


Incretin-based therapy for MASH: are two better than one?
 0
0 
INTRODUCTION
Metabolic dysfunction-associated steatotic liver disease (MASLD) has become a global health problem affecting almost 40% of the adult population, with the highest prevalence in those with type 2 diabetes mellitus (T2DM)[1,2] and obesity[3]. MASLD can present as simple steatosis (defined as at least 5% fat in the liver), steatosis with inflammation (steatohepatitis), or steatohepatitis with hepatocyte ballooning and fibrosis (metabolic dysfunction-associated steatohepatitis, MASH). Because those with MASH are at highest risk of developing cirrhosis and liver-related outcomes [hepatic decompensation and hepatocellular carcinoma (HCC)], that has been the MASLD group targeted for therapy.
In the last few years, two therapies have been approved for MASH with stage 2-3 fibrosis (F2-3). The primary outcomes of these trials are an improvement in MASH without worsening fibrosis and improvements in fibrosis without worsening MASH. Resmetirom, approved in 2024, targets the thyroid hormone receptor beta (THR-β)[4]. In the phase 3, 240-week study, patients were randomized to resmetirom 80 mg, 100 mg, or placebo. Of the 996 enrolled subjects, steatohepatitis resolution was achieved in 25.9% (80 mg dose) and 29.9% (100 mg dose) compared to 9.7% in those on placebo. Fibrosis improvements were observed in 24.2% (80 mg dose) and 25.9% (100 mg dose) compared to 14.2% on placebo[5]. Incretin-based therapy for MASH can include a glucagon-like peptide 1 (GLP-1) receptor agonist (RA) alone or in dual-target combination with a glucose-dependent insulinotropic polypeptide (GIP) agonist or glucagon RA[6].
In 2025, incretin-based therapy with Semaglutide (a GLP-1 RA) was approved. In the phase 3, 72-week study, 1,197 patients with F2-3 MASH were randomized 2:1 to subcutaneous semaglutide 2.4 mg/week or placebo, with 62.9% achieving steatohepatitis resolution and 36.8% achieving reduction in fibrosis compared to 34.3% steatohepatitis resolution and 22.4% fibrosis reduction in those on placebo[7]. Dual-acting agents are another therapy option. In a phase 2 trial, tirzepatide (GLP-1 RA/GIP agonist) demonstrated 56%-62% achieving resolution of MASH and 51% achieving at least 1 stage of fibrosis compared to 10% MASH resolution and 30% fibrosis improvement in those on placebo[8]. Similarly, in a phase 2 study of survodutide (GLP-1 RA/glucagon RA) in MASH with F1-3, 62% had improvement in MASH and 34% had improvement in fibrosis compared to 14% improvement in MASH and 22% in fibrosis in the placebo group[9]. All these trials are somewhat limited by drug side effects and discontinuations.
RESEARCH SUMMARY
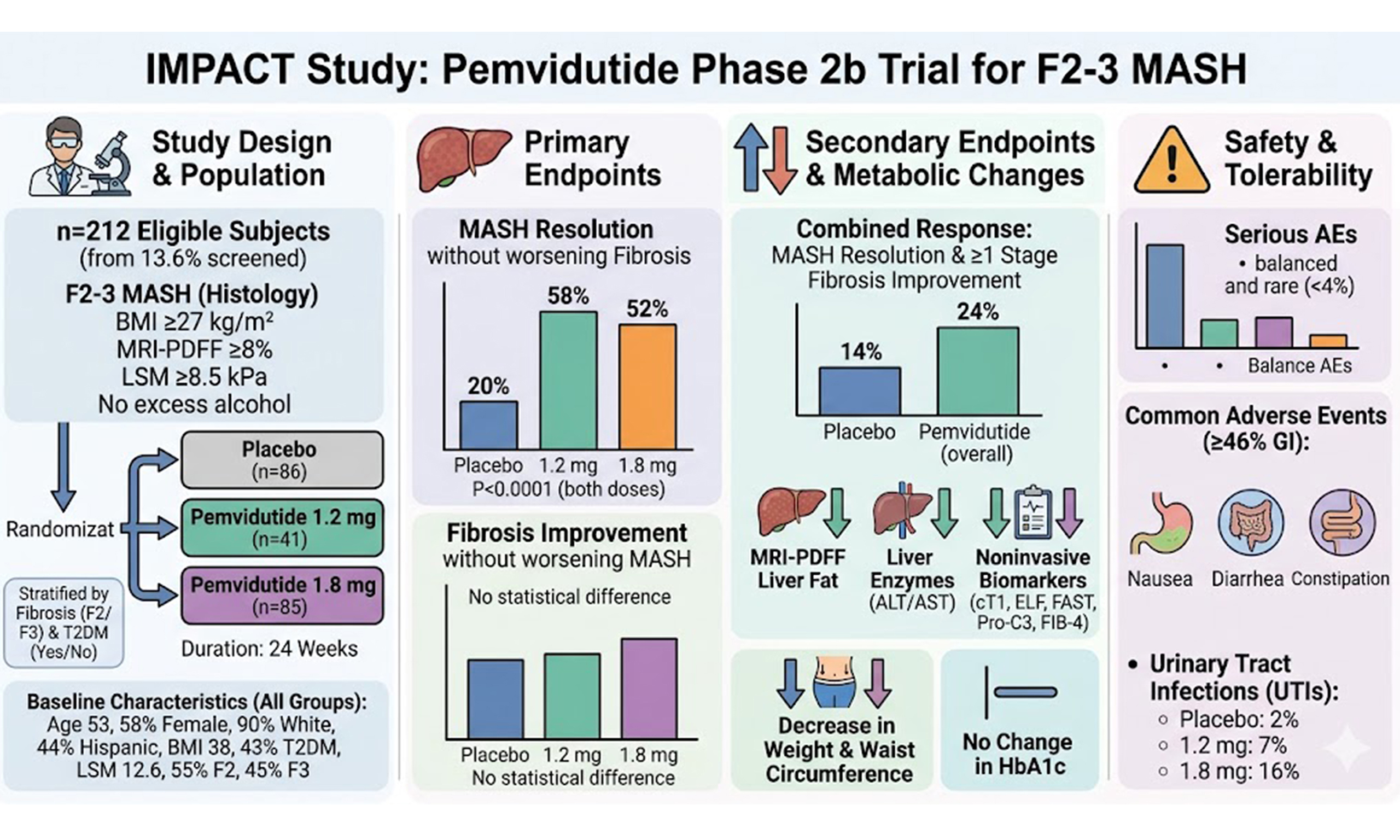
As opposed to the prior studies of GLP-1 RA or dual drugs that often require starting at a lower dose then increasing to the desired dose if tolerated, the pharmacokinetic properties of pemvidutide (GLP-1 RA/glucagon RA) allow starting at the target dose. In the current phase 2b study, Noureddin and colleagues studied the safety and efficacy of weekly pemvidutide in patients with F2-3 MASH (IMPACT)[10]. In this phase 2 study, 212 eligible subjects (13.6% of those screened) were randomized to 24 weeks of pemvidutide 1.2 mg (n = 41), 1.8 mg (n = 85), or placebo (n = 86) stratified by fibrosis (F2 or F3) and presence/absence of T2DM. All subjects had MASH (F2-3 by histology, a body mass index (BMI) of at least 27 kg/m2, fat fraction by magnetic resonance imaging-proton density fat fraction (MRI-PDFF) of at least 8%, and liver stiffness measurement (LSM) of at least 8.5 kPa without excess alcohol use. Primary end points were improvement in MASH without worsening fibrosis and improvements in fibrosis without worsening MASH. Secondary endpoints were proportion achieving both MASH resolution and fibrosis improvement, change in MRI-PDFF fat fraction, liver enzymes, and several noninvasive biomarkers [corrected T1 (cT1) relaxation, enhanced liver fibrosis (ELF) test, FibroScan-asparate aminotransferase (FAST), Pro-C3 and fibrosis-4 (FIB-4) index]. The groups were well matched: age 53 years, 58% female, 90% White, 44% Hispanic, BMI 38 kg/m2, 43% had T2DM, LSM 12.6 kPa with 55% F2 and 45% F3.
MASH resolution without worsening of fibrosis was observed in 58% in the 1.2 mg group and 52% in the
LIMITATIONS AND CONCLUSIONS
The mainstay for management of all patients with MASLD includes minimizing alcohol use, healthy lifestyle including weight loss through diet and exercise, and identification of cardiovascular and kidney disease. This often requires a multidisciplinary team. In those with MASH, identified through noninvasive tests (FIB-4, elastography, ELF, or other “at risk MASH” model), treatments can be considered. Those with cirrhosis will need HCC surveillance and screening for esophageal varices in those at risk. Incretin-based therapies for MASH seem to provide greater resolution of MASH without worsening of fibrosis compared to THR-β directed treatment.
However, there are several important differences across the trials and cross-trial comparison should be interpreted with caution due to differences in study design, treatment duration, and patient populations limiting comparisons [Table 1]. In the current trial, while the primary end point of MASH improvement was met, patients on pemvidutide did not have improved fibrosis compared to placebo. This may have been due to the shorter duration of treatment (24 weeks) compared to other studies with longer duration (52-72 weeks), engagement of differential pathways, or sampling error associated with liver biopsy. However, because the study showed decreases in several noninvasive biomarkers, future studies of longer duration will be able to address that limitation. Because obesity is common in those with MASLD, weight loss is an important secondary benefit of incretin therapies that may not occur in those on THR-β directed treatment. In this trial, moderate weight loss was seen. For other GLP-1 RA treatments that also have use in primary treatments of T2DM, use of pemvidutide did not have a significant change in HbA1c compared to placebo. This may be due to the relative proportion of GLP-1 RA compared to the other drug (glucagon RA in this case). If this holds true in a larger phase 3 study, it may impact its use in those with T2DM. Notwithstanding these limitations, the study supports the need for a phase 3 trial of longer duration to determine if pemvidutide should be in the growing armamentarium in the treatment of MASH. Mechanistically, dual-target therapy, like pemvidutide may be better than GLP-1 RA monotherapy by targeting enhanced fatty acid oxidation, inhibition of lipogenesis, increased energy expenditure, and hepatic lipid mobilization in addition to the indirect effects on inflammation, insulin sensitivity and weight loss provided by GLP-1 RA providing greater fat loss without hyperglycemia. Additional data on noninvasive assessments of effectiveness to determine whether the drug should be continued to avoid liver biopsy, how long it should be continued, and the long-term sequelae of these agents are needed. Unlike treating other liver diseases like hepatitis C that only requires a defined course of treatment (8-12 weeks) with high cure rates (> 95%), MASH treatment may end up needing combinations of several drugs with different mechanisms [THR-β, incretins, and anti-fibrotics such as fibroblast growth factor 21 (FGF21) analogues] to reach comparable results. With our available data on incretin-based MASH treatment, it remains unclear if two are better than one.
Comparing incretin-based therapies in MASH
| Study author[Ref.] | Therapy | Target | Duration (weeks) | MASH resolution without worsening fibrosis | Fibrosis improvement without worsening MASH |
| Harrison et al.[5] | Resmetirom | THR-β RA | 52 | 25.9%-29.9%a | 24.2%-25.9% |
| Sanyal et al.[7] | Semaglutide | GLP-1 RA | 240 | 62.9% | 36.8% |
| Loomba et al.[8] | Tirzepatide | GLP-1 RA/GIP RA | 52 | 44%-62%b | 51%-55% |
| Sanyal et al.[9] | Survodutide | GLP-1 RA/Glucagon RA | 48 | 42%-62%c | 34%-36% |
| Noureddin et al.[10] | Pemvidutide | GLP-1 RA/Glucagon RA | 24 | 52%-58%d | 28%-36% |
DECLARATIONS
Authors’ contributions
The author contributed solely to the article.
Availability of data and materials
Not applicable.
AI and AI-assisted tools statement
The graphical abstract was generated using Google Gemini. The author reviewed and finalized the content and took full responsibility for its accuracy and originality.
Financial support and sponsorship
None.
Conflicts of interest
None.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Ho GJK, Tan FXN, Sasikumar NA, et al. High global prevalence of steatotic liver disease and associated subtypes: a meta-analysis. Clin Gastroenterol Hepatol. 2025;23:2423-32.e1.
2. Tilg H, Petta S, Stefan N, Targher G. Metabolic dysfunction-associated steatotic liver disease in adults: a review. JAMA. 2026;335:163-74.
3. Amangurbanova M, Huang DQ, Noureddin N, et al. A prospective study on the prevalence of MASLD in patients with type 2 diabetes and hyperferritinaemia. Aliment Pharmacol Ther. 2025;61:456-64.
4. Liu J, Yang F, Gao B, Yang L, Cao Y, Zhou Y. Resmetirom, the first FDA-approved drug for MASH: from drug discovery and action mechanisms to clinical trials. Arch Pharm Res. 2025;48:1299-313.
5. Harrison SA, Bedossa P, Guy CD, et al.; MAESTRO-NASH Investigators. A phase 3, randomized, controlled trial of resmetirom in NASH with liver fibrosis. N Engl J Med. 2024;390:497-509.
6. Brouwers B, Rao G, Tang Y, Rodríguez Á, Glass LC, Hartman ML. Incretin-based investigational therapies for the treatment of MASLD/MASH. Diabetes Res Clin Pract. 2024;211:111675.
7. Sanyal AJ, Newsome PN, Kliers I, et al.; ESSENCE Study Group. Phase 3 trial of semaglutide in metabolic dysfunction-associated steatohepatitis. N Engl J Med. 2025;392:2089-99.
8. Loomba R, Hartman ML, Lawitz EJ, et al.; SYNERGY-NASH Investigators. Tirzepatide for metabolic dysfunction-associated steatohepatitis with liver fibrosis. N Engl J Med. 2024;391:299-310.
9. Sanyal AJ, Bedossa P, Fraessdorf M, et al.; 1404-0043 Trial Investigators. A phase 2 randomized trial of survodutide in MASH and fibrosis. N Engl J Med. 2024;391:311-9.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0













Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].