate and multivariate regression is presented in Table 3. Compared with NFM, the initial HR and 95%CI of FM patients were 1.52 (1.10 to 2.11) for primary outcome. However, after multivariate adjustment, the HR and 95%CI changed to 0.90 (0.35 to 2.30). For the secondary outcome, FM patients initially exhibited a higher risk, with an OR and 95%CI of 3.67 (2.22 to 6.22). After multivariate adjustment, the OR and 95%CI were 1.61 (0.73 to 3.54), which was not significant. We believe that data-driven methods may lead to over-adjustment, while the results based on the DAG are more accurate.
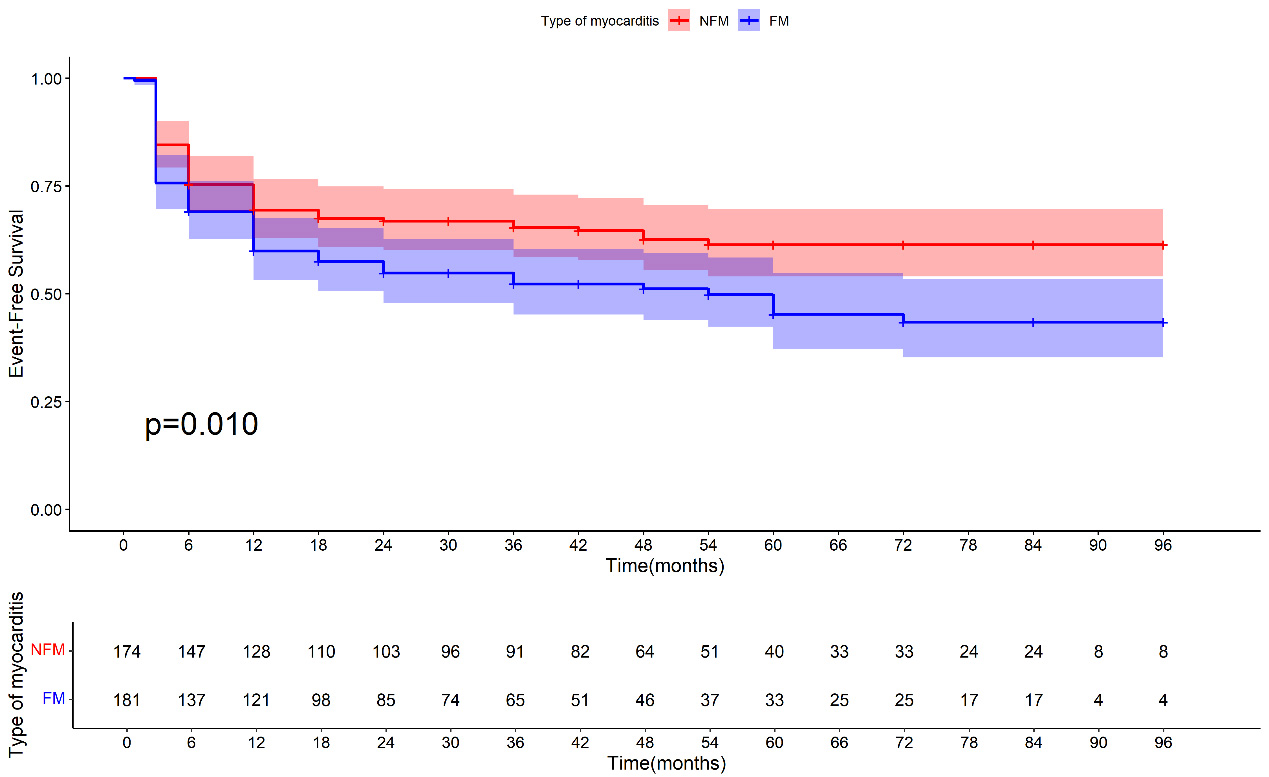
Figure 3. Survival analysis of the primary outcome of fulminant myocarditis (FM) versus non-fulminant myocarditis (NFM) in all patients.
Univariate and multivariate analyses of predictors for primary and secondary outcomes
| Characteristics | HR (95%CI) for primary outcome | OR (95%CI) for secondary outcome | ||
| Univariate | Multivariate | Univariate | Multivariate | |
| FM | 1.52 (1.10-2.11) * | 0.90 (0.35-2.30) | 3.67 (2.22-6.22) * | 2.20 (0.48-8.81) |
| Male | 1.26 (0.90-1.77) | 0.78 (0.48-1.26) | ||
| Age, per 1 year | 1.03 (1.02-1.04) * | 1.03 (1.02-1.04) * | 1.03 (1.01-1.04) * | 1.02 (1.00-1.04)* |
| TFOHA, per 1 day | 1.02 (1.00-1.05) | 1.02 (0.98-1.06) | ||
| LOS, per 1 day | 1.02 (1.01-1.05) * | 1.01 (0.98-1.04) | 0.99 (0.51-1.82) | |
| Smoking status | ||||
| Never | 1.00 (reference) | 1.00 (reference) | ||
| Former or current | 2.01 (1.39-2.90) * | 1.45 (0.99-2.13) | 0.99 (0.51-1.82) | |
| Drinking status | ||||
| Never | 1.00 (reference) | 1.00 (reference) | ||
| Former or current | 1.27 (0.76-2.13) | 0.38 (0.11-1.02) | ||
| ECG at admission | ||||
| ST-T segment abnormalities | 1.48 (1.07-2.05) * | 1.24 (0.87-1.75) | 1.74 (1.08-2.84) * | 1.17 (0.67-2.03) |
| Advanced AV block | 0.95 (0.56-1.61) | 2.06 (1.00-4.17) * | 1.79 (0.69-4.62) | |
| VT/VF | 0.90 (0.49-1.66) | 1.13 (0.45-2.59) | ||
| Cardiac arrest | 1.17 (0.61-2.22) | 2.54 (0.98-6.49) | ||
| Echocardiography at admission | ||||
| LVEF, per 1% | 0.98 (0.97-0.99) * | 0.99 (0.98-1.01) | 0.97 (0.95-0.98) * | 0.82 (0.98-1.02) |
| Admission laboratory tests | ||||
| cTnI, per 1000 pg/mL | 1.02 (1.01-1.03) * | 1.01 (1.00-1.03) * | 1.04 (1.02-1.05) * | 1.03 (1.01-1.05) * |
| NT-proBNP, per 1000 pg/mL | 1.03 (1.01-1.04) * | 1.00 (0.98-1.02) | 1.07 (1.04-1.10) * | 1.04 (1.01-1.08) * |
| ALT, per 1000 U/L | 0.96 (0.72-1.20) | 1.20 (0.89-1.53) | ||
| AST, per 1000 U/L | 0.96 (0.81-1.12) | 1.11 (0.91-1.31) | ||
| Scr, per 10 umol/L | 0.98 (0.96-1.00) | 1.01 (1.00-1.03) | ||
| Serum potassium, per 1 mmol/L | 1.05 (0.76-1.44) | 1.05 (0.66-1.65) | ||
| LDH, per 1000 U/L | 1.73 (1.40-2.06) * | 1.16 (0.70-1.62) | 2.13 (1.56-2.71) * | 0.92 (0.13-1.69) |
| CRP, per 10 mg/L | 1.02 (1.00-1.04) | 1.00 (0.97-1.04) | ||
| ESR, per 10 mm/H | 1.04 (0.96-1.11) | 1.04 (0.93-1.16) | ||
| Therapy | ||||
| IABP | 1.52 (1.11-2.10) * | 0.71 (0.28-1.81) | 3.42 (2.09-5.68) * | 0.89 (0.24-3.79) |
| ECMO | 1.67 (1.12-2.47) * | 1.23 (0.72-2.13) | 1.65 (0.89-3.02) | |
| Pacemaker | 1.45 (0.99-2.13) | 1.96 (1.09-3.49) * | 0.57 (0.25-1.29) | |
| CRRT | 0.99 (0.63-1.56) | 1.50 (0.76-2.86) | ||
| CPR/Defibrillation | 0.82 (0.46-1.44) | 1.44 (0.65-3.06) | ||
| Intravenous immunoglobulin | 1.26 (0.81-1.96) | 2.81 (1.35-6.61) * | 1.27 (0.48-3.76) | |
| Glucocorticoids | 1.13 (0.57-2.21) | 4.21 (1.20-26.64) * | 1.54 (0.32-11.39) | |
| Inotropes | 1.35 (0.96-1.89) | 1.91 (1.16-3.13) * | 0.71 (0.37-1.35) | |
| Antiviral drugs | 1.28 (0.71-2.31) | 1.00 (0.46-2.36) | ||
| ACEI/ARB | 1.19 (0.86-1.64) | 1.19 (0.74-1.91) | ||
| Beta blockers | 0.97 (0.71-1.34) | 1.54 (0.96-2.51) | ||
Subgroup analyses for the primary outcome
To assess the consistency of results across clinically relevant variables, we performed prespecified analyses stratified by sex, age, TFOHA, LOS, smoking status, drinking status, and cardiac troponin I (cTnI). Continuous variables (age, TFOHA, LOS, cTnI) were dichotomized at median values. As shown in Figure 4, the direction of effect favored a consistent overall result across all subgroups, with no significant heterogeneity detected (all interaction P-values > 0.05).
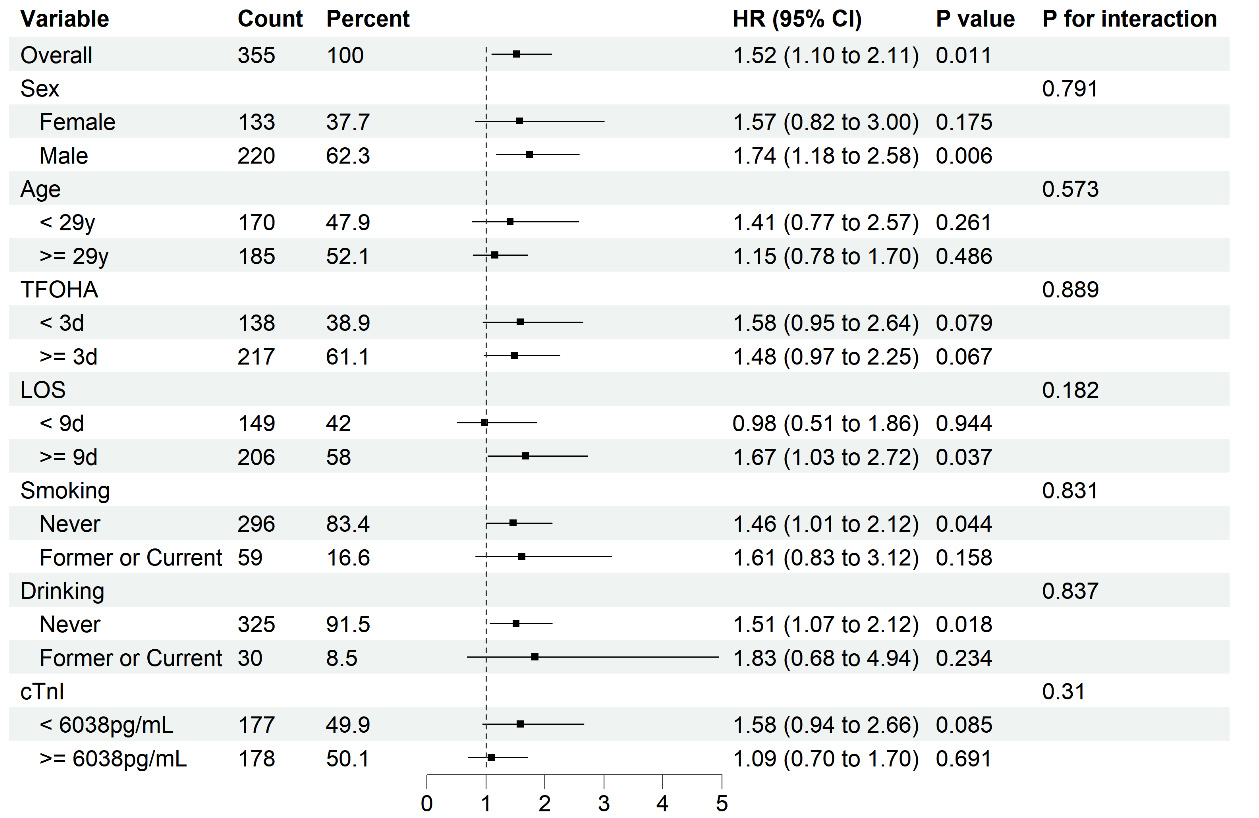
Figure 4. A subgroup analysis was conducted for the primary outcome in the entirety of the patient population (fulminant myocarditis vs. non-fulminant myocarditis). HR: Hazard ratio; CI: confidence interval; TFOHA: time from onset to hospital admission; LOS: length of stay; cTnI: Cardiac troponin I. All continuous variables were dichotomized at their median values.
Analysis of secondary and primary outcome association
Unadjusted analysis demonstrated that persistent troponin elevation (secondary outcome) was significantly associated with an increased risk of the primary composite endpoint (HR 1.97, 95%CI 1.42-2.74). This association remained significant after adjustment for age and sex (adjusted HR 1.66, 95%CI 1.18-2.33; Supplementary Figure 2).
Further analysis examined the log2-transformed average of two consecutive troponin measurements taken at 1-month post-discharge. A positive linear relationship was observed between troponin I levels and the risk of the primary outcome once troponin exceeded the upper limit of the normal reference range (34.2 pg/mL, log2-transformed value of 5). This dose-dependent association persisted in both unadjusted [Figure 5A] and adjusted models [Figure 5B].
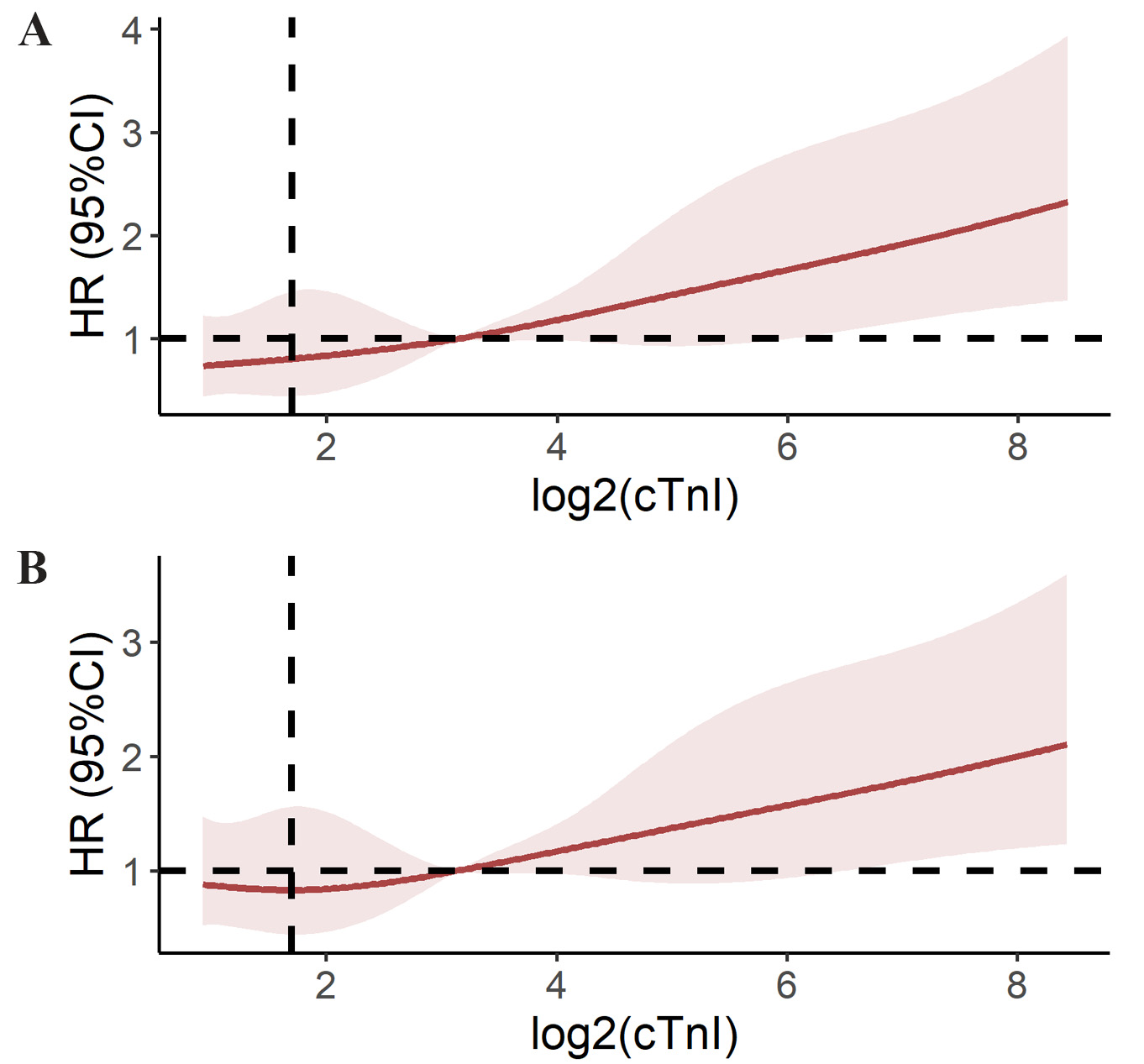
Figure 5. Restricted Cubic Spline (RCS) estimation depicting the hazards ratio (HR) between secondary (persistently elevated cardiac troponin I) and primary outcome. (A) Unadjusted estimation; (B) Estimation adjusted for age and sex. CI: Confidence interval; HR: hazard ratio; cTnI: Cardiac troponin I.
Sensitivity analyses
To address potential heterogeneity between pediatric and adult populations, we conducted analyses in patients aged ≥ 15 years. Supplementary Table 2 presents the baseline clinical characteristics of these adult patients, while Supplementary Table 3 details their treatment regimens. Unadjusted survival analysis [Supplementary Figure 3] demonstrated that FM patients maintained a significantly higher risk of developing the primary composite endpoint, consistent with findings in the overall population. This non-significant association remained robust after multi-model adjustment (Supplementary Figure 4A for primary outcome and Supplementary Figure 4B for secondary outcome). Similar results were observed in the relationship between secondary and primary outcomes [Supplementary Figure 5].
PSM based on DAG effectively balanced age and sex distributions between groups (other factors served as mediating variables and did not require balancing), as evidenced by the baseline characteristics and treatment details presented in Supplementary Tables 4 and 5. Survival analysis of the matched cohort showed no significant difference between groups (log-rank P = 0.084, Supplementary Figure 6). Subgroup analyses of the balanced population [Supplementary Figure 7] yielded results concordant with those from the overall cohort.
DISCUSSION
This prospective multicenter cohort study was designed to comprehensively compare long-term clinical outcomes between FM and NFM patients, addressing current knowledge gaps in the field. Specifically, it aims to clarify the long-term prognosis of Chinese FM patients treated according to Chinese clinical guidelines. The findings showed a statistically significant incidence (P = 0.018) of the primary composite endpoint in FM patients (89, 49.2%) versus NFM patients (63, 36.2%). However, after full adjustment, the result was marginal effect size (HR 1.38, 95%CI 0.98-1.94; P = 0.062), suggesting the need for cautious interpretation. Although negative results were consistently observed in both sensitivity analyses, we cannot exclude the possibility that these findings reflect insufficient statistical power rather than true equivalence. Post-hoc power analysis indicated only 70% power (30% probability of type II error), further emphasizing the need for careful consideration of these results[26]. These findings highlight the critical need for future studies with larger sample sizes and extended follow-up periods exceeding ten years to provide definitive conclusions.
In our study, with follow-up extending up to nine years, eight cases of cardiovascular death or heart transplantation were recorded, seven of which occurred in FM patients. Due to the limited number of events for this specific endpoint, we did not perform separate statistical analyses. McCarthy et al.[10] reported favorable long-term prognosis in FM patients compared to NFM patients, attributed to low rates of cardiovascular death or heart transplantation despite higher in-hospital mortality. However, this conclusion was drawn from a small cohort (15 FM vs. 132 NFM patients), with only one endpoint event observed in the FM group, suggesting substantial random variability in the results. Similarly, Lorusso et al.[27] proposed favorable prognosis in FM patients due to fewer cardiac-related events; however, their study lacked direct comparisons between FM and NFM patients, limiting its clinical relevance. A study has suggested comparable long-term survival between FM and NFM patients who survive the acute phase, but these were similarly constrained by small sample sizes (14 FM vs. 13 NFM patients), rendering their conclusions inconclusive[28].
In contrast, two studies by Ammirati et al.[11,12] demonstrated significantly higher risks of cardiovascular death or heart transplantation in FM versus NFM patients. These studies partially addressed prior limitations through larger sample sizes and multicenter designs. Ammirati et al.[11,12] defined FM largely on the basis of clinical presentation requiring inotropic or MCS, without incorporating organ dysfunction or imaging-based criteria. Similarly, the American Heart Association (AHA) scientific statement emphasizes rapid hemodynamic deterioration but does not mandate quantitative imaging or organ failure metrics[6]. Compared with these approaches, our composite criteria integrate hemodynamic instability, objective imaging findings, and early multiorgan dysfunction, thereby aiming to reduce misclassification and enhance consistency across centers. However, we acknowledge that differences in diagnostic criteria may affect cross-study comparability and should be considered when interpreting our findings. The observed higher risk of cardiovascular death or heart transplantation in FM patients aligns with the findings of Ammirati et al.[11,12] but is supported by more rigorous methodology. Additionally, our study provides novel data from a Chinese cohort, addressing the geographic gap in prior research.
Although chronic heart failure risk assessment was not pre-specified as a single end point, a descriptive analysis revealed that among 61 patients who developed chronic heart failure during follow-up, 48 cases (26.5%) were FM patients compared to 13 cases (7.5%) in NFM patients, demonstrating a substantially higher absolute events in the FM group. Prior research by Ammirati et al.[11] directly compared cardiac systolic function between FM and NFM patients. It suggests that while FM patients showed more significant LVEF improvement during hospitalization, their long-term follow-up revealed lower LVEF values compared to NFM patients. Our findings corroborate this observation and extend it by employing chronic heart failure (CHF) as a clinical endpoint that incorporates both LVEF assessment and symptomatic status (NYHA class ≥ II), thereby providing a more comprehensive evaluation of long-term cardiac dysfunction.
The favorable long-term trends observed in FM patients under the current regimen may be attributable to several key components of the “Life Support-Based Comprehensive Treatment Regimen”. First, early initiation of MCS (such as IABP or ECMO) likely plays a critical role in stabilizing hemodynamics during the acute inflammatory phase, thereby preventing irreversible end-organ damage and allowing myocardial recovery. Second, the use of immunomodulatory therapy with essential-dose glucocorticoids and IVIG may help attenuate excessive inflammatory responses without inducing profound immunosuppression[29]. Unlike cytotoxic immunosuppressive agents, which may increase infection risk and are generally reserved for biopsy-proven virus-negative inflammatory cardiomyopathy[8], our strategy focuses on immune modulation rather than broad immune suppression. Third, strict standardized supportive care and structured follow-up protocols may have contributed to improved long-term management of ventricular remodeling and heart failure progression. Nevertheless, given the observational design of our study, we cannot definitively determine the relative contribution of each treatment component. The improved long-term prognosis may reflect the synergistic effect of early hemodynamic stabilization and controlled immunomodulation rather than any single intervention alone. Future randomized or mechanistic studies are needed to clarify the individual and combined effects of these therapeutic strategies.
This research also examined the relationship between the secondary outcome (persistent elevation of cTnI for one month) and the primary outcome, given that previous research has linked persistent inflammatory activation to a poorer long-term prognosis[30]. The persistent elevation of cTnI is a marker of ongoing myocardial injury and active inflammation within the myocardium[30,31]. This prolonged inflammatory response and immune-mediated cardiac damage may ultimately contribute to the long-term deterioration of cardiac structure and function[32].
Currently, there is a lack of reliable biomarkers for predicting long-term cardiac structural and functional outcomes in patients with acute myocarditis. A study reported that peak troponin levels in patients with acute myocarditis correlated with more extensive late gadolinium enhancement on CMR imaging and lower LVEF during follow-up[33]. Another study found that initial admission cTnI levels were associated with progressive ventricular dysfunction in heart failure patients[34]. However, conflicting evidence exists, a study has shown no correlation between admission cTnI levels and late LVEF in myocarditis patients[35]. From a clinical perspective, our findings suggest that measurement of cTnI at 1-month follow-up may serve as a practical risk stratification tool. Patients with persistently elevated cTnI levels may benefit from closer surveillance, including more frequent outpatient visits, repeat echocardiographic assessment, and careful monitoring for symptoms of heart failure or ventricular remodeling. In selected high-risk individuals, clinicians may consider optimization of guideline-directed medical therapy for heart failure and closer rhythm monitoring. Conversely, patients with normalized cTnI levels at one month may be considered at relatively lower risk and could potentially follow a standard follow-up schedule. However, these recommendations are hypothesis-generating and should be interpreted cautiously. Given the observational design of our study, the prognostic value of 1-month troponin measurement requires prospective validation in independent cohorts before it can be formally incorporated into clinical decision-making algorithms.
Study limitations
Firstly, EMB was not conducted for all patients in this study. However, despite expert consensus and other statements recommending EMB for patients with acute myocarditis to guide diagnosis or treatment decisions[1,36], this recommendation has not been confirmed through large-scale clinical trials. Historical research also indicates a relatively low rate of EMB completion. For instance, Ammirati et al.[11] reported that only 26.7% of patients with acute myocarditis underwent EMB, while in a multicenter study, EMB was performed in 183 (44%) suspected FM patients[37]. Similarly, a Japanese single-center study of 22 patients did not include EMB[38]. Compared to these previous studies, our research has made progress in addressing this limitation.
Secondly, our study did not incorporate molecular analysis using gene test, and immunohistochemistry on myocardial biopsy tissue samples was not performed in all centers. This was primarily due to a lack of compelling evidence supporting the use of these procedures, as well as financial constraints faced by the research team.
Thirdly, while our sample size met pre-specified power calculations, it remained insufficient to definitively exclude modest but clinically important risk differences (particularly for rare outcomes such as heart transplantation). This limitation underscores the need for larger, collaborative studies to validate these findings.
Conclusions
Our study demonstrates that patients with FM under the current treatment regimen based on Chinese guidelines did not show a significantly increased long-term risk of the primary composite endpoints (cardiovascular death, heart transplantation, chronic heart failure, and cardiac structural abnormalities) compared with NFM patients. However, it should be noted that, given the borderline P value and the limited statistical power, this finding should be interpreted with caution. Notably, FM patients had a substantially higher incidence of persistent cTnI elevation at one-month follow-up than NFM patients. In both FM and NFM groups, persistent cTnI elevation was associated with an increased risk of developing the primary composite endpoints, with the magnitude of risk showing a positive correlation with the degree of cTnI elevation.
DECLARATIONS
Authors’ contribution
Contributed to the conception or design of the work: Wang DW, Jiang J
Drafted the manuscript: Jiang J, Li G
Completed the data analysis: Li G
Data collection and follow-up and at each center: Li Z, Zhang J, Xu Z, Ning Y, Zhang L
Data quality control: Cui G, Li R, Wang H, Wang DW, Jiang J
Availability of data and materials
The data supporting the findings of this article will be made available upon reasonable request to the corresponding author.
AI and AI-assisted tools statement
Not applicable.
Financial support and sponsorship
This work was supported by Projects from the National Natural Science Foundation of China (nos. 82241034, 82330010), Tongji Hospital affiliated to Tongji Medical College of Huazhong University of Science and Technology, the State Key Laboratory for Diagnosis and Treatment of Severe Infectious Diseases (2024ZZ00016), and the National Natural Science Foundation of China (82330010).
Conflicts of interest
Wang DW is a Consulting Editor of The Journal of Cardiovascular Aging. Wang DW was not involved in any steps of editorial processing, notably including reviewers’ selection, manuscript handling, or decision-making. The other authors declare that there are no conflicts of interest.
Ethical approval and consent to participate
This study was approved by the Institutional Review Board of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, on February 2, 2016 (approval number: TJ-C20160202). All participating centers obtained local Institutional Review Board approval prior to patient enrollment. The study adhered to the ethical guidelines set out in the Declaration of Helsinki. Informed consent was obtained from all participants or their legal guardians before inclusion in the study.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
Supplementary Materials
REFERENCES
1. Caforio ALP, Pankuweit S, Arbustini E, et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2013;34:2636-48.
2. Nagai T, Inomata T, Kohno T, et al. ; on behalf of the Japanese Circulation Society Joint Working Group. JCS 2023 guideline on the diagnosis and treatment of myocarditis. Circ J. 2023;87:674-754.
3. Barhoum P, Pineton De Chambrun M, Dorgham K, et al. Phenotypic heterogeneity of fulminant COVID-19--related myocarditis in adults. J Am Coll Cardiol. 2022;80:299-312.
4. Li G, Zhang J, Xu Z, et al. Long-term left ventricular ejection function in fulminant and non-fulminant myocarditis: a multicenter study in China. IJC Heart & Vasculature. 2025;59:101738.
5. Kanaoka K, Onoue K, Terasaki S, et al. Features and outcomes of histologically proven myocarditis with fulminant presentation. Circulation. 2022;146:1425-33.
6. Kociol RD, Cooper LT, Fang JC, et al. ; On behalf of the American Heart Association Heart Failure and Transplantation Committee of the Council on Clinical Cardiology. Recognition and initial management of fulminant myocarditis: a scientific statement from the American Heart Association. Circulation. 2020;141.
7. He W, Zhou L, Xu K, et al. Immunopathogenesis and immunomodulatory therapy for myocarditis. Sci. China Life Sci. 2023;66:2112-37.
8. Chimenti C, Russo MA, Frustaci A. Immunosuppressive therapy in virus-negative inflammatory cardiomyopathy: 20-year follow-up of the TIMIC trial. Eur Heart J. 2022;43:3463-73.
9. Li S, Xu S, Li C, et al. A life support-based comprehensive treatment regimen dramatically lowers the in-hospital mortality of patients with fulminant myocarditis: a multiple center study. Sci. China Life Sci. 2019;62:369-80.
10. Mccarthy RE, Boehmer JP, Hruban RH, et al. Long-term outcome of fulminant myocarditis as compared with acute (nonfulminant) myocarditis. N Engl J Med. 2000;342:690-5.
11. Ammirati E, Cipriani M, Lilliu M, et al. Survival and left ventricular function changes in fulminant versus nonfulminant acute myocarditis. Circulation. 2017;136:529-45.
12. Ammirati E, Veronese G, Brambatti M, et al. Fulminant versus acute nonfulminant myocarditis in patients with left ventricular systolic dysfunction. J Am Coll Cardiol. 2019;74:299-311.
13. Jiang J, Shu H, Wang DW, et al. ; Chinese Society of Cardiology, Chinese Medical Association, Writing Group. Chinese Society of Cardiology guidelines on the diagnosis and treatment of adult fulminant myocarditis. Sci. China Life Sci. 2024;67:913-39.
14. Schmidt M, Ponnaiah M, Huang F, et al. ; on behalf of the FULLMOON Study Group. Temporary mechanical support in fulminant myocarditis: prognostic factors and clinical implications from the FULLMOON study. Intensive Care Med. 2026;52:240-51.
15. D’ettore N, Eghbalzadeh K, Oezkur M, Bertoldi LF, Bossard M, Pappalardo F. Diagnosis and management of patients with fulminant myocarditis. Eur Heart J Suppl. 2025;27 Suppl:iv23-30.
17. Friedrich MG, Sechtem U, Schulz-menger J, et al. Cardiovascular magnetic resonance in myocarditis: a JACC white paper. J Am Coll Cardiol. 2009;53:1475-87.
18. Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;128:1810-52.
19. Wharton G, Steeds R, Allen J, et al. A minimum dataset for a standard adult transthoracic echocardiogram: a guideline protocol from the British Society of Echocardiography. Echo Res Pract. 2015;2:G9-G24.
20. Ziegel ER, Lemeshow S, Hosmer D, Klar J, Luanga S. Adequacy of sample size in health studies. J Health Stud. 1990;23:123-34. Available from: https://api.semanticscholar.org/CorpusID:123475116 [Last accessed on 20 May 2026].
22. Curnow E, Carpenter JR, Heron JE, et al. Multiple imputation of missing data under missing at random: compatible imputation models are not sufficient to avoid bias if they are mis-specified. J Clin Epidemiol. 2023;160:100-9.
23. Karuppasamy S, Premkumar PS, Mohan VR. Handling missing outcomes in time-to-event analyses in randomised controlled trials: a scoping review with a focus on multiple imputation. BMC Med Res Methodol. 2025;25:220.
24. Feeney T, Hartwig FP, Davies NM. How to use directed acyclic graphs: guide for clinical researchers. BMJ. 2025;388:e078226.
25. Ellison G, Rhoma H. Directed acyclic graphs as conceptual and analytical tools in applied and theoretical epidemiology: advances, setbacks and future possibilities. Math Biosci Eng. 2025;22:1280-306.
26. Quach NE, Yang K, Chen R, et al. Post‐hoc power analysis: a conceptually valid approach for power based on observed study data. Gen Psychiatry. 2022;35:e100764.
27. Lorusso R, Centofanti P, Gelsomino S, et al. Venoarterial Extracorporeal membrane oxygenation for acute fulminant myocarditis in adult patients: a 5-year multi-institutional experience. Ann Thorac Surg. 2016;101:919-26.
28. Asaumi Y, Yasuda S, Morii I, et al. Favourable clinical outcome in patients with cardiogenic shock due to fulminant myocarditis supported by percutaneous extracorporeal membrane oxygenation. Eur Heart J. 2005;26:2185-92.
29. Jain L, Kaur D, Khalil S, et al. Efficacy and safety of intravenous immunoglobulin (IVIg) in acute viral myocarditis in children: a systematic review. Indian Pediatr. 2025;62:56-62.
30. Ji M, Jiang L, Zhang Z, Jiang S, Zuo H. Novel insights into short-term troponin remeasurement and long-term cardiac function and structure following fulminant myocarditis. IJC Heart Vasc. 2025;60:101759.
31. Li G, Li Z, Li F, Jiang J. Predictors of long-term adverse course in acute myocarditis: a multicentre cohort study. Eur J Prev Cardiol. 2026;33:774-87.
32. Wang W, Jia H, Hua X, Song J. New insights gained from cellular landscape changes in myocarditis and inflammatory cardiomyopathy. Heart Fail Rev. 2024;29:883907.
33. Shyam-sundar V, Slabaugh G, Mohiddin SA, Petersen SE, Aung N. Clinical features, myocardial injury and systolic impairment in acute myocarditis. Open Heart. 2024;11:e002901.
34. Horwich TB, Patel J, Maclellan WR, Fonarow GC. Cardiac troponin I is associated with impaired hemodynamics, progressive left ventricular dysfunction, and increased mortality rates in advanced heart failure. Circulation. 2003;108:833-8.
35. Ammann P, Naegeli B, Schuiki E, et al. Long-term outcome of acute myocarditis is independent of cardiac enzyme release. Int J Cardiol. 2003;89:217-22.
36. Cooper LT, Baughman KL, Feldman AM, et al. The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology Endorsed by the Heart Failure Society of America and the Heart Failure Association of the European Society of Cardiology. Eur Heart J. 2007;28:3076-93.
37. Huang F, Ammirati E, Ponnaiah M, et al. ; for the FULLMOON Study Group. Fulminant myocarditis proven by early biopsy and outcomes. Eur Heart J. 2023;44:5110-24.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Special Topic
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].