

Atrial fibrillation density: biological signal or prognostic tool?
 0
0 
INTRODUCTION
Considerable research has sought to identify risk factors for ischemic stroke in atrial fibrillation (AF)[1] .The factors most commonly used in clinical practice to stratify this risk are largely comorbidities and demographic features. Whether features of the arrhythmia itself also influence stroke risk remains an open question. Efforts to address this question have largely focused on AF burden, with the proportion of time spent in AF appearing to independently predict stroke[2,3]. However, burden captures only a single dimension of a complex biological phenomenon, and current monitoring devices already provide readily accessible additional information that may yet prove useful.
The proportion of time spent in AF over any given period is not distributed uniformly – at a fixed arrhythmia burden, some patients have AF distributed over the entire monitoring period, whereas others have a single sustained epoch. AF density quantifies this temporal dispersion from low density (“brief, dispersed, disconnected AF episodes”) to high density (“consolidated, uninterrupted AF episodes”)[4,5]. For example, a 10% AF burden over a 10-day monitoring period could be due to 2.4 h per day over those 10 days (or 10% per day, a relatively lower density) or could be due to one continuous episode lasting 24 h (or 10% of the 240 h of monitoring, reflecting higher density). Prior work has shown that AF density modifies the yield of rhythm monitoring to detect AF recurrence[5]. Until recently, however, its prognostic significance remained unestablished.
Against this backdrop, Rosman et al. investigated the association between AF density and risk of incident ischemic stroke[4]. The investigators leveraged data from two clinical cohorts of patients (n = 12,868, median CHA2DS2-VASc 4) with cardiac implantable electronic devices (CIED). Using G-computation methods, they estimated that greater AF density was associated with a 1.75-fold increased risk of incident ischemic stroke. This association was independent of AF burden and consistent across a range of subgroups. In this Commentary, we discuss these findings and consider whether AF density reflects a causal biological signal, a useful prognostic tool, or both.
IS AF DENSITY A CAUSAL RISK FACTOR FOR ISCHEMIC STROKE?
Establishing AF density as a causal risk factor would advance our understanding of how AF promotes intracardiac thrombosis and could reveal a new therapeutic target for reducing ischemic stroke risk. While the presented findings are promising, at least two important sources of bias potentially preclude causal inference.
Although G-computation improves adjustment for known confounders, it cannot account for unmeasured or poorly measured confounders. Of potential importance is the contribution of left atrial cardiopathy, which is an independent risk factor for ischemic stroke and has been associated with increased AF burden[6,7]. It is therefore plausible that AF density is also correlated with atrial cardiopathy, which may confound the association of AF density with ischemic stroke [Figure 1A]. Indeed, a more abnormal atrial substrate may be prone to produce longer episodes of AF, though data are needed to establish the directionality of this association.
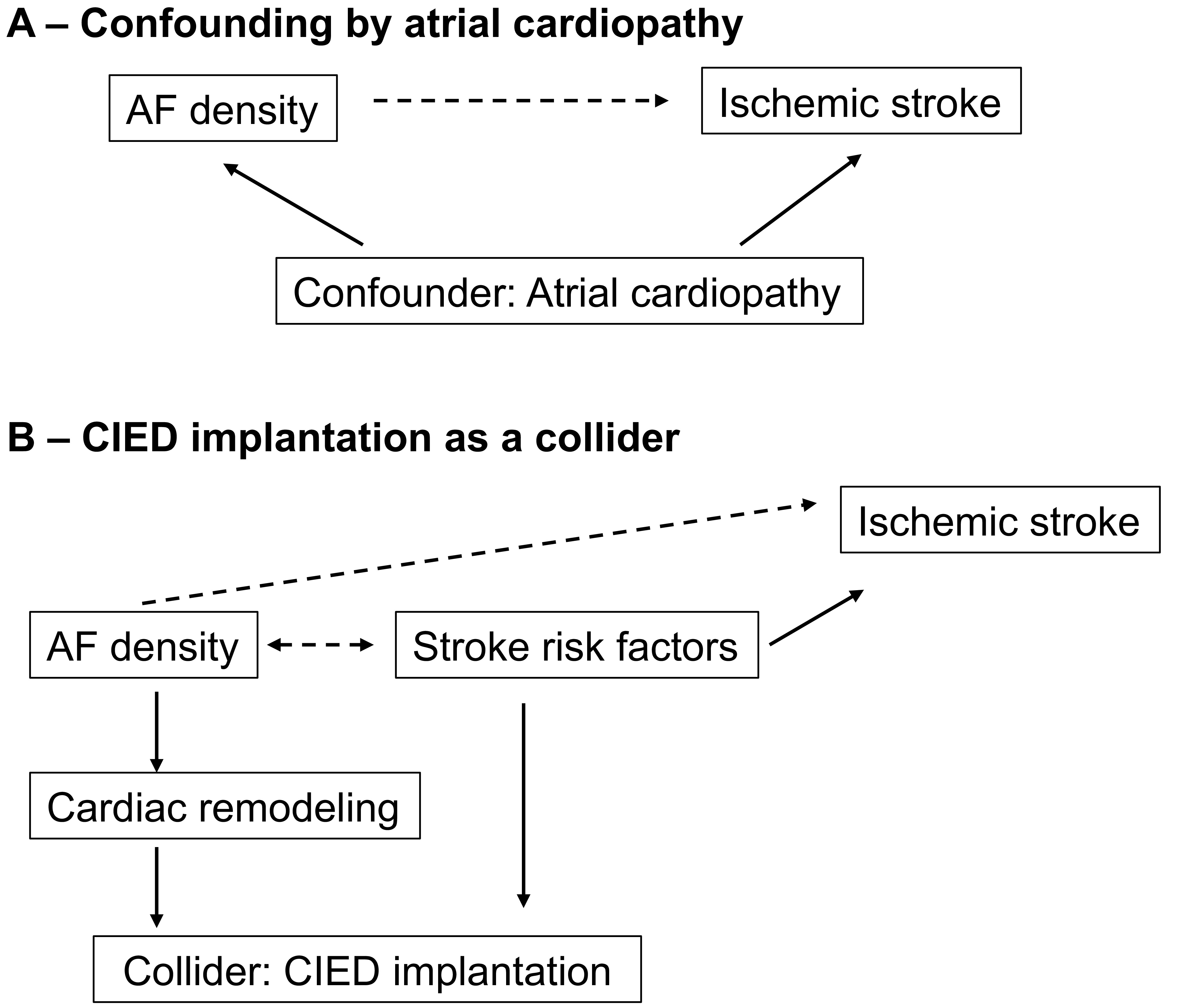
Figure 1. Directed acyclic graphs illustrating potential sources of bias in the association between AF density and ischemic stroke. The depicted biases include (A) confounding and (B) collider bias. Solid arrows represent causal relationships, while dashed arrows represent non-causal correlations induced by the respective biases. AF: Atrial fibrillation. CIED: cardiac implantable electronic devices.
It is well established that conditioning study participation on a variable (i.e., CIED implantation) can induce spurious associations with factors related to that variable, in a phenomenon known as collider bias [Figure 1B][8]. Independent replication in cohorts where continuous cardiac monitoring is applied uniformly, rather than conditional on clinical indication, would further strengthen the case for causality.
IS AF DENSITY A USEFUL PROGNOSTIC RISK FACTOR FOR ISCHEMIC STROKE?
Even without a causal relationship, AF density may still provide clinically relevant predictive information about stroke risk, helping to discriminate between those more or less likely to benefit from anticoagulation. Establishing such predictive value, however, is methodologically challenging in contemporary clinical cohorts[1]. Because CHA2DS2-VASc often determines oral anticoagulation (OAC) candidacy, any novel predictor is assessed in a population whose stroke risk may be modified by treatment decisions tied to the incumbent score. Indeed, the observed stroke risk of 6.3 per 1000 person-years in this study is far lower than that expected in an untreated AF cohort with a median CHA2DS2-VASc of 4.
One strategy to avoid this problem is to study patients with low CHA2DS2-VASc scores, for whom OAC is generally not indicated. Identifying risk factors that elevate stroke risk in such patients to levels comparable with high-risk groups could justify broadening OAC use in this population. Accordingly, estimating the relative and absolute ischemic stroke risks across AF density strata in patients with low CHA2DS2-VASc scores would be an important future direction.
CONCLUSIONS
The authors have carried out rigorous and foundational work on a clinically relevant topic. They are to be congratulated for providing compelling evidence pertinent to a new readily measurable AF biomarker that may ultimately be incorporated into stroke risk stratification. Triangulation of evidence, investigations of the interplay between AF density and atrial cardiopathy, and replication in independent unselected cohorts will be essential to establish the causal and prognostic significance of AF density for ischemic stroke[9].
DECLARATIONS
Authors’ contribution
Contributed to the conceptualization of the idea, critically revised the manuscript: Daghlas I, Marcus GM
Drafted the initial manuscript: Daghlas I
Availability of data and materials
Not applicable.
AI and AI-assisted tools statement
Not applicable.
Financial support and sponsorship
None.
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Lip GYH, Banerjee A, Boriani G, et al. Antithrombotic therapy for atrial fibrillation: CHEST guideline and expert panel report. Chest. 2018;154:1121-201.
2. Chen LY, Chung MK, Allen LA, et al.; American Heart Association Council on Clinical Cardiology, Council on Cardiovascular and Stroke Nursing, Council on Quality of Care and Outcomes Research, and Stroke Council. Atrial fibrillation burden: moving beyond atrial fibrillation as a binary entity: a scientific statement from the American Heart Association. Circulation. 2018;137:e623-44.
3. Joglar JA, Chung MK, Armbruster AL, et al.; Peer Review Committee Members. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2024;149:e1-e156.
4. Rosman L, Wang K, Sarkar S, Ziegler PD, Passman RS. Atrial fibrillation density as a biomarker for ischaemic stroke risk prediction. Eur Heart J. ;2026:ehag203.
5. Charitos EI, Stierle U, Ziegler PD, et al. A comprehensive evaluation of rhythm monitoring strategies for the detection of atrial fibrillation recurrence: insights from 647 continuously monitored patients and implications for monitoring after therapeutic interventions. Circulation. 2012;126:806-14.
6. Kamel H, Okin PM, Longstreth WT Jr, Elkind MS, Soliman EZ. Atrial cardiopathy: a broadened concept of left atrial thromboembolism beyond atrial fibrillation. Future Cardiol. 2015;11:323-31.
7. Bertelsen L, Diederichsen SZ, Haugan KJ, et al. Left atrial late gadolinium enhancement is associated with incident atrial fibrillation as detected by continuous monitoring with implantable loop recorders. JACC Cardiovasc Imaging. 2020;13:1690-700.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].