


Global burden of liver cancer mortality due to alcohol use from 1990 to 2021 and predictions to 2050
 0
0 Abstract
Aim: This study aimed to explore the long-term mortality trends in the mortality burden of liver cancer due to alcohol use (LCA) from 1990 to 2021 and assess health inequalities stratified by sex and location, with projections to 2050. The contribution of population growth, age structure and epidemiologic changes to the increase in deaths will also be assessed.
Methods: Bayesian age-period-cohort model was applied to predict age-standardized mortality rate (ASMR). Bayesian spatiotemporal model was utilized to characterize the spatiotemporal distribution of ASMR. Frontier analysis assessed national prevention and control capacity. Decomposition analysis was performed to clarify driving factors of mortality growth.
Results: Global LCA ASMR presented an upward trend during 1990-2021 (AAPC = 0.35). Europe yielded the highest ASMR at 1.34, followed by Africa, while the Americas witnessed the fastest growth. National-level ASMR displayed obvious spatial clustering, with hotspots concentrated in West Africa, Southern Africa and partial Southeast Asian territories. Global LCA ASMR is projected to decline after 2022 and reach 0.93 by 2050. The Americas will undergo an initial rise followed by a subsequent drop in ASMR. Population aging will serve as the predominant driver of growing LCA mortality worldwide. Several nations including Brazil and Somalia are expected to attain relatively low ASMR by 2050.
Conclusion: LCA-related ASMR and health inequalities have aggravated across regions and countries. Targeted regional public health interventions are urgently required, particularly in the Americas and Africa.
Keywords
INTRODUCTION
Liver cancer (LC) ranks among the most common and lethal malignant tumors globally, with its disease burden steadily rising over recent decades[1]. Hepatitis B and C viruses constitute the leading etiological factors, while excessive alcohol consumption has emerged as an increasingly prominent driver, driven by prevalent alcohol abuse worldwide[2].
Alcohol triggers hepatocellular injury, persistent hepatic inflammation, fibrosis and cirrhosis, ultimately promoting malignant transformation[3]. Distinct from viral hepatitis, alcoholic liver disease progression is closely modulated by drinking habits and genetic susceptibility[4]. Its clinical spectrum covers asymptomatic early lesions to decompensated cirrhosis complicated with portal hypertension. Alcoholic liver disease generally advances more rapidly and is frequently diagnosed at advanced stages[5].
Unlike LC caused by viral hepatitis[6] and non-alcoholic fatty liver disease[7], LC due to alcohol use (LCA) features an occult onset, accompanied by limited therapeutic options and difficult early detection[8,9] compared with liver cancer induced by viral hepatitis and non-alcoholic fatty liver disease. Relevant prevention and management strategies remain underdeveloped. Given substantial interregional and international disparities in liver cancer burden, targeted intervention formulation faces great challenges[10]. Existing studies lack comprehensive assessments on LCA mortality patterns and geographic heterogeneity, particularly long-term projections. This study therefore analyzed three-decade LCA mortality trends and regional discrepancies, and predicted disease dynamics until 2050, aiming to furnish evidence for global public health policy design and preventive strategy optimization.
METHODS
Statistical analysis and data source
This study employed a range of statistical methods to analyze and forecast the age-standardized mortality rates (ASMR, per 100,000 persons) and LCA deaths at global, regional, national and gender levels from 1990 to 2021, with extended projections up to 2050. Derived from the Global Burden of Disease (GBD) 2021 dataset, the Bayesian age-period-cohort model was adopted to predict LCA ASMR across six World Health Organization (WHO) geographical regions and 204 countries and territories during 2022-2050. The average annual percent change (AAPC) was calculated to quantify temporal variations in ASMR. The Bayesian spatiotemporal model was further applied to characterize ASMR trends in 1990-2021 and 2022-2050, accounting for three variation sources: geographical spatial correlation, long-term temporal tendency and annual random fluctuations among individual nations. Frontier analysis was performed to evaluate national performance and room for improvement in LCA mortality reduction. Decomposition analysis was utilized to quantify the respective contributions of population aging, population growth and epidemiological shifts to mortality fluctuations across WHO regions. All statistical analyses, including the Bayesian age-period-cohort (BAPC), Bayesian spatiotemporal model, frontier analysis, and decomposition analysis, were performed using R software (version 4.3.0). All figures in this study were generated using the same R version, primarily utilizing the “ggplot2” and “sf” packages for data visualization and mapping. Additionally, the calculation of AAPC was conducted using the Joinpoint Program (version 4.9). Detailed methods are presented in subsequent sections and supplementary materials.
Bayesian spatiotemporal model
We analyzed the temporal trends and spatial distribution of ASMR for LCA across 204 countries and territories using Bayesian spatio-temporal models[11], which were developed based on observed ASMR from 1990 to 2021 and predicted ASMR from 2022 to 2050. Take the 1990-2021 analysis for example, yit denoted the ASMR in year t (t = 1990, 1991, ···, 2021) of the ith (i = 1, 2, ···, 204) country/territory, let yit~Normal(μit, σ2), then μit can be expressed as the formula:
μit = α + Si + θt + δit.
α was the intercept measuring the overall yit over the 1990-2021. Si represented the spatial effect, with Si > 0 indicating the ASMR of ith country/territory was above the overall level during the period. θt represented the temporal effect, which captured the overall dynamic temporal trend common to all countries. δit is the spatiotemporal interaction random effect, reflecting the remaining local dynamic characteristic of ith country in year t that cannot be explained adequately by Si and θt. A growing δit indicated that the upward trend of the ith country was stronger than the overall upward trend or the downward trend was weaker than the overall downward trend, and a decreasing trend was just the opposite. The further details were shown in Supplementary Methods.
Frontier analysis
Frontier analysis was applied to assess national efficiency and improvement potential in lowering LCA-related ASMR. Based on the projected ASMR data of 204 countries and territories in 2050, data envelopment analysis (DEA) and free disposal hull model were adopted for relevant evaluation[11] [Supplementary Methods]. The sociodemographic index (SDI) was conducted to reflect the comprehensive national development level.
RESULTS
The ASMR and AAPC for LCA stratified by sex, region, SDI, income, and health system level during 1990-2021
From 1990 to 2021, the ASMR of LCA increased worldwide (AAPC = 0.35, 95%CI: 0.22-0.48). For six WHO regions, ASMR of LCA decreased in the African region (AAPC = -0.48, 95%CI: -0.55 to -0.42), and was stable in the Western Pacific region (AAPC = -0.23, 95%CI: -0.69-0.24), while the other four regions showed an upward trend [Figure 1]. The African region had the highest ASMR in 1990 and carried the fastest decline during 1990-2021 (AAPC = -0.48, 95%CI: -0.55 to -0.42), while the Americas region experienced the fastest-growing ASMR (AAPC = 1.78, 95%CI: 1.45-2.11). In 2021, the European region had the highest ASMR of LCA among males, whereas the Eastern Mediterranean region had the lowest. Females in the African region sustained the highest ASMR over the past three decades [Table 1]. The high SDI quintile consistently had the highest LCA deaths, whereas the quintile with the highest ASMR shifted from the low SDI in 1990 to high SDI in 2021. Among females, the middle SDI quintile had the highest deaths, and the low SDI quintile had the highest ASMR. For males, both deaths and ASMR of LCA remained the highest in the high SDI quintile [Table 1]. Geographically, the region with the highest ASMR of LCA transitioned from Africa to Europe. In terms of health system levels, regions with limited health systems had the lowest ASMR, while those with minimal health system capacity exhibited the highest ASMR. From the perspective of economic levels, the highest LCA ASMR shifted from low-income areas in 1990 to high-income areas in 2021. Additionally, high-income areas consistently bore the highest burden of LCA-related deaths throughout 1990-2021.
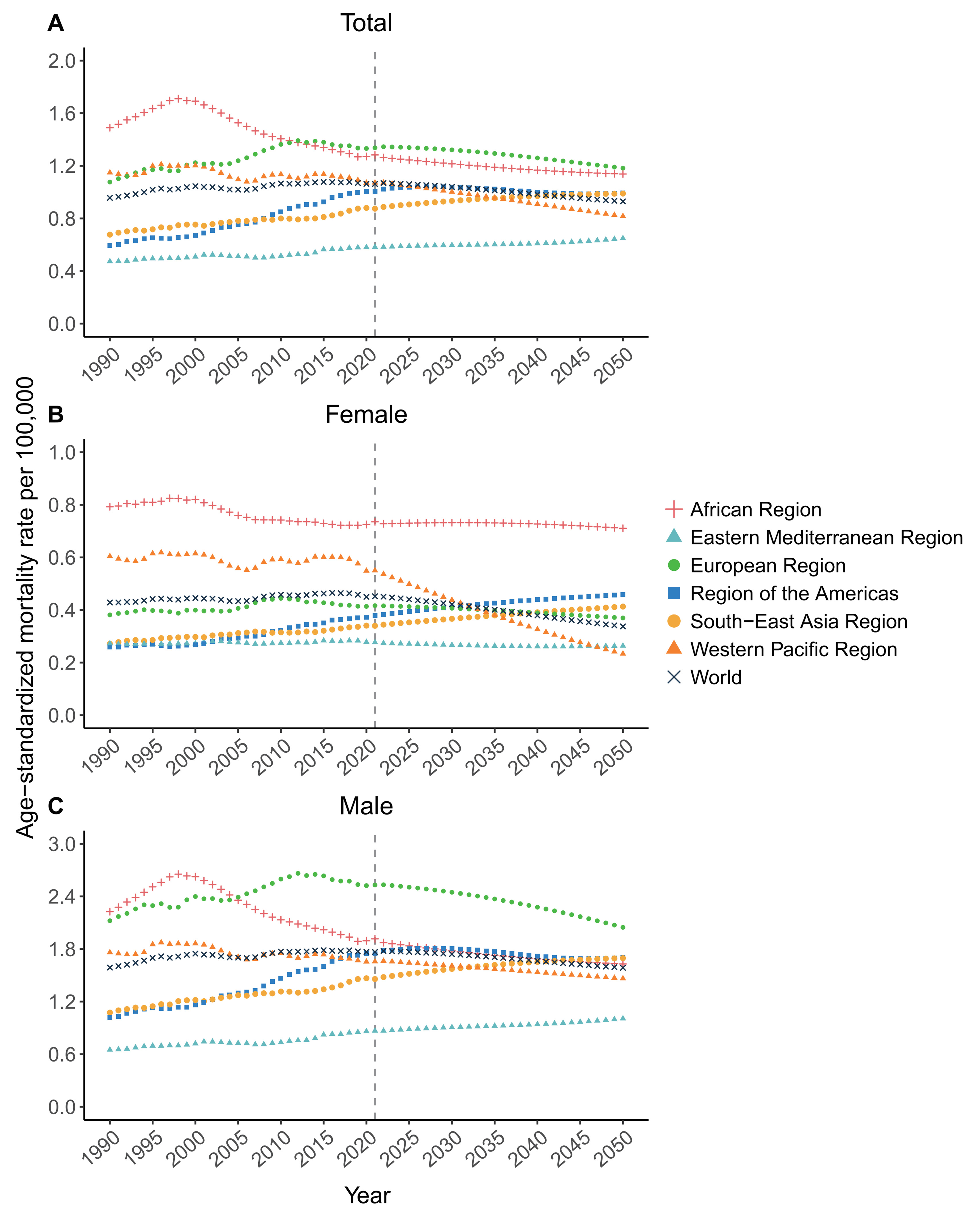
Figure 1. Temporal trends in ASMR for LCA from 1990 to 2050. (A) Total population; (B) Female; (C) Male. The dashed vertical line denotes the transition point between historical data (1990-2021) obtained from the Global Burden of Disease database, and future projections (2022-2050) estimated by the Bayesian age-period-cohort model. ASMR: Age-standardized mortality rate; LCA: liver cancer due to alcohol use.
Deaths, ASMR, change percents and AAPC for LCA during 1990 and 2021
| Category | 1990 | 2021 | 1990-2021 | ||||
| Deaths (95%UI) | ASMR (95%UI) | Deaths (95%UI) | ASMR (95%UI) | Change in deaths (95%UI) | AAPC (95%CI) | ||
| Total | |||||||
| Global | 38171 (31169-46199) | 0.96 (0.78-1.15) | 92227 (75053-112160) | 1.06 (0.86-1.29) | 141.61 (118.82-169.97) | 0.35 (0.22-0.48) | |
| WHO regions | African region | 3303 (2006-5020) | 1.49 (0.91-2.29) | 6454 (4669-8658) | 1.28 (0.95-1.71) | 95.38 (54.07-205.51) | -0.48 (-0.55 to -0.42) |
| Eastern Mediterranean region | 851 (582-1258) | 0.47 (0.32-0.70) | 2620 (1880-3600) | 0.58 (0.41-0.79) | 207.75 (116.37-299.28) | 0.67 (0.44-0.89) | |
| European region | 11764 (9867-13846) | 1.08 (0.90-1.26) | 22309 (18272-26428) | 1.34 (1.1-1.57) | 89.63 (76.49-102.51) | 0.69 (0.51-0.88) | |
| Region of the Americas | 3650 (3169-4190) | 0.59 (0.52-0.68) | 13679 (11824-15689) | 1.00 (0.87-1.15) | 274.77 (256.49-290.98) | 1.78 (1.45-2.11) | |
| South-East Asia region | 4809 (3781-6110) | 0.68 (0.54-0.86) | 15962 (13095-19969) | 0.87 (0.72-1.10) | 231.89 (178.16-287.87) | 0.82 (0.57-1.06) | |
| Western Pacific region | 13615 (10876-16790) | 1.15 (0.93-1.41) | 30767 (23786-39559) | 1.07 (0.83-1.37) | 125.99 (88.62-176.42) | -0.23 (-0.69-0.24) | |
| SDI quintile | High | 11989 (10070-14059) | 1.08 (0.91-1.27) | 28567 (23765-33858) | 1.36 (1.13-1.61) | 138.27 (119.53-154.43) | 0.74 (0.51-0.97) |
| High-middle | 9802 (8131-11665) | 0.97 (0.81-1.15) | 18544 (15108-22320) | 0.92 (0.76-1.11) | 89.18 (66.51-116.02) | -0.14 (-0.54-0.27) | |
| Middle | 9708 (7874-12146) | 0.93 (0.75-1.16) | 28334 (22395-35632) | 1.04 (0.83-1.29) | 191.86 (144.55-248.54) | 0.38 (0.12-0.63) | |
| Low-middle | 3960 (3054-5162) | 0.65 (0.50-0.85) | 11579 (9277-14972) | 0.80 (0.64-1.02) | 192.42 (146.96-246.71) | 0.69 (0.46-0.92) | |
| Low | 2664 (1729-3886) | 1.19 (0.78-1.76) | 5117 (3703-7020) | 1.02 (0.74-1.40) | 92.11 (56.47-179.58) | -0.51 (-0.66 to -0.37) | |
| Health system level | Advanced | 17499 (14789-20400) | 1.06 (0.89-1.23) | 37352 (31088-44119) | 1.31 (1.09-1.53) | 113.45 (99.80-125.93) | 0.66 (0.42-0.91) |
| Basic | 14142 (11246-17767) | 0.93 (0.75-1.17) | 36927 (28584-47214) | 0.96 (0.75-1.23) | 161.12 (117.11-216.65) | 0.10 (-0.14-0.34) | |
| Limited | 5158 (3968-6627) | 0.65 (0.50-0.85) | 15581 (12615-19463) | 0.78 (0.63-0.97) | 202.06 (152.95-268.21) | 0.61 (0.45-0.77) | |
| Minimal | 1324 (773-2059) | 2.27 (1.35-3.57) | 2281 (1512-3324) | 1.90 (1.26-2.75) | 72.27 (30.68-181.31) | -0.57 (-0.71 to -0.43) | |
| World Bank income level | High | 15081 (12711-17633) | 1.16 (0.98-1.36) | 33395 (27687-39728) | 1.42 (1.18-1.68) | 121.44 (106.00-135.47) | 0.63 (0.38-0.88) |
| Upper middle | 13455 (10834-16555) | 0.88 (0.71-1.08) | 31736 (25170-39843) | 0.89 (0.71-1.11) | 135.87 (94.96-180.83) | -0.83 (-0.89 to -0.76) | |
| Lower middle | 7598 (6028-9789) | 0.72 (0.58-0.93) | 23567 (18727-30273) | 0.93 (0.74-1.18) | 210.16 (157.34-275.60) | 0.80 (0.67-0.92) | |
| Low | 1989 (1267-3016) | 1.37 (0.87-2.10) | 3442 (2338-4907) | 1.06 (0.73-1.52) | 73.05 (37.66-162.05) | 0 (-0.29-0.30) | |
| Male | |||||||
| Global | 29020 (23918-35445) | 1.59 (1.32-1.93) | 71268 (58195-86613) | 1.77 (1.45-2.13) | 145.58 (120.16-181.45) | 0.36 (0.25-0.47) | |
| WHO regions | African region | 2423 (1414-3645) | 2.23 (1.32-3.38) | 4542 (3255-6247) | 1.92 (1.40-2.59) | 87.45 (42.91-221.97) | -0.5 (-0.55 to -0.44) |
| Eastern Mediterranean region | 625 (443-923) | 0.65 (0.46-0.97) | 2027 (1457-2855) | 0.87 (0.62-1.20) | 224.15 (124.87-316.03) | 0.91 (0.62-1.21) | |
| European region | 9244 (7770-10718) | 2.12 (1.80-2.46) | 18288 (15194-21403) | 2.53 (2.11-2.95) | 97.84 (83.04-114.00) | 0.55 (0.36-0.74) | |
| Region of the Americas | 2766 (2436-3125) | 1.02 (0.90-1.15) | 10878 (9503-12283) | 1.74 (1.52-1.97) | 293.33 (271.59-311.97) | 1.84 (1.50-2.18) | |
| South-East Asia region | 3889 (3012-4912) | 1.07 (0.84-1.35) | 12793 (10338-16520) | 1.46 (1.18-1.87) | 228.97 (172.60-292.03) | 0.98 (0.64-1.32) | |
| Western Pacific region | 9930 (7832-12547) | 1.76 (1.41-2.19) | 22392 (16812-29654) | 1.66 (1.25-2.16) | 125.49 (76.72-186.23) | -0.17 (-0.56-0.21) | |
| SDI quintile | High | 9759 (8256-11278) | 2.05 (1.74-2.37) | 23698 (20022-27753) | 2.46 (2.07-2.86) | 142.84 (123.50-160.51) | 0.59 (0.38-0.81) |
| High-middle | 7272 (6052-8686) | 1.68 (1.41-1.97) | 13850 (11139-16808) | 1.53 (1.24-1.86) | 90.45 (66.13-122.89) | -0.28 (-0.69-0.14) | |
| Middle | 6918 (5514-8956) | 1.36 (1.09-1.75) | 21260 (16440-27630) | 1.64 (1.28-2.11) | 207.29 (151.32-280.87) | 0.62 (0.34-0.90) | |
| Low-middle | 3009 (2346-4011) | 0.96 (0.75-1.26) | 8705 (6921-11459) | 1.25 (1.00-1.64) | 189.32 (143.37-249.00) | 0.86 (0.62-1.10) | |
| Low | 2026 (1301-2903) | 1.77 (1.16-2.55) | 3685 (2632-5144) | 1.49 (1.08-2.06) | 81.90 (44.57-185.31) | -0.57 (-0.74 to -0.41) | |
| Health system level | Advanced | 14018 (11886-16115) | 2.04 (1.74-2.34) | 30819 (25993-35907) | 2.42 (2.04-2.81) | 119.86 (104.66-134.04) | 0.54 (0.31-0.77) |
| Basic | 9986 (7914-13015) | 1.37 (1.09-1.76) | 27012 (20355-35741) | 1.49 (1.13-1.94) | 170.49 (117.49-236.95) | 0.24 (0.01-0.48) | |
| Limited | 3934 (3061-5072) | 0.95 (0.74-1.23) | 11633 (9390-14808) | 1.21 (0.98-1.53) | 195.69 (146.82-271.12) | 0.77 (0.56-0.98) | |
| Minimal | 1047 (598-1632) | 3.63 (2.07-5.61) | 1735 (1153-2538) | 3.07 (2.04-4.42) | 65.72 (23.07-198.30) | -0.55 (-0.70 to -0.40) | |
| World Bank income level | High | 12291 (10457-14177) | 2.21 (1.89-2.54) | 27828 (23513-32673) | 2.59 (2.18-3.03) | 126.41 (109.58-141.92) | 0.50 (0.26-0.75) |
| Upper middle | 9235 (7384-11759) | 1.31 (1.05-1.64) | 22518 (17398-28836) | 1.36 (1.05-1.73) | 143.83 (94.05-205.14) | -0.88 (-0.94 to -0.82) | |
| Lower middle | 5940 (4697-7735) | 1.14 (0.91-1.48) | 18330 (14311-24338) | 1.49 (1.18-1.94) | 208.61 (156.71-282.25) | 0.89 (0.75-1.04) | |
| Low | 1519 (941-2305) | 2.16 (1.33-3.28) | 2522 (1708-3666) | 1.65 (1.13-2.35) | 66.09 (28.31-176.61) | 0.08 (-0.24-0.40) | |
| Female | |||||||
| Global | 9151 (7228-11508) | 0.43 (0.34-0.54) | 20960 (16643-25768) | 0.45 (0.36-0.56) | 129.04 (98.63-165.84) | 0.17 (-0.08-0.41) | |
| WHO regions | African region | 880 (530-1447) | 0.79 (0.48-1.32) | 1912 (1394-2556) | 0.74 (0.53-0.97) | 117.21 (51.79-204.96) | -0.24 (-0.36 to -0.13) |
| Eastern Mediterranean region | 226 (144-374) | 0.27 (0.17-0.46) | 593 (417-823) | 0.28 (0.20-0.38) | 162.40 (71.56-289.76) | 0.06 (-0.09-0.21) | |
| European region | 2521 (1953-3189) | 0.38 (0.30-0.48) | 4022 (3087-5127) | 0.42 (0.32-0.52) | 59.55 (48.70-70.88) | 0.28 (0-0.56) | |
| Region of the Americas | 884 (732-1075) | 0.26 (0.21-0.31) | 2801 (2300-3422) | 0.38 (0.31-0.46) | 216.74 (197.94-234.03) | 1.25 (0.90-1.60) | |
| South-East Asia region | 921 (702-1160) | 0.27 (0.21-0.34) | 3169 (2493-4011) | 0.34 (0.27-0.43) | 244.21 (181.85-311.35) | 0.74 (0.46-1.02) | |
| Western Pacific region | 3684 (2861-4618) | 0.60 (0.47-0.76) | 8375 (6380-10631) | 0.55 (0.42-0.70) | 127.32 (79.96-194.56) | -0.27 (-0.85-0.32) | |
| SDI quintile | High | 2231 (1765-2807) | 0.34 (0.27-0.42) | 4869 (3769-6133) | 0.41 (0.33-0.52) | 118.30 (98.38-135.35) | 0.59 (0.27-0.91) |
| High-middle | 2530 (2042-3123) | 0.45 (0.36-0.55) | 4693 (3651-5882) | 0.42 (0.33-0.53) | 85.51 (55.00-125.57) | -0.17 (-0.58-0.23) | |
| Middle | 2790 (2197-3450) | 0.53 (0.42-0.65) | 7074 (5491-8692) | 0.50 (0.39-0.61) | 153.58 (103.56-221.71) | -0.16 (-0.44-0.12) | |
| Low-middle | 951 (678-1337) | 0.32 (0.23-0.46) | 2874 (2253-3604) | 0.39 (0.30-0.48) | 202.20 (130.12-277.20) | 0.58 (0.37-0.79) | |
| Low | 638 (396-1024) | 0.59 (0.37-0.97) | 1432 (994-1974) | 0.57 (0.40-0.79) | 124.53 (72.53-196.76) | -0.12 (-0.20 to -0.03) | |
| Health system level | Advanced | 3482 (2783-4329) | 0.35 (0.28-0.44) | 6533 (5087-8137) | 0.40 (0.31-0.49) | 87.64 (72.15-101.01) | 0.38 (0.07-0.68) |
| Basic | 4156 (3229-5228) | 0.54 (0.42-0.68) | 9915 (7676-12379) | 0.50 (0.38-0.62) | 138.58 (87.76-208.81) | -0.26 (-0.57-0.06) | |
| Limited | 1224 (860-1700) | 0.33 (0.23-0.46) | 3948 (3112-4835) | 0.39 (0.31-0.48) | 222.51 (148.01-299.85) | 0.57 (0.40-0.75) | |
| Minimal | 277 (151-487) | 0.95 (0.52-1.74) | 546 (336-864) | 0.89 (0.54-1.38) | 96.97 (44.55-181.43) | -0.23 (-0.33 to -0.14) | |
| World Bank income level | High | 2790 (2213-3518) | 0.37 (0.29-0.45) | 5568 (4281-7002) | 0.42 (0.33-0.52) | 99.55 (82.49-114.58) | 0.40 (0.15-0.66) |
| Upper middle | 4220 (3309-5234) | 0.52 (0.41-0.64) | 9218 (7128-11467) | 0.48 (0.37-0.60) | 118.44 (75.20-180.40) | -0.47 (-0.58 to -0.36) | |
| Lower middle | 1659 (1217-2224) | 0.32 (0.24-0.44) | 5237 (4101-6613) | 0.40 (0.32-0.51) | 215.72 (137.11-289.44) | 0.72 (0.56-0.88) | |
| Low | 470 (282-777) | 0.64 (0.38-1.07) | 919 (604-1339) | 0.55 (0.36-0.81) | 95.55 (50.02-161.31) | -0.27 (-0.62-0.09) | |
Future forecasts of ASMR for LCA during 2022-2050 by sex and region
The predictive analysis showed that the global ASMR of LCA will shift from a historical fluctuating upward trend to a gradual downward trend after 2022, without considering future changes in alcohol exposure or the implementation of new relevant policies. The global ASMR is projected to drop to 0.93 per 100,000 population by 2050, representing a 12.26% reduction from the 2021 baseline of 1.06 per 100,000 population [Supplementary Table 1]. From 2022 to 2050, European males and African females are predicted to sustain the highest sex-specific ASMRs worldwide [Figure 1]. Unlike most WHO regions that will follow the global declining trend, the Southeast Asia region (AAPC = 0.39, 95%CI: 0.38-0.40) and the Eastern Mediterranean region (AAPC = 0.38, 95%CI: 0.36-0.40) are projected to maintain continuous increases in ASMR [Supplementary Table 1]. Regionally, males will consistently exhibit substantially higher ASMRs than females across all WHO regions until 2050. Long-term forecasting ASMRs showed that the 95% uncertainty intervals (UIs) for males and females will gradually widen and partially overlap, attributable to the cumulative inherent uncertainty of predictive models. Nevertheless, a persistent absolute difference remains between the projected mean ASMRs of males and females.
The AAPC and spatiotemporal patterns of ASMR for LCA in 204 countries and territories, 1990-2021 and 2022-2050
LCA ASMR exhibited substantial geographical heterogeneity across 204 countries and territories worldwide. Spatiotemporal model analysis revealed that the structured spatial variation (Mean ± SD = 4.22 ± 0.81) was markedly higher than the unstructured variation (Mean ± SD = 0.41 ± 0.19). This finding indicates a prominent spatial clustering of LCA mortality, with spatial dependence among adjacent regions serving as the primary contributor to cross-country and cross-territory disparities in LCA ASMR [Supplementary Table 3]. Significant high-mortality clustering of LCA ASMR was concentrated in West Africa, Southern Africa, and partial regions of Southeast Asia [Figure 2A]. The baseline ASMR for the period 1990-2021 was 1.50 (95%CI: 1.38-1.61). Temporal effect analysis demonstrated that LCA ASMR fluctuated minimally around this baseline (± 0.03) throughout the study period, with a relatively high mortality level observed around 1997 [Figure 2B and Supplementary Table 3]. Although the spatiotemporal interaction coefficient was numerically small, it reached statistical significance with its 95% confidence interval excluding zero. The United States, China, India, Brazil, and Indonesia presented consistent spatiotemporal specificity in LCA mortality trends. Specifically, their national ASMRs remained below the overall baseline in the early stage of the study period and gradually rose to and exceeded the baseline level between 2005 and 2010 [Figure 2C]. Among these five countries, the United States experienced the most severe deterioration in LCA mortality status. For the projected period of 2022-2050, the overall baseline ASMR across the 204 countries and territories is estimated to be 1.46 (95%CI: 1.22-1.69). Forecast results indicate weakened spatial similarity and dependence in LCA ASMR among neighboring regions, accompanied by increased spatial random variation in mortality distribution [Supplementary Table 3 and Figure 3]. The ASMR of LCA is predicted to decrease the fastest in Singapore (AAPC = -6.44, 95%CI: -6.47 to -6.40), whereas it is predicted to increase the fastest in Venezuela (AAPC = 7.34, 95%CI: 7.30-7.37). The top three countries with the highest ASMR in 2021 were Mongolia, Gambia, and Mozambique [Figure 4A and Supplementary Table 2]. By 2050, Mongolia, The Gambia, and Venezuela are predicted to become the top three countries with the highest ASMRs [Figure 4B and Supplementary Table 2]. For the historical period of 1990-2021, Mauritius had the most remarkable decline in LCA ASMR, whereas Poland exhibited the fastest growth (AAPC = 4.30, 95%CI: 3.30-5.31, Figure 4C).
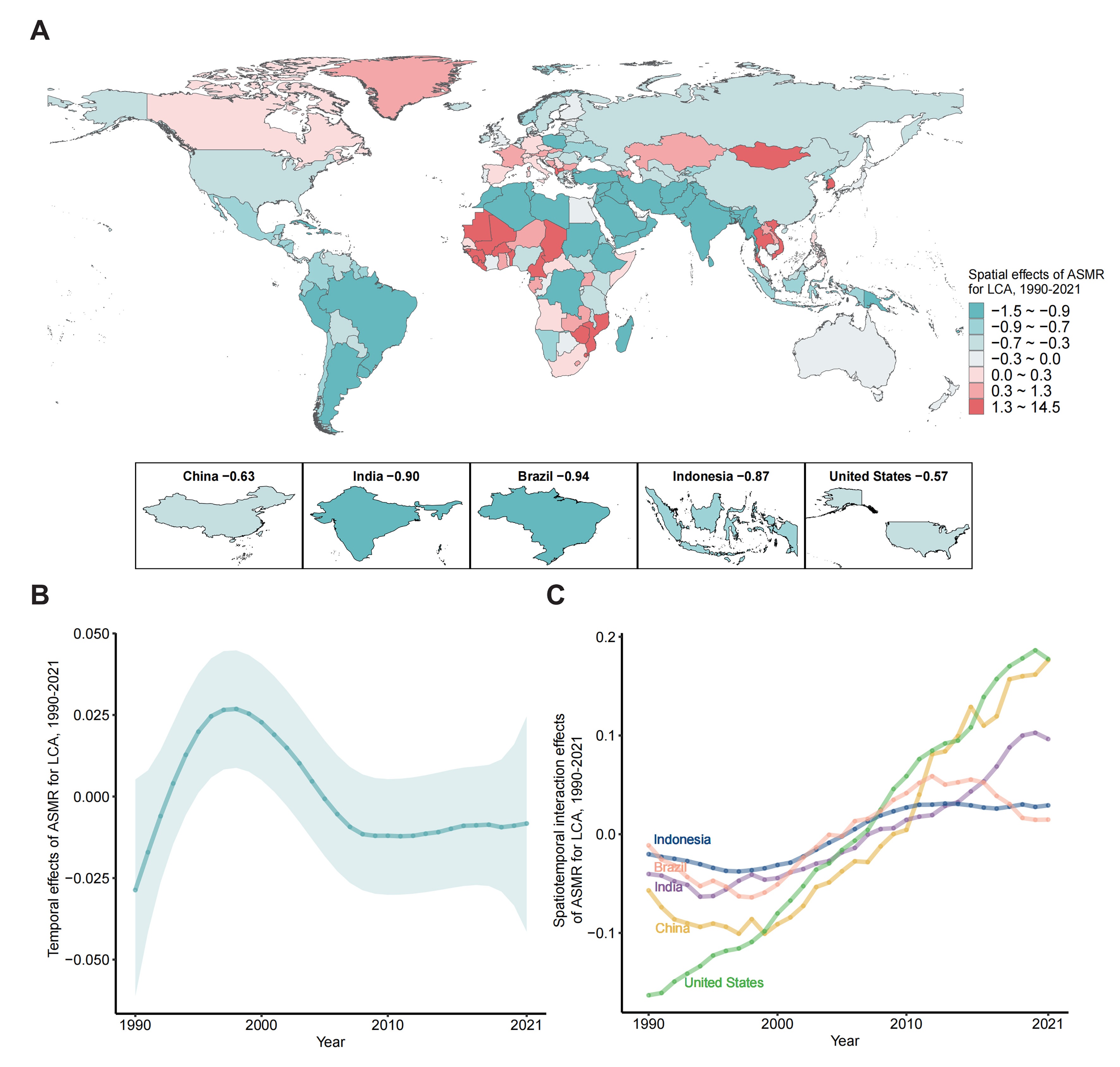
Figure 2. Bayesian spatial temporal distribution of ASMR for LCA in 204 countries and territories, 1990-2021. (A) Spatial effects of 204 countries and territories; (B) The overall temporal effects, with the 95% credible interval shown as a shaded region; (C) Spatiotemporal interaction effects of top five countries by population (including China, India, the United States, Indonesia, and Brazil). ASMR: Age-standardized mortality rate; LCA: liver cancer due to alcohol use.
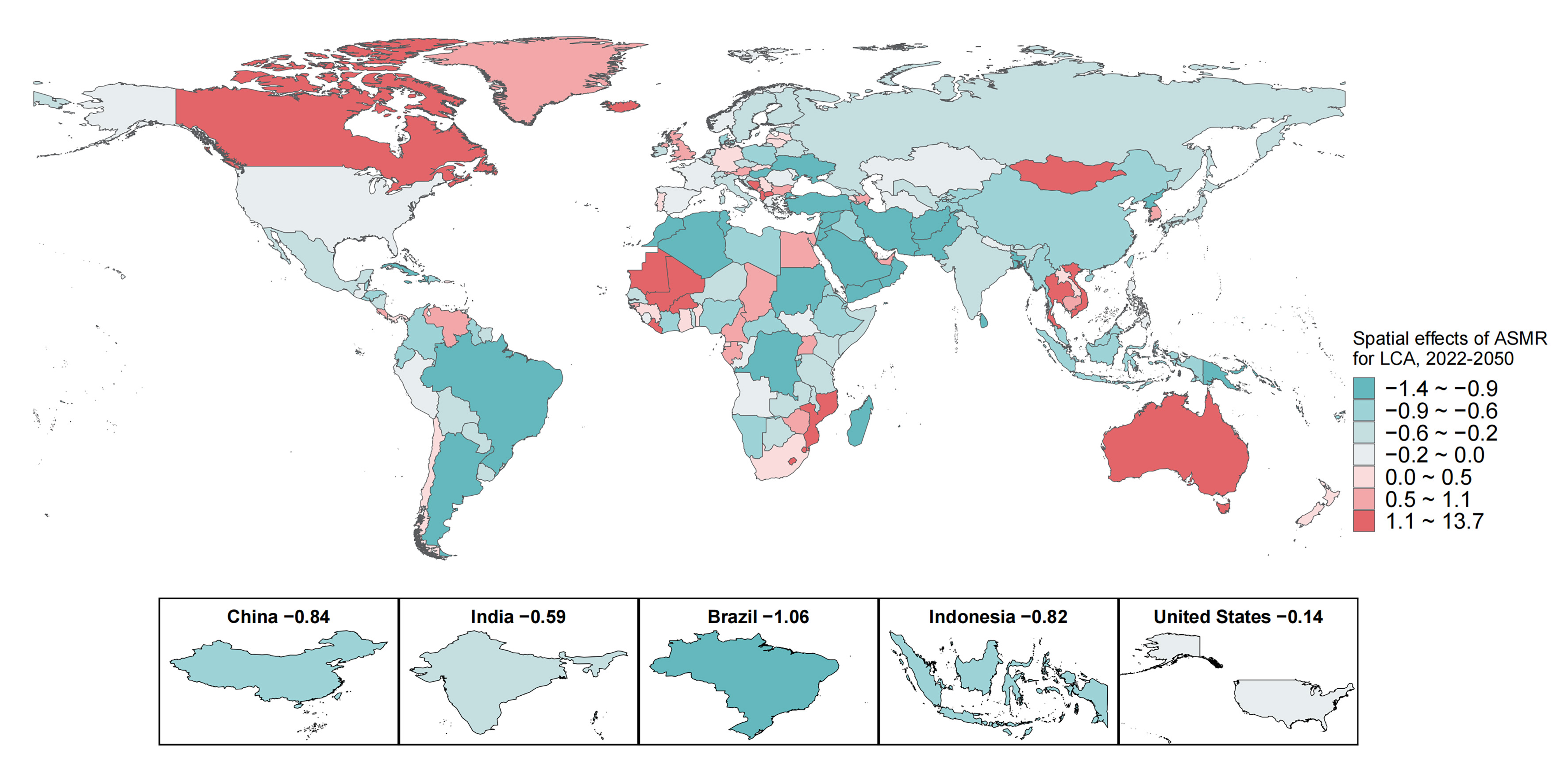
Figure 3. Bayesian spatial effects of ASMR for LCA in 204 countries and territories, 2022-2050. ASMR: Age-standardized mortality rate; LCA: liver cancer due to alcohol use.

Figure 4. The ASMR and AAPC of LCA in 204 countries and territories. (A) Historical ASMR in 2021 (per 100,000); (B) Projected ASMR in 2050 (per 100,000); (C) AAPC of ASMR during the historical period from 1990 to 2021. ASMR: Age-standardized mortality rate; LCA: liver cancer due to alcohol use; AAPC: average annual percent change.
Frontier prediction of ASMR for LCA with different SDI countries and territories in 2050
Figure 5 illustrates the predicted improvement potential of LCA ASMR across countries and territories with different socioeconomic development levels. The effective difference in ASMR increased alongside rising SDI, suggesting that countries with higher socioeconomic development possess greater potential for ameliorating LCA-related health burdens. Frontier analysis further indicated that higher-SDI countries could attain lower LCA ASMR by 2050 through full utilization of existing health and socioeconomic resources. Globally, the top ten countries with substantial effective differences were predominantly classified as medium-to-high SDI regions. Among the five most populous countries, Indonesia, India, China, and the United States exhibited varying degrees of potential for ASMR reduction, while Brazil is expected to reach its achievable minimum. Additionally, several countries, including Somalia, Haiti, Hungary, and Niger, showed zero effective differences in ASMR projections. This finding suggests that their predicted 2050 ASMRs will approach the optimal achievable limit under current conditions, indicating highly efficient national health resource utilization in these regions [Supplementary Table 4].
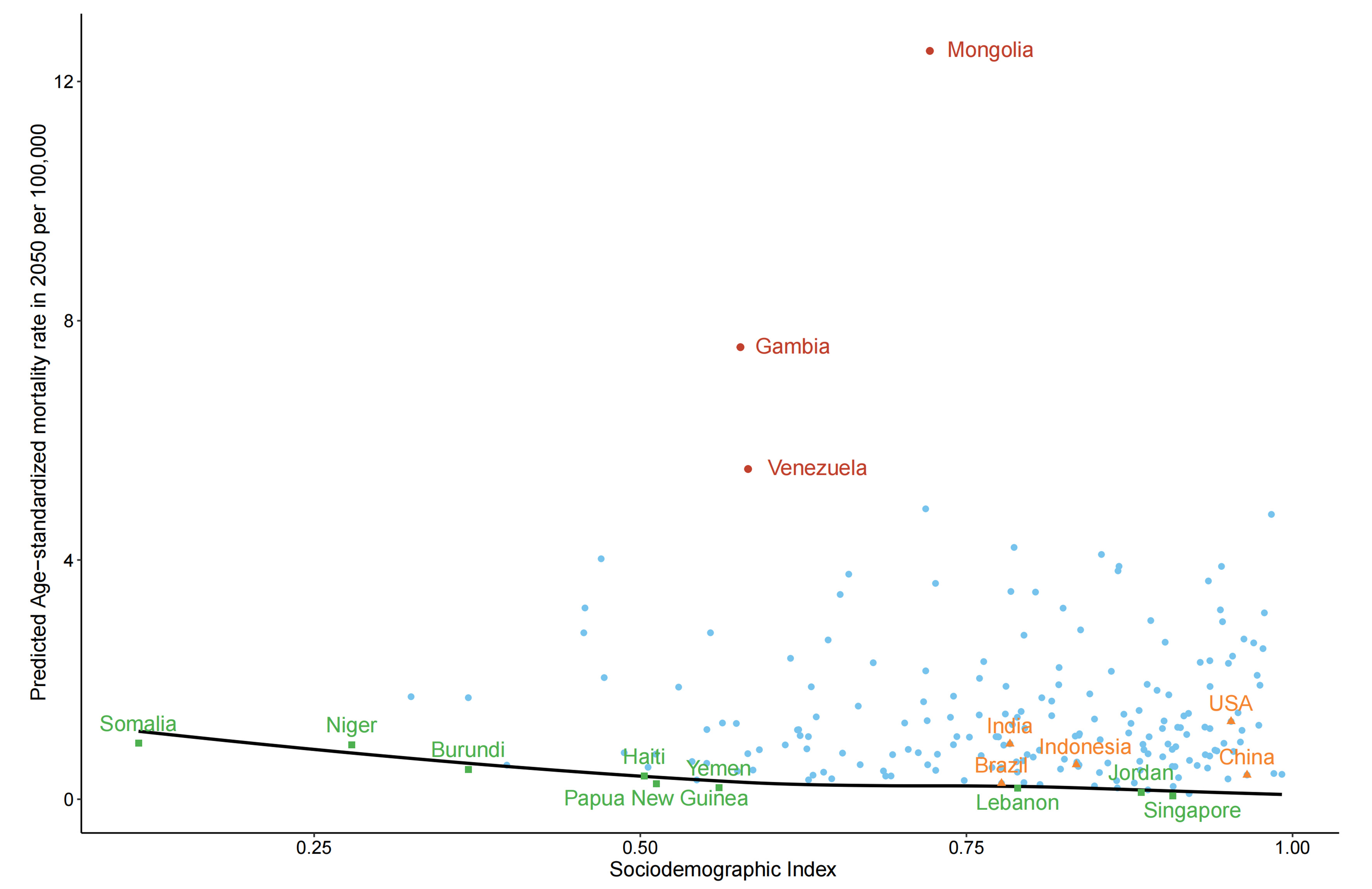
Figure 5. Frontier analysis results based on the sociodemographic index and predicted ASMR for LCA in 2050. The black line represents the frontier (i.e., the optimal ASMR achievable at each SDI level). Green dots represent countries and territories with the lowest predicted ASMR. Red dots highlight the top ten countries with the greatest effective differences from the frontier. Orange dots represent the top five countries by population including China, India, the United States, Indonesia, and Brazil. Light blue dots represent all other countries and territories. The smaller the vertical distance between the point and the curve, the smaller the gap between the predicted ASMR value of the corresponding country and the lowest achievable ASMR value, that is, the more efficient the use of national resources for disease prevention and control. ASMR: Age-standardized mortality rate; LCA: liver cancer due to alcohol use; SDI: sociodemographic index.
Impact contribution of population growth, age structure and epidemiological changes on LCA deaths
Decomposition analysis demonstrated that population growth and age structure were the predominant drivers of increased global LCA deaths between 1990 and 2021. From 2022 to 2050, the age structure will become the key point for the increase in LCA deaths except for the African region [Figure 6]. In Africa, population growth remains the dominant factor accounting for temporal variations in LCA mortality across the entire study and forecast period. For the Western Pacific and European regions, age structure transitions constitute the primary determinant of LCA death trends throughout 1990-2050 [Supplementary Table 5]. Notably, epidemiological changes are expected to exert a beneficial effect, contributing to the global reduction in LCA mortality during the 2022-2050 projection period.
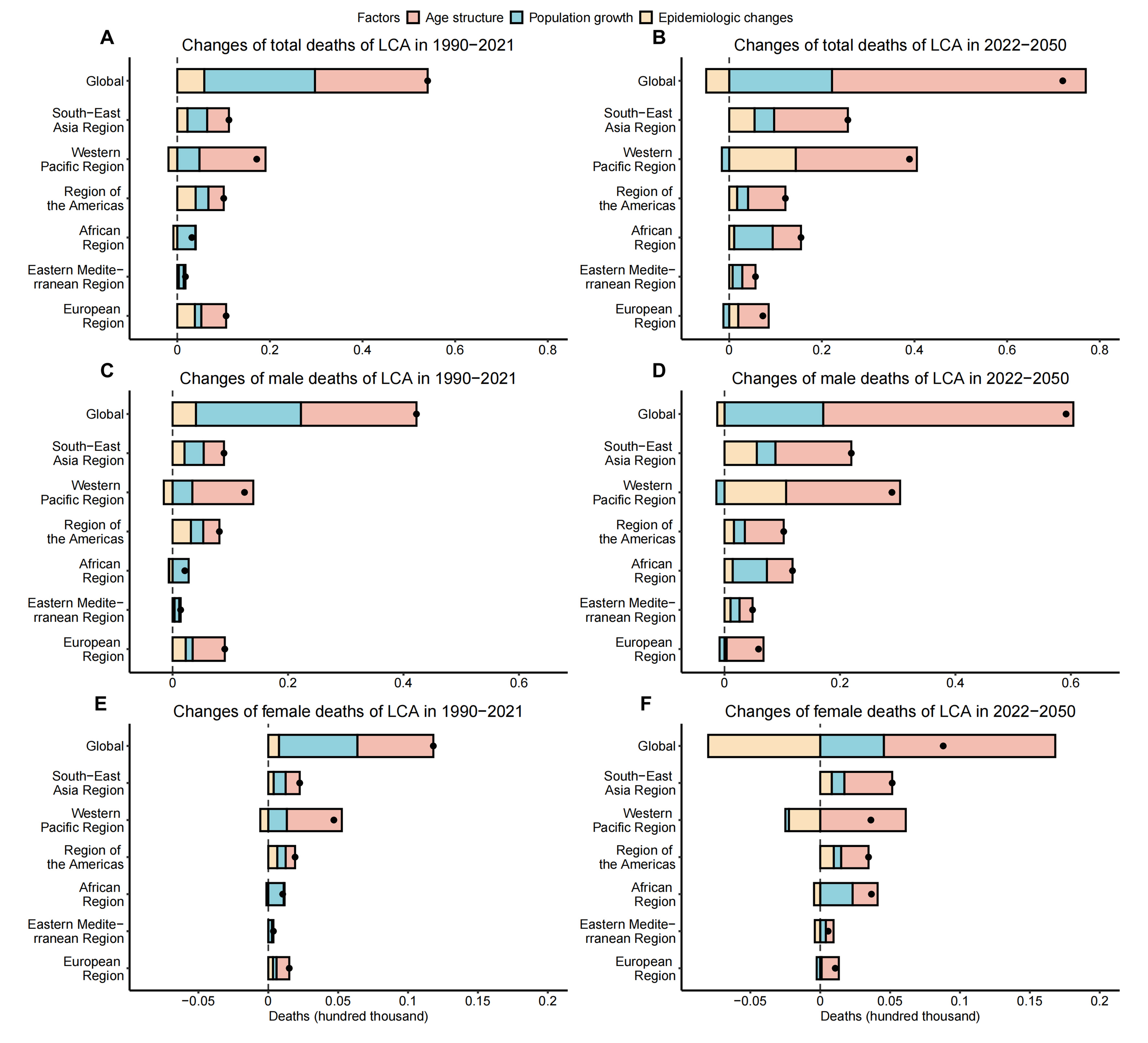
Figure 6. Contributions of population growth, age structure, epidemiological changes to the increase in deaths from LCA, 1990-2021, 2022-2050. (A) Decomposition analysis for both genders, 1990-2021; (B) Decomposition analysis for both genders, 2022-2050; (C) Decomposition analysis for males, 1990-2021; (D) Decomposition analysis for males, 2022-2050; (E) Decomposition analysis for females, 1990-2021; (F) Decomposition analysis for females, 2022-2050. Black dots represent the net change of deaths during each time period. The magnitude of a positive value indicates a corresponding increase in deaths attributed to the factor, and the magnitude of a negative value indicates a corresponding decrease in deaths attributed to the related factor. LCA: Liver cancer due to alcohol use.
DISCUSSION
This study comprehensively analyzed the global, regional and national mortality burden of LCA from 1990 to 2021 and further predicted its epidemiological trends through 2050. Globally, LCA ASMR exhibited an upward trend during 1990-2021, with the most rapid increase observed in the Americas and the highest mortality level recorded in Europe in 2021. The high SDI quintile and high-income areas consistently bore the greatest number of deaths. Population growth and age structure were the main contributors to rising global LCA deaths, and population aging is projected to remain a dominant contributing factor through 2050. Substantial global heterogeneity in LCA mortality was identified across different populations, income strata, healthcare capacities, and socioeconomic conditions. These findings demonstrate the evolving epidemiological profile of LCA within the overall liver cancer mortality burden and underline the necessity of targeted and tailored public health intervention strategies.
The pronounced temporal and spatial disparities in LCA ASMR identified in this study highlight the urgent demand for standardized and systematic frameworks for LCA prevention, early diagnosis, population assessment, and clinical treatment. Overall, the global LCA mortality burden gradually increased during 1990-2021 but is projected to plateau and slowly decline in the future. The Americas showed the most rapid growth in ASMR, and Europe held the highest ASMR in 2021, which were consistent with the distribution of alcohol consumption[12]. In contrast, the Eastern Mediterranean region presented the lowest LCA ASMR, which corresponded to local reductions in alcohol intake. Regional alcohol consumption patterns have diverged substantially: per-adult alcohol consumption has risen sharply across Asia and Africa, while declining in North America, South America, and Europe[13]. Although improved public health awareness and reduced alcohol exposure have contributed to LCA mortality declines in several regions, low-income settings and populations with insufficient access to healthcare continue to endure a disproportionately heavy LCA mortality burden. Notably, African females sustained the highest LCA ASMR over the study period. This observation is consistent with prior evidence documenting prominent socioeconomic inequities in the prevalence and prognostic outcomes of alcohol-related liver disease[14]. Further in-depth research focusing on epigenetic mechanisms, individual disease susceptibility, and gender-specific biological and social determinants is warranted to elucidate the distinct gender disparities in LCA epidemiology.
The geographical distribution of the highest LCA ASMR has gradually transitioned from low-income to high-income regions over the past three decades, whereas high-income settings have persistently exhibited the greatest absolute number of LCA-related deaths. A similar epidemiological shift was also observed across SDI stratifications. Population aging represents a critical risk factor for liver cancer, and the more severe aging burden in high-income regions substantially elevates LCA mortality risk[15]. In addition, alcohol consumption constitutes another predominant modifiable driver of LCA epidemiology, with higher per capita alcohol intake commonly documented in high-income populations. Alcohol use disorder (AUD) can cause a series of physical damages. However, the main cause of alcohol-related deaths is alcohol-associated liver disease (ALD). In some countries, the mortality rate due to alcohol-related causes caused by ALD is almost 90%[13]. Furthermore, the contribution of alcohol to the LC burden continues to rise, especially in high-income countries[16]. These synergistic drivers underscore a transitioning epidemiologic landscape for LCA. Continued trends may escalate ASMRs in high-income areas without coordinated prevention strategies.
Viral hepatitis (HBV and HCV) has historically been the predominant etiology of hepatocellular carcinoma (HCC). With widespread HBV vaccination and the availability of potent direct-acting antivirals (DAAs) for HCV, the viral contribution to liver cancer is gradually declining, leading to a more complex, multifactorial epidemiological landscape. Accumulating evidence indicates that alcohol consumption and metabolic dysfunction-associated steatotic liver disease (MASLD) have become the fastest-growing risk factors for liver cancer worldwide[2]. These etiological factors often exert synergistic rather than independent effects, such that alcohol exposure further elevates liver cancer risk in individuals with pre-existing metabolic or viral liver diseases. Recent clinical data have further demonstrated the evolving epidemiology and prognostic profiles of LCA[17,18]. Registry-based evidence from Florida has documented a continuous rise in LCA incidence, with an annual percentage increase of 6.0% between 2010 and 2018, disproportionately affecting ethnic minorities, particularly Puerto Rican and Mexican subgroups[19]. Alcohol-attributable mortality has also risen sharply, with a notable surge during the COVID-19 pandemic[20,21]. Correspondingly, LCA has become a leading indication for liver transplantation, accounting for 41% of all liver transplantations in 2022[22,23]. In patients with mild-to-moderate AUD without critical complications, substantial alcohol reduction can yield clinical benefits, whereas strict abstinence markedly improves survival in patients with alcohol-related cirrhosis[5]. Integrated therapeutic strategies combining liver disease management and addiction treatment have also achieved favorable outcomes in patients with advanced ALD[24].
Despite ongoing advances in the understanding and management of LCA, substantial regional disparities in disease burden persist. Low-income countries and populations with restricted healthcare access continue to bear a disproportionate LCA mortality burden, particularly African females, who consistently exhibit the highest LCA ASMR. Therefore, intervention measures must combine clinical progress with socio-economic factors. In regions with lower income levels, healthcare access remains a critical factor shaping LCA burden. In the United States, ethnic disparities and income inequality and lower socioeconomic status are correlated with increased LC mortality, particularly in areas with high unemployment or housing issues[25]. In China, geographical disparities in liver cancer mortality are driven by poverty, limited healthcare access, and environmental pollution; industrial areas suffer higher mortality due to excessive alcohol consumption and substandard healthcare infrastructure[26]. Notably, significant LCA mortality differences also exist between geographically and demographically similar neighboring countries. In East Asia, for example, Mongolia and South Korea have disproportionately high LCA ASMR. In 2022, South Korea recorded a per capita alcohol consumption of 8.4 liters, exceeding 6.3 liters in Japan and 4.8 liters in North Korea[27]. South Korea also has a markedly higher prevalence of heavy drinking, driven by high spirits (particularly soju) consumption, which is closely associated with socioeconomic stress and prevalent workplace drinking norms[28,29]. Cross-national disparities in LCA burden are collectively attributed to variations in healthcare system capacity, obesity and metabolic syndrome prevalence, alcohol consumption patterns, and public health policies. Mitigating global LCA-related health inequities requires addressing fundamental income inequality, expanding healthcare access for vulnerable populations, and reforming high-risk drinking cultures and social norms.
Frontier analysis revealed substantial cross-national disparities in the efficiency of LCA mortality control. While countries such as Brazil have attained near-optimal ASMR reductions via effective public health interventions, many low- and middle-income regions continue to face a heavy LCA mortality burden[30]. LCA mortality is largely preventable through population-level policy restrictions on alcohol accessibility. Although lifelong alcohol abstinence is critical for improving long-term clinical outcomes, sustained abstinence remains challenging for ALD patients with comorbid AUD. This underscores the necessity of a full-cycle, multidisciplinary management model involving hepatologists, addiction specialists, and social workers to optimize patient care[5].
Our findings provide a roadmap for region-specific public health interventions. Given the rapidly rising in LCA burden in the Americas, local governments should prioritize WHO-recommended “Best Buys” interventions, including higher alcohol excise taxes and stricter regulation of alcohol marketing. Furthermore, considering that population aging will remain the dominant driver of LCA mortality through 2050, public health strategies should shift from universal health education to precise targeted surveillance. Regular liver ultrasound and alpha-fetoprotein (AFP) screening are strongly recommended for elderly populations with a long-term drinking history as part of routine physical examinations. For African regions with persistent high LCA burden despite declining mortality trends, policy efforts should focus on strengthening primary healthcare infrastructure to facilitate community-based early diagnosis and standardized AUD management.
This study had several limitations that should be acknowledged. First, all analyses were based on GBD modeled estimates, and the adopted predictive framework formed a “model-on-model” approach that accumulates inherent modeling uncertainties. Results for low-data regions, including most African, Asian, and South American countries as well as small island nations, were largely extrapolated rather than derived from primary surveillance data, which may overestimate precision and requires cautious interpretation. Additionally, GBD data may underestimate the true LCA burden in low-resource settings with incomplete vital registration and weak healthcare systems. Treating large countries such as China as single analytical units also masks substantial subnational heterogeneity in alcohol exposure and healthcare accessibility, highlighting the need for future subnational-level studies. Although the Bayesian spatiotemporal and decomposition models used in this study can generate robust population-level projections, long-term forecasting inevitably involves uncertainties. Our 2022-2050 projections were based on demographic inertia and assumed sustained current trends, without accounting for future changes in alcohol-related behaviors, public health policies, and other potential confounding factors that may alter LCA mortality trajectories. Furthermore, the findings lack direct validation against real-world epidemiological data. GBD modeling produces smoothed global epidemiological patterns that may reflect preset modeling assumptions rather than actual localized heterogeneity. Integrating granular registry-based data and conducting regional and local analyses in future research can further improve the accuracy and generalizability of burden estimates. Finally, this study could not distinguish overlapping disease etiologies due to GBD data limitations. The coexistence of multiple risk factors, such as concurrent viral hepatitis infection and hazardous alcohol consumption, could not be quantified separately, which may obscure the independent and interactive effects of different pathogenic drivers.
In conclusion, this study comprehensively analyzed the global, regional and national mortality burden of LCA, systematically revealing temporal and spatial trends and regional imbalances. Global LCA ASMR exhibited a sustained increasing trend from 1990 to 2021 and is projected to gradually stabilize and decline in the future. Targeted public health interventions, including standardized alcohol control strategies and optimized liver disease surveillance systems, are urgently needed to mitigate the rising LCA burden, particularly in high-risk regions such as Africa and the Americas.
DECLARATIONS
Acknowledgments
We thank all members of our study team for their cooperation and the Global Burden of Disease Study collaborators for their work.
Authors’ contributions
Conceptualization: Deng Y, Zu J, Wang Y, Ji F
Data curation: Tan J, Xing Z, Deng Y
Formal analysis: Tan J, Xing Z, Deng Y
Funding acquisition: Deng Y, Zu J
Investigation: Yuan X, Fei Q, Qu D, Zhang C, Bo Y, Yang Z (Zhiluo Yang), He X, Han M
Methodology: Tan J, Xing Z, Yang Z (Zhanpeng Yang), Zhang Y
Project administration: Zu J, Deng Y, Wang Y
Resources: Deng Y, Wang Y, Zu J
Software: Tan J, Xing Z, Yang Z (Zhanpeng Yang), Zhang Y
Supervision: Zu J, Deng Y, Wang Y
Validation: Tan J, Xing Z, Yang Z (Zhanpeng Yang)
Visualization: Tan J, Xing Z, Yang Z (Zhanpeng Yang)
Writing - original draft: Tan J, Xing Z
Writing - review and editing: Zu J, Wang Y, Deng Y, Ji F
Had unrestricted access to all data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis: Deng Y, Zu J, Wang Y
All authors reviewed the manuscript.
Availability of data and materials
All data generated or analyzed during this study are included in this published article and its Supplementary Materials.
AI and AI-assisted tools statement
Not applicable.
Financial support and sponsorship
This work was supported by the National Natural Science Foundation of China (grant numbers 12471470, 82403188).
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
Supplementary Materials
REFERENCES
1. Oh JH, Jun DW. The latest global burden of liver cancer: a past and present threat. Clin Mol Hepatol. 2023;29:355-7.
2. Huang DQ, Singal AG, Kono Y, Tan DJH, El-Serag HB, Loomba R. Changing global epidemiology of liver cancer from 2010 to 2019: NASH is the fastest growing cause of liver cancer. Cell Metab. 2022;34:969-77.e2.
3. Diaz LA, Winder GS, Leggio L, Bajaj JS, Bataller R, Arab JP. New insights into the molecular basis of alcohol abstinence and relapse in alcohol-associated liver disease. Hepatology. 2025;82:254-71.
4. Ding C, Ng Fat L, Britton A, et al. Binge-pattern alcohol consumption and genetic risk as determinants of alcohol-related liver disease. Nat Commun. 2023;14:8041.
5. Jophlin LL, Singal AK, Bataller R, et al. ACG clinical guideline: alcohol-associated liver disease. Am J Gastroenterol. 2024;119:30-54.
6. Yu S, Wang S, Li J, et al. Detection of metabolic signatures implicated in the progression from hepatitis to cirrhosis to hepatocellular carcinoma. ILIVER. 2024;4:100142.
7. Ouyang W, Wang MD, Guan MC, et al. Diagnostic performance comparisons of two commonly used multi-biomarker-based scores for detection of hepatocellular carcinoma in non-alcoholic fatty liver disease. ILIVER. 2024;3:100098.
8. Fu Y, Maccioni L, Wang XW, Greten TF, Gao B. Alcohol-associated liver cancer. Hepatology. 2024;80:1462-79.
9. Singal AK, Mathurin P. Diagnosis and treatment of alcohol-associated liver disease: a review. JAMA. 2021;326:165-76.
10. Choi S, Kim BK, Yon DK, et al. Global burden of primary liver cancer and its association with underlying aetiologies, sociodemographic status, and sex differences from 1990-2019: a DALY-based analysis of the Global Burden of Disease 2019 study. Clin Mol Hepatol. 2023;29:433-52.
11. Deng Y, Tan J, Zu J, et al. Trends and health inequalities of hepatitis virus-associated liver cancer mortality during 1990-2050. Ann Hepatol. 2026;31:102144.
12. Global status report on alcohol and health and treatment of substance use disorders. Geneva: World Health Organization. 2024. Available from: https://www.who.int/publications/i/item/9789240096745. [Last accessed on 17 Jun 2026].
14. Niu X, Zhu L, Xu Y, et al. Global prevalence, incidence, and outcomes of alcohol related liver diseases: a systematic review and meta-analysis. BMC Public Health. 2023;23:859.
15. Li Q, Ding C, Cao M, et al. Global epidemiology of liver cancer 2022: an emphasis on geographic disparities. Chin Med J. 2024;137:2334-42.
16. Hernández-Évole H, Jiménez-Esquivel N, Pose E, Bataller R. Alcohol-associated liver disease: epidemiology and management. Ann Hepatol. 2024;29:101162.
18. Su H, Wei Y, Liao X, et al. Interpretation of the updates of the chinese guidelines for the diagnosis and treatment of primary liver cancer (CNLC-2024 Edition). Hepatoma Res. 2024;10:30.
19. Pinheiro PS, Jones PD, Medina H, et al. Incidence of etiology-specific hepatocellular carcinoma: diverging trends and significant heterogeneity by race and ethnicity. Clin Gastroenterol Hepatol. 2024;22:562-71.e8.
20. Kim D, Alshuwaykh O, Dennis BB, Cholankeril G, Ahmed A. Trends in etiology-based mortality from chronic liver disease before and during COVID-19 pandemic in the United States. Clin Gastroenterol Hepatol. 2022;20:2307-16.e3.
21. Deutsch-Link S, Jiang Y, Peery AF, Barritt AS, Bataller R, Moon AM. Alcohol-associated liver disease mortality increased from 2017 to 2020 and accelerated during the COVID-19 pandemic. Clin Gastroenterol Hepatol. 2022;20:2142-4.e2.
22. Kasiske BL, Lentine KL, Ahn Y, et al. OPTN/SRTR 2020 annual data report: living donor collective. Am J Transplant. 2022;22:553-86.
23. Younossi ZM, Stepanova M, Al Shabeeb R, et al. The changing epidemiology of adult liver transplantation in the United States in 2013-2022: the dominance of metabolic dysfunction-associated steatotic liver disease and alcohol-associated liver disease. Hepatol Commun. 2024;8:e0352.
24. Arab JP, Addolorato G, Mathurin P, Thursz MR. Alcohol-associated liver disease: integrated management with alcohol use disorder. Clin Gastroenterol Hepatol. 2023;21:2124-34.
25. Rezaee-Zavareh MS, Liang J, Yang JD. Ethnic disparities in the epidemiology, treatment, and outcome of patients with hepatocellular carcinoma in the United States. Hepatoma Res. 2023;9:18.
26. Shen X, Wang L, Zhang X, Liu J, Wang L, Zhu L. Analysis of forty years of geographic disparity in liver cancer mortality and the influence of risk factors. Ann Am Assoc Geogr. 2022;112:563-80.
27. World Health Organization. Alcohol, total per capita (15+) consumption (in litres of pure alcohol) (SDG Indicator 3.5.2). In: Repository GHOD, editor. 2025. Available from: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/total-(recorded-unrecorded)-alcohol-per-capita-(15-)-consumption. [Last accessed on 17 Jun 2026].
28. Kim SY, Kim HJ. Trends in alcohol consumption for korean adults from 1998 to 2018: korea national health and nutritional examination survey. Nutrients. 2021;13:609.
29. Hong JW, Noh JH, Kim DJ. The prevalence of and factors associated with high-risk alcohol consumption in Korean adults: the 2009-2011 Korea National Health and Nutrition Examination Survey. PLoS One. 2017;12:e0175299.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].