


Minimally invasive function-preserving pancreatic surgery: a single-center experience
 0
0 Abstract
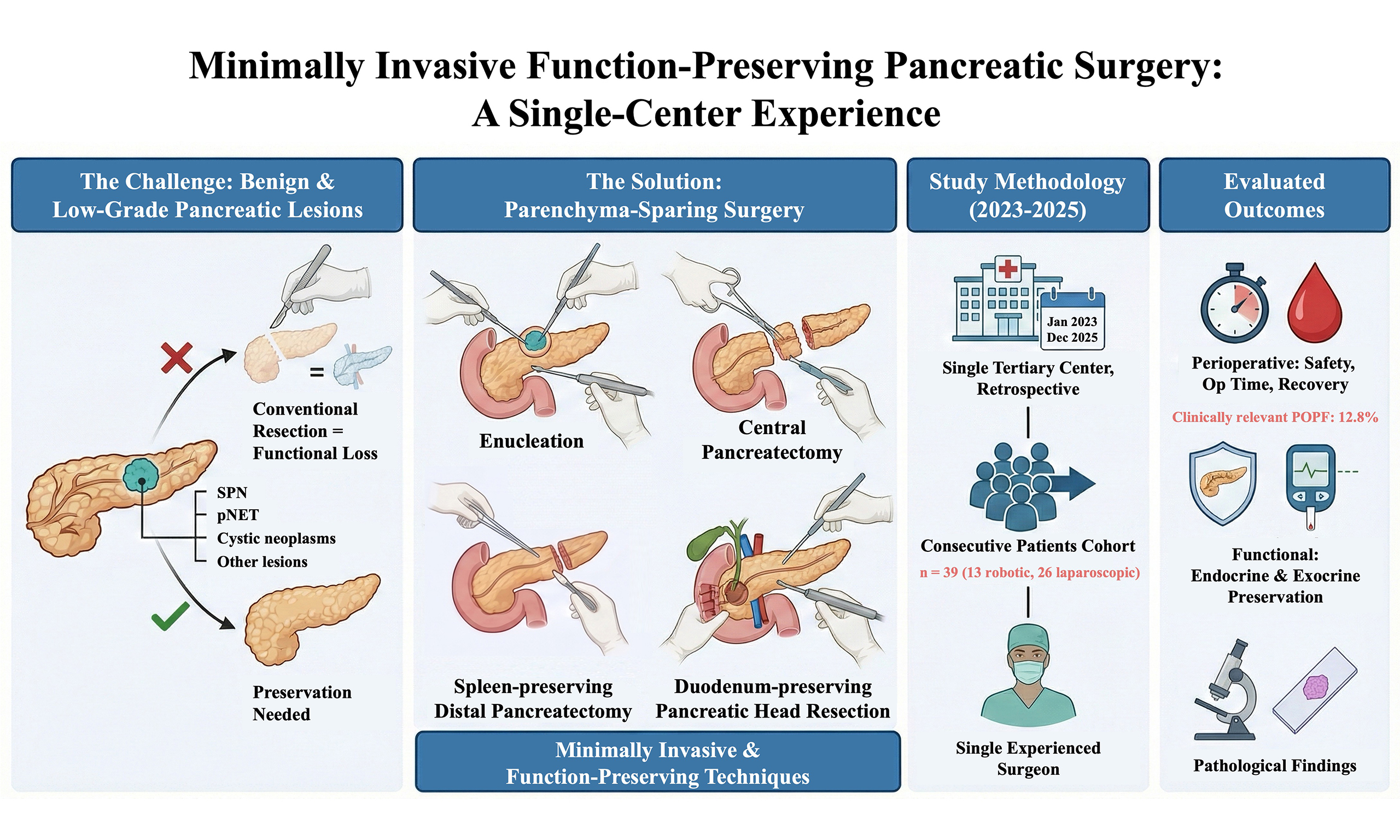
Aim: Minimally invasive function-preserving pancreatic surgery has emerged as a parenchyma-sparing strategy for benign or low-grade pancreatic lesions; however, evidence regarding perioperative safety and functional outcomes remains limited. This study aimed to evaluate perioperative outcomes, postoperative complications, functional results, and pathological findings following minimally invasive function-preserving pancreatic surgery in a single-center cohort.
Methods: This retrospective observational study included consecutive adult patients who underwent minimally invasive function-preserving pancreatic surgery between January 1, 2023, and December 31, 2025. All procedures were performed by a single experienced pancreatic surgeon. Surgical procedures included enucleation, central pancreatectomy, spleen-preserving distal pancreatectomy, and duodenum-preserving pancreatic head resection, performed using laparoscopic or robotic approaches. Perioperative outcomes, postoperative complications, functional outcomes, and pathological findings were analyzed descriptively.
Results: A total of 39 patients were included, comprising 13 robotic and 26 laparoscopic procedures. The median operative time was 240 min and median estimated blood loss was 200 mL. Clinically relevant postoperative pancreatic fistula (ISGPS grade B/C) occurred in 12.8% of patients, with no perioperative mortality or reoperation. New-onset diabetes mellitus developed in 7.7% of patients during follow-up. Pancreatic exocrine insufficiency was identified in 28.2% of patients based on clinical symptoms, and 41.0% required pancreatic enzyme replacement therapy. Pathological diagnoses predominantly included pancreatic neuroendocrine tumors, solid pseudopapillary neoplasms, and cystic pancreatic lesions.
Conclusion: Minimally invasive function-preserving pancreatic surgery is a feasible and safe option for selected patients with benign or low-grade pancreatic lesions, offering acceptable perioperative outcomes and preservation of pancreatic function when performed in experienced centers.
Keywords
INTRODUCTION
Pancreatic surgery is frequently associated with substantial postoperative morbidity, particularly involving pancreatic endocrine and exocrine dysfunction. Conventional pancreatic resections, such as pancreatoduodenectomy and distal pancreatectomy, involve removal of substantial functional pancreatic parenchyma and can be followed by long-term metabolic consequences, including new-onset diabetes mellitus and pancreatic exocrine insufficiency[1-3]. These functional impairments are of particular concern in patients with benign or low-grade malignant pancreatic lesions, who are expected to achieve long-term survival.
Function-preserving pancreatic surgery has therefore gained increasing attention as a parenchyma-sparing strategy aimed at preserving pancreatic function while achieving adequate disease control[4,5]. Procedures such as enucleation, central pancreatectomy, spleen-preserving distal pancreatectomy, and duodenum-preserving pancreatic head resection are increasingly performed in carefully selected patients, particularly those with pancreatic neuroendocrine tumors, solid pseudopapillary neoplasms, and cystic pancreatic lesions.
Alongside these developments, minimally invasive surgical approaches have further expanded the technical feasibility of function-preserving pancreatic procedures. Laparoscopic and robotic techniques may offer advantages in operative visualization, dissection precision, and postoperative recovery[6-8]. However, these procedures remain technically demanding, and the available evidence regarding perioperative safety and functional outcomes of minimally invasive function-preserving pancreatic surgery remains limited, being largely derived from small and heterogeneous series[9-11].
This study aimed to evaluate perioperative outcomes, postoperative complications, functional outcomes, and pathological characteristics in a consecutive single-center cohort undergoing minimally invasive function-preserving pancreatic surgery. By reporting our institutional experience, we sought to provide additional evidence regarding the safety, feasibility, and functional preservation of parenchyma-sparing pancreatic procedures in the minimally invasive setting.
METHODS
Study design and patient selection
This retrospective observational study included consecutive patients who underwent minimally invasive function-preserving pancreatic surgery at a single tertiary referral center between January 1, 2023, and December 31, 2025. All procedures were performed by a single experienced pancreatic surgeon to ensure procedural consistency. Patient selection, surgical classification, perioperative management, and data collection are summarized in the study flowchart [Figure 1].
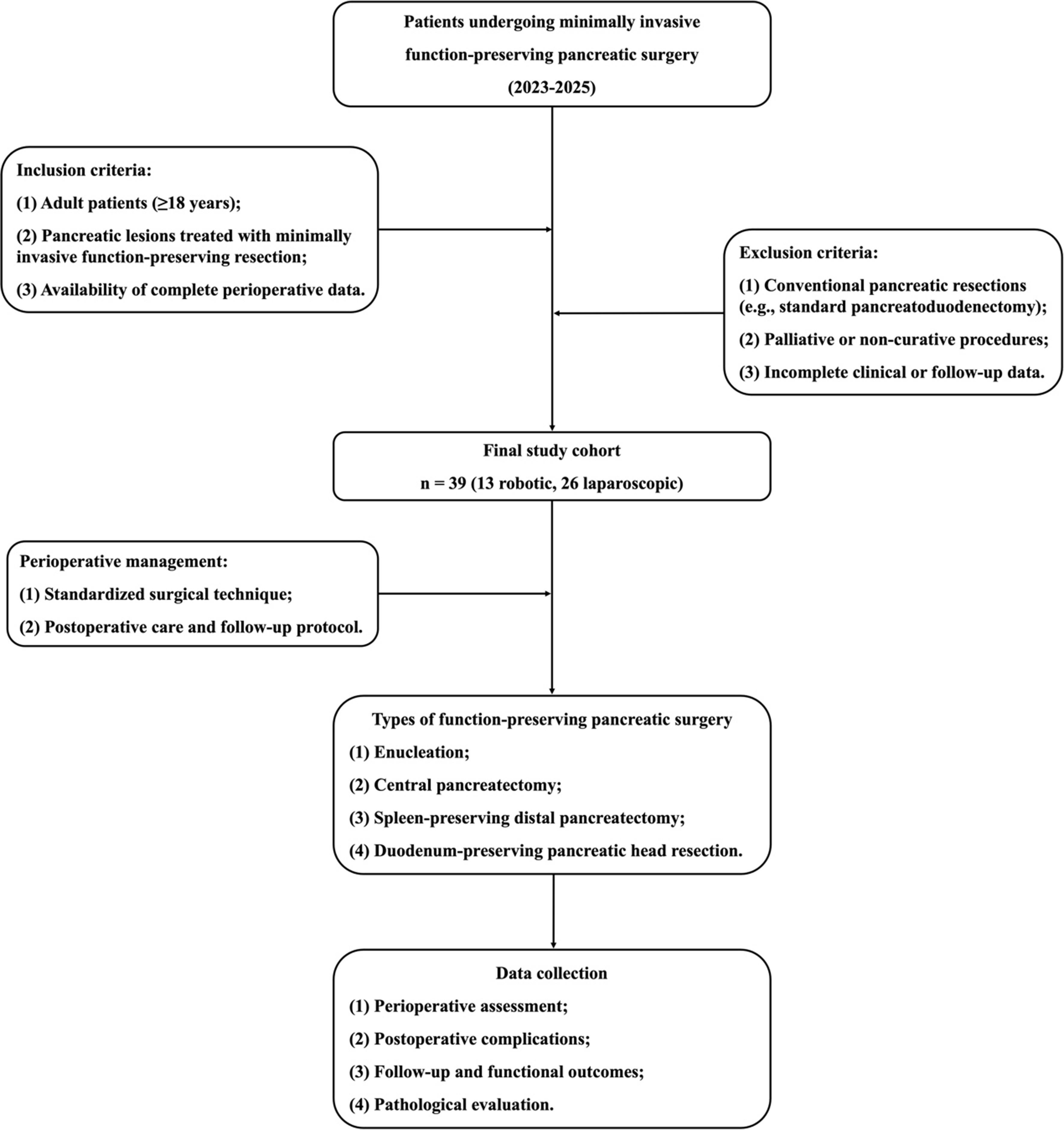
Figure 1. Study flowchart of patient selection and data collection. Flowchart illustrating patient inclusion and exclusion, the final study cohort, types of minimally invasive function-preserving pancreatic surgery, perioperative management, and data collection for analysis.
The inclusion criteria were as follows: (1) adult patients (≥ 18 years); (2) pancreatic lesions treated with minimally invasive function-preserving pancreatic surgery; and (3) availability of complete perioperative and follow-up data. The exclusion criteria included: (1) conventional pancreatic resections (e.g., standard pancreatoduodenectomy); (2) palliative or non-curative procedures; and (3) incomplete clinical or follow-up data.
A total of 39 patients were included in the final study cohort, including 13 robotic and 26 laparoscopic procedures.
Surgical techniques and perioperative management
Minimally invasive function-preserving pancreatic surgery included four main procedure types: enucleation, central pancreatectomy, spleen-preserving distal pancreatectomy, and duodenum-preserving pancreatic head resection. The choice of surgical approach and specific procedure was determined based on tumor location, size, biological behavior, and its relationship to the main pancreatic duct.
Enucleation was preferentially performed for small, well-circumscribed lesions located at a safe distance from the main pancreatic duct, with the aim of preserving maximal pancreatic parenchyma. Central pancreatectomy was considered for selected lesions located in the pancreatic neck or proximal body, allowing preservation of both the pancreatic head and tail. Spleen-preserving distal pancreatectomy was applied for lesions in the pancreatic body or tail, with preservation of the splenic vessels whenever feasible. Duodenum-preserving pancreatic head resection was reserved for benign or low-grade lesions confined to the pancreatic head and was performed using a modified Beger procedure with preservation of the duodenum and biliary tract. After duodenum-preserving pancreatic head resection and central pancreatectomy, the distal pancreatic stump was reconstructed with pancreaticojejunostomy, whereas the proximal stump was closed by suture when applicable.
Perioperative management followed a standardized institutional protocol, including parenchyma-preserving surgical techniques, standardized postoperative care pathways, and a structured follow-up program.
Patient positioning and trocar placement were standardized across all procedures. Patients were positioned supine with a slight reverse Trendelenburg tilt of approximately 15°-20°. The camera port was positioned along the midline, with bilateral working ports symmetrically arranged to ensure adequate exposure and optimal instrument triangulation [Figure 2].
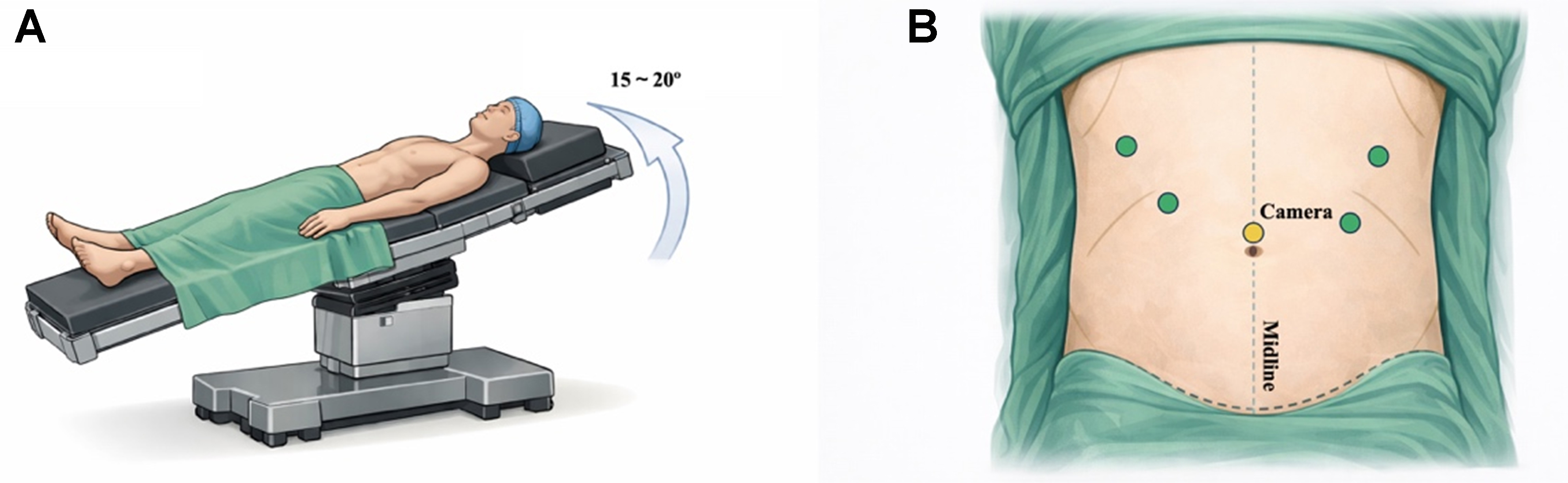
Figure 2. Patient positioning and trocar placement for minimally invasive function-preserving pancreatic surgery. (A) The patient is placed in the supine position with slight reverse Trendelenburg tilt (approximately 15°-20°); (B) Schematic illustration of trocar placement, with the camera port positioned at the midline and bilateral working ports arranged symmetrically to allow adequate exposure and instrument triangulation.
Figure 3A-D shows the preoperative magnetic resonance imaging findings of a pancreatic neuroendocrine tumor, whereas Figure 3E-P illustrates the key steps of minimally invasive enucleation, including tumor localization, pancreatic exposure, parenchyma-sparing dissection, hemostasis, specimen retrieval, and drain placement. Figure 4A-C shows the preoperative computed tomography findings of a solid pseudopapillary neoplasm, whereas Figure 4D-P demonstrates the main steps of robotic enucleation, including pancreatic exposure, intraoperative ultrasonography, stepwise tumor dissection, preservation of the main pancreatic duct, hemostatic management, specimen retrieval, and postoperative imaging confirmation.
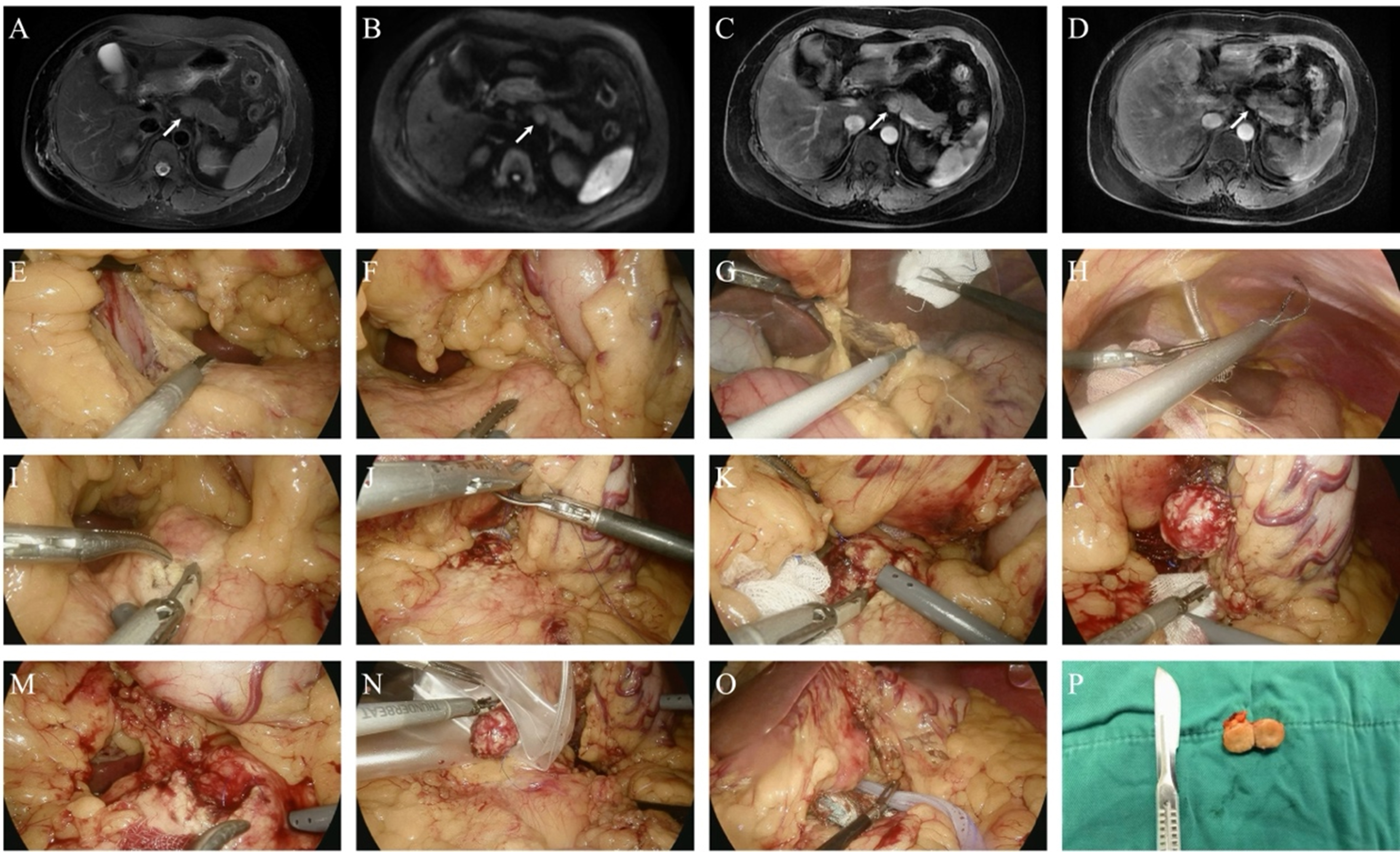
Figure 3. Representative minimally invasive enucleation of a pancreatic neuroendocrine tumor. (A-D) Preoperative magnetic resonance imaging demonstrating a well-circumscribed lesion located at the superior border of the pancreatic body, measuring approximately 1.7 cm in diameter, with slightly hyperintense signal on T2-weighted imaging, mild diffusion restriction on DWI, hyperenhancement in the arterial phase, isoenhancement in the venous phase, and no pancreatic duct dilation; (E) Adhesiolysis of the posterior gastric wall; (F) Identification of the tumor location; (G) Opening of the lesser sac; (H) Suspension of the stomach to the upper abdominal wall; (I) Incision of the pancreatic capsule along the tumor margin; (J) Suturing and suspension of the tumor; (K) Continued dissection of the lesion; (L) Complete enucleation of the tumor; (M) Ligation of arterial bleeding; (N) Specimen retrieval; (O) Placement of hemostatic materials and drainage; (P) Gross appearance of the resected specimen. DWI: Diffusion-weighted imaging.
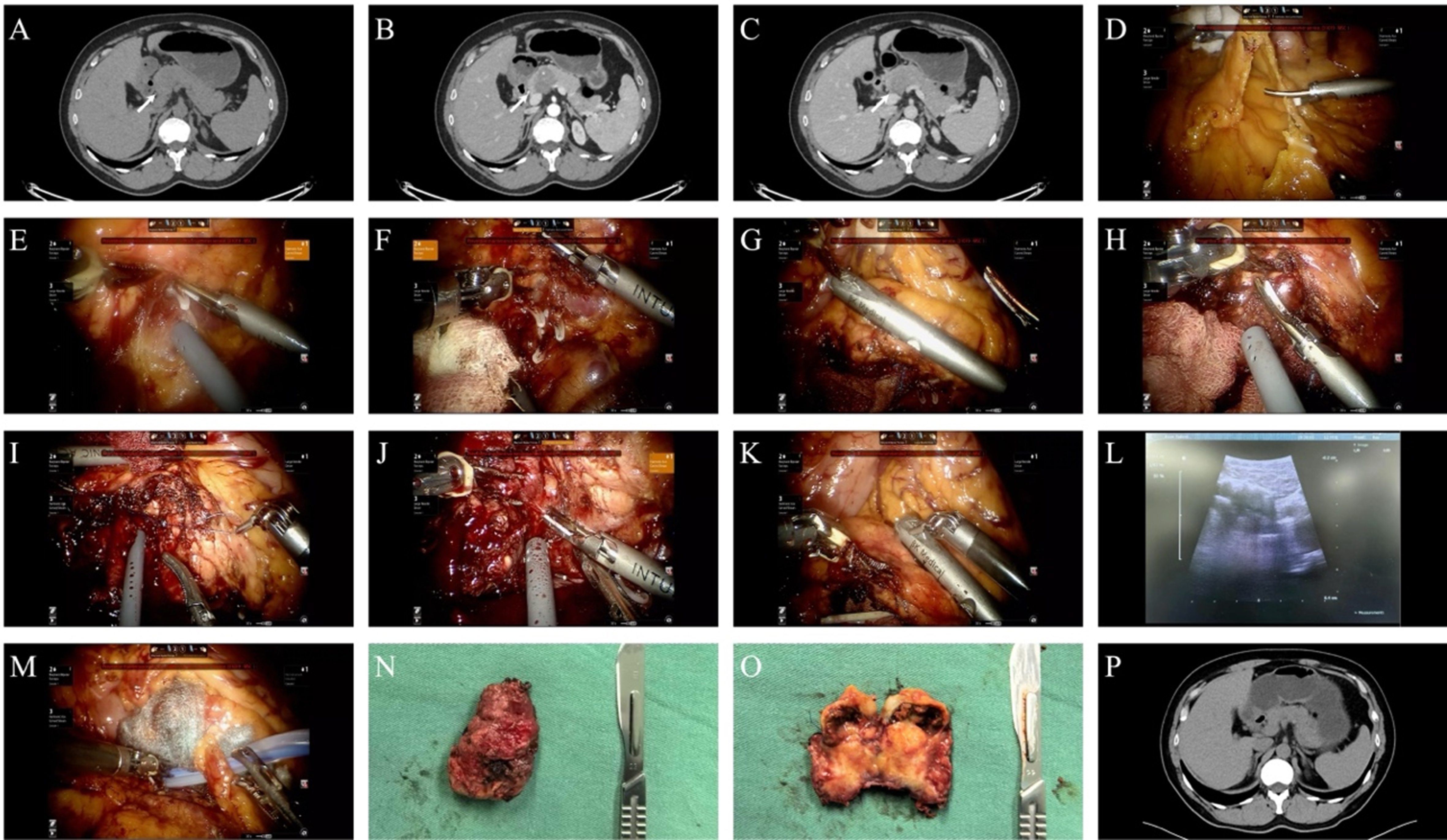
Figure 4. Representative robotic enucleation for a solid pseudopapillary neoplasm of the pancreas. (A-C) Contrast-enhanced computed tomography demonstrating a heterogeneous, relatively hypodense lesion at the pancreatic head–neck junction, measuring approximately 3.8 × 3.0 cm in maximal diameter, with focal calcifications, relative hypoenhancement, and no dilation of the main pancreatic duct; (D) Adhesiolysis; (E) Clip ligation and division of encountered ductal structures; (F) Opening of the gastrocolic ligament to expose the pancreas; (G) Intraoperative ultrasonography revealing a heterogeneous hypoechoic lesion; (H) Stepwise transection of pancreatic parenchyma using an ultrasonic scalpel; (I) Suture ligation of arterial bleeding; (J) Complete enucleation of the lesion with preservation of surrounding pancreatic parenchyma; (K and L) Repeat intraoperative ultrasonography confirming integrity of the main pancreatic duct; (M) Placement of hemostatic materials and surgical drainage; (N and O) Gross appearance of the resected specimen; (P) Postoperative computed tomography showing no abnormal findings and no pancreatic duct dilation.
Data collection and outcome measures
Clinical data were extracted from electronic medical records and prospectively maintained institutional databases. Collected data included: (1) perioperative variables, including operative time, estimated blood loss, conversion to open surgery, and length of hospital stay; (2) postoperative complications, classified according to the Clavien–Dindo classification system; (3) follow-up and functional outcomes, including pancreatic endocrine and exocrine function, changes in body weight, and the requirement for pancreatic enzyme replacement therapy; and (4) pathological outcomes based on final histopathological diagnosis.
Postoperative pancreatic fistula (POPF), delayed gastric emptying, and postpancreatectomy hemorrhage were defined and graded according to established international consensus criteria. Biochemical leak was recorded separately according to the updated International Study Group of Pancreatic Surgery (ISGPS) definition and was not classified as a clinically relevant POPF. Overall clinically relevant postoperative morbidity, as well as readmission and mortality, were additionally assessed within 90 days after surgery. Pancreatic exocrine insufficiency was assessed based on clinical symptoms and the need for pancreatic enzyme supplementation.
Statistical analysis
Continuous variables were summarized as medians with interquartile ranges (IQRs), and categorical variables were presented as counts and percentages. All statistical analyses were performed using SPSS version 27.0 (IBM Corp., Armonk, NY, USA) and R software version 4.5.1 (R Foundation for Statistical Computing, Vienna, Austria). Given the descriptive nature of this study and the limited sample size, no formal hypothesis testing was performed.
RESULTS
Patient characteristics and tumor features
A total of 39 consecutive patients who underwent minimally invasive function-preserving pancreatic surgery were included in the analysis. Baseline patient characteristics are summarized in Table 1. The median age was 55 years (IQR, 36-67), and 22 patients (56.4%) were female. The median body mass index was 24.7 kg/m2 (IQR, 22.2-27.1). Most patients were classified as American Society of Anesthesiologists (ASA) physical status I-II (34/39, 87.2%), and the median Charlson Comorbidity Index was 0 (IQR, 0-1).
Baseline characteristics of patients
| Characteristic | Value |
| No. of patients | 39 |
| Age, years | 55 (36-67) |
| Sex (male/female), n | 17/22 |
| Body mass index, kg/m2 | 24.7 (22.2-27.1) |
| ASA score (I-II/III-IV), n | 34/5 |
| Charlson Comorbidity Index | 0 (0-1) |
| Pre-existing diabetes mellitus, n (%) | 1 (2.6%) |
| Preoperative hypoglycemia, n (%) | 7 (17.9%) |
| Pre-existing pancreatic exocrine insufficiency, n (%) | 2 (5.1%) |
| Symptomatic presentation, n (%) | 19 (48.7%) |
| Incidentally detected, n (%) | 20 (51.3%) |
| Tumor configuration (solitary/multilocular or lobulated), n | 33/6 |
| Tumor location (head/body/tail), n | 10/10/19 |
| Tumor size, cm | 3.0 (2.0-4.5) |
| Cystic lesion, n (%) | 15 (38.5%) |
Pre-existing diabetes mellitus was present in 1 patient (2.6%), whereas preoperative hypoglycemia was observed in 7 patients (17.9%). Pre-existing pancreatic exocrine insufficiency was documented in 2 patients (5.1%). Nineteen patients (48.7%) were symptomatic at presentation, whereas 20 patients (51.3%) were diagnosed incidentally.
Regarding tumor characteristics, most lesions were solitary (33/39, 84.6%), whereas 6 patients (15.4%) had multilocular or lobulated cystic lesions rather than truly separate tumors. Tumors were located in the pancreatic head, body, and tail in 10 (25.6%), 10 (25.6%), and 19 patients (48.7%), respectively. The median tumor size was 3.0 cm (IQR, 2.0-4.5), and cystic lesions accounted for 38.5% of cases (15/39).
Operative characteristics and perioperative outcomes
Operative characteristics and perioperative outcomes are summarized in Table 2. Thirteen procedures (33.3%) were performed using a robotic approach, whereas 26 cases (66.7%) were completed laparoscopically. Spleen-preserving distal pancreatectomy was the most frequently performed procedure (24 cases, 61.6%), followed by duodenum-preserving pancreatic head resection (9 cases, 23.1%), enucleation (5 cases, 12.8%), and central pancreatectomy (1 case, 2.6%).
Operative characteristics and perioperative outcomes
| Variable | Value |
| Surgical approach (robotic/laparoscopic), n | 13/26 |
| Type of procedure | |
| - Enucleation, n (%) | 5 (12.8%) |
| - Central pancreatectomy, n (%) | 1 (2.6%) |
| - Spleen-preserving distal pancreatectomy, n (%) | 24 (61.6%) |
| - Duodenum-preserving pancreatic head resection, n (%) | 9 (23.1%) |
| Operative time, min | 240 (200-340) |
| Estimated blood loss, mL | 200 (50-400) |
| Conversion to open surgery, n (%) | 1 (2.6%) |
| Intraoperative transfusion, n (%) | 6 (15.4%) |
| Intraoperative ultrasound use, n (%) | 12 (30.8%) |
| Drain placement, n (%) | 39 (100%) |
| Postoperative ICU admission, n (%) | 4 (10.3%) |
| Length of hospital stay, days | 9 (6.5-11.5) |
The median operative time was 240 min (IQR, 200-340), and the median estimated blood loss was 200 mL (IQR, 50-400). Conversion to open surgery occurred in 1 patient (2.6%). Intraoperative blood transfusion was required in 6 patients (15.4%), and intraoperative ultrasound was used in 12 cases (30.8%). Abdominal drain placement was performed in all patients. Postoperative admission to the intensive care unit was required in 4 patients (10.3%). The median length of hospital stay was 9 days (IQR, 6.5-11.5).
Postoperative complications
Postoperative outcomes are summarized in Table 3. Overall clinically relevant postoperative complications occurred in 7 patients (17.9%), with some patients experiencing more than one complication. Clinically relevant POPF was observed in 5 patients (12.8%), whereas biochemical leak, recorded separately as a non–clinically relevant ISGPS category, was identified in 33 patients (84.6%). Delayed gastric emptying occurred in 5 patients (12.8%), and postpancreatectomy hemorrhage was noted in 2 patients (5.1%). No patient required reoperation, and no 30-day mortality was observed. The 90-day morbidity, readmission, and mortality rates were 17.9%, 15.4%, and 0%, respectively.
Postoperative complications
| Outcome | Value |
| Overall clinically relevant postoperative complications, n (%) | 7 (17.9%) |
| Clinically relevant POPF (ISGPS grade B/C), n (%) | 5 (12.8%) |
| Biochemical leak, n (%) | 33 (84.6%) |
| Delayed gastric emptying, n (%) | 5 (12.8%) |
| Postpancreatectomy hemorrhage, n (%) | 2 (5.1%) |
| Reoperation, n (%) | 0 (0%) |
| 90-day morbidity, n (%) | 7 (17.9%) |
| 30-day readmission, n (%) | 6 (15.4%) |
| 90-day readmission, n (%) | 6 (15.4%) |
| Clavien–Dindo grade I-II, n (%) | 32 (82.1%) |
| Clavien–Dindo grade ≥ III, n (%) | 5 (12.8%) |
| No postoperative complications, n (%) | 2 (5.1%) |
| 30-day mortality, n (%) | 0 (0%) |
| 90-day mortality, n (%) | 0 (0%) |
According to the Clavien–Dindo classification, 32 patients (82.1%) experienced grade I-II complications, whereas 5 patients (12.8%) developed grade III or higher complications. Thirty-day readmission was recorded in 6 patients (15.4%).
Functional outcomes and pathological findings
Functional outcomes during follow-up and pathological findings are summarized in Table 4. The median follow-up duration was 9 months (IQR, 4-21.5). New-onset diabetes mellitus developed in 3 patients (7.7%) during follow-up. The median change in blood glucose level during follow-up was 0.86 mmol/L (IQR, 0.08-2.17). Individual preoperative and postoperative blood glucose values are illustrated in Figure 5.
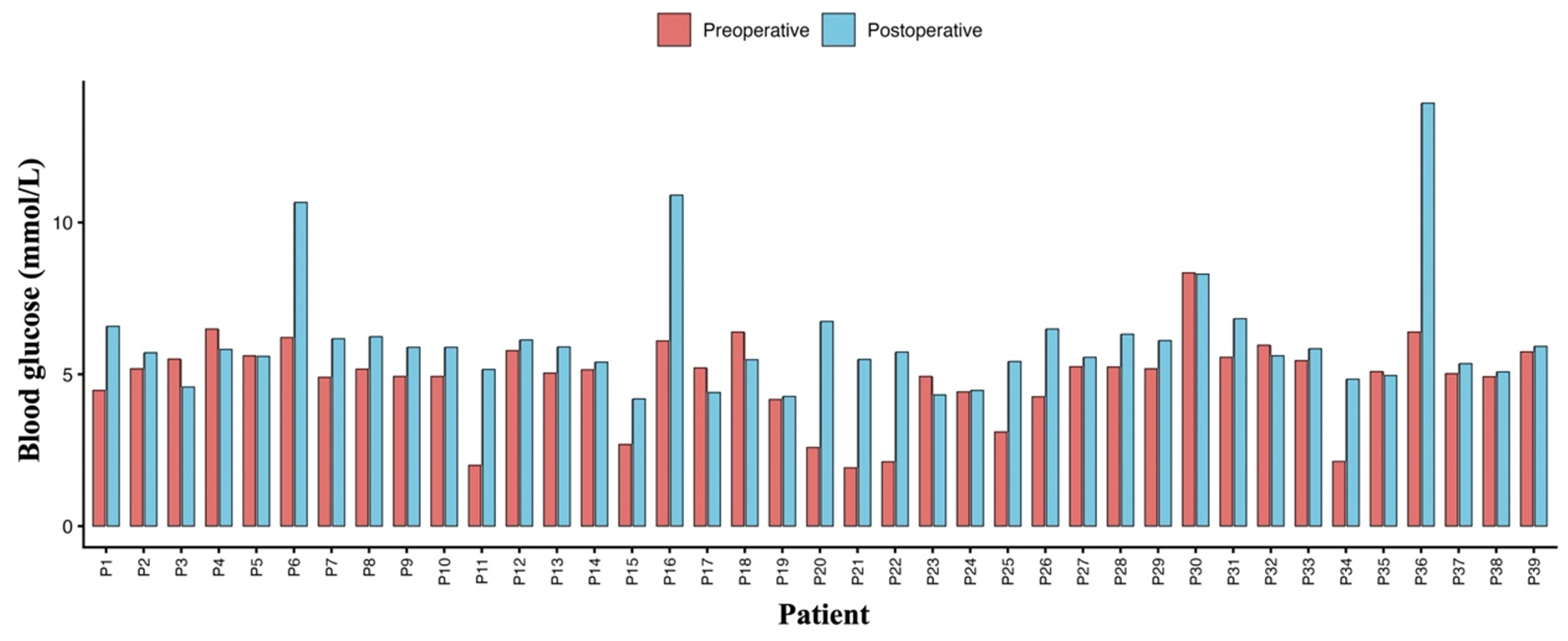
Figure 5. Individual blood glucose levels before and after function-preserving pancreatic surgery. Paired bar chart showing preoperative and postoperative blood glucose levels for each patient (P1-P39). Red bars represent preoperative measurements, and blue bars represent postoperative values obtained during follow-up. Blood glucose levels are expressed in mmol/L.
Functional outcomes during follow-up and pathological findings
| Functional outcome | Value |
| Median follow-up, months | 9 (4-21.5) |
| New-onset diabetes mellitus, n (%) | 3 (7.7%) |
| Blood glucose change during follow-up, mmol/L | 0.86 (0.08-2.17) |
| Pancreatic exocrine insufficiency, n (%) | 11 (28.2%) |
| Need for pancreatic enzyme replacement therapy, n (%) | 16 (41.0%) |
| Body weight change, kg | -1.5 (-3.0 to 0.5) |
| Final pathological diagnosis | |
| - SPN, n (%) | 11 (28.2%) |
| - pNET, n (%) | 11 (28.2%) |
| - G1 | 6 |
| - G2 | 5 |
| - Cystic neoplasms, n (%) | 14 (35.9%) |
| - IPMN | 5 |
| - MCN | 4 |
| - SCN | 5 |
| - Other lesions | 3 (7.7%) |
Pancreatic exocrine insufficiency was identified in 11 patients (28.2%), and 16 patients (41.0%) required pancreatic enzyme replacement therapy during follow-up. The median body weight change was -1.5 kg (IQR, -3.0 to 0.5).
Final pathological diagnoses included solid pseudopapillary neoplasm in 11 patients (28.2%) and pancreatic neuroendocrine tumors in 11 patients (28.2%), comprising 6 grade G1 and 5 grade G2 tumors. Cystic neoplasms were identified in 14 patients (35.9%), including intraductal papillary mucinous neoplasm (n = 5), mucinous cystic neoplasm (n = 4), and serous cystic neoplasm (n = 5). Other pathological findings were observed in 3 patients (7.7%), including one unexpected moderately differentiated pancreatic ductal adenocarcinoma despite preoperative imaging and intraoperative frozen section favoring a neuroendocrine tumor. Robotic duodenum-preserving pancreatic head resection with peripancreatic lymph node dissection was performed in this patient, and no nodal metastasis or recurrence was observed during 8 months of follow-up.
DISCUSSION
In this single-center experience, minimally invasive function-preserving pancreatic surgery demonstrated acceptable perioperative safety, a manageable postoperative complication profile, and favorable functional outcomes in carefully selected patients with benign or low-grade pancreatic lesions. The absence of perioperative mortality and a clinically relevant POPF rate of 12.8% support the feasibility of minimally invasive parenchyma-sparing pancreatic procedures in experienced centers. Similar findings have been reported in recent series, indicating that minimally invasive enucleation and other parenchyma-sparing resections can achieve morbidity rates comparable to open surgery, with potential advantages in postoperative recovery and length of hospital stay; however, high-quality evidence remains limited[5,11,12].
POPF remains the principal concern following function-preserving pancreatic surgery, as preservation of pancreatic parenchyma and transection in close proximity to the main pancreatic duct inherently increase the risk of pancreatic leakage[13]. In the present cohort, although biochemical leakage was common, the incidence of clinically relevant POPF was relatively low compared with rates reported in several recent series of minimally invasive central pancreatectomy. These studies suggest that minimally invasive approaches are associated with comparable or even lower rates of clinically relevant POPF than open surgery, while offering the additional benefit of reduced intraoperative blood loss[14,15]. Importantly, no patient in our series required reoperation, and severe morbidity was uncommon, indicating that although POPF was frequent, it was generally manageable within a minimally invasive treatment framework.
Beyond patient selection, several pragmatic, procedure-specific strategies in our institutional practice may have contributed to reducing the incidence and severity of clinically relevant POPF. Preoperative cross-sectional imaging was systematically reviewed to delineate the anatomical relationship between the lesion and the main pancreatic duct, thereby guiding operative planning. In one patient with a lesion in close proximity to the pancreatic duct, a deliberately limited local resection was performed, accompanied by selective placement of a prophylactic intraductal pancreatic stent to facilitate ductal drainage and reduce intrapancreatic pressure. This was not used routinely in our series and remains to be further optimized with increasing experience. Intraoperatively, ultrasonography was selectively employed in real-world practice, particularly in cases requiring additional assessment of tumor localization and the tumor–main pancreatic duct relationship, to facilitate precise parenchyma-sparing dissection and reduce the risk of ductal injury. It may also serve as a valuable adjunct for defining the optimal site of pancreatic transection and guiding more accurate tumor localization in parenchyma-sparing procedures. Postoperatively, closed-suction drains were routinely positioned adjacent to the resection site and securely fixed to ensure effective drainage. This approach was intended not only to monitor pancreatic leakage but also to reduce the risk of secondary complications, including infection or hemorrhage necessitating interventional drainage or reoperation. Collectively, these individualized, anatomy-based measures may partly explain why, despite a high incidence of biochemical leakage, clinically relevant POPF remained largely manageable in our cohort.
Function-preserving pancreatic surgery comprises a heterogeneous group of procedures, each associated with distinct technical challenges and complication risk profiles. Enucleation and central pancreatectomy are typically associated with higher fistula rates, largely due to limited resection margins and close proximity to the main pancreatic duct, whereas spleen-preserving distal pancreatectomy and duodenum-preserving pancreatic head resection involve more extensive dissection but may allow better ductal control[16,17]. Recent studies have demonstrated that minimally invasive duodenum-preserving pancreatic head resection can be performed safely with acceptable outcomes when undertaken in high-volume centers by experienced surgeons[18]. In our series, overall complication rates across different procedures were acceptable, suggesting that tailored, anatomy-based selection of parenchyma-sparing techniques is essential for balancing oncologic adequacy with functional preservation. Careful preoperative evaluation remains crucial for appropriate case selection, particularly when malignancy cannot be confidently excluded.
The adoption of minimally invasive techniques has further expanded the feasibility of function-preserving pancreatic surgery. Enhanced visualization, improved instrument articulation, and refined dissection planes provided by laparoscopic and robotic platforms may facilitate precise parenchyma-sparing resections while minimizing surgical trauma[19-22]. Although these procedures remain technically demanding and are associated with a steep learning curve, this evolution parallels broader trends in minimally invasive pancreatic surgery, whereby robotic and laparoscopic approaches have gradually gained acceptance and are increasingly endorsed by contemporary guidelines for selected pancreatic resections when performed by specialized teams[23]. Our experience, in which all procedures were performed by a single experienced pancreatic surgeon, underscores the importance of technical expertise and procedural consistency in achieving favorable outcomes.
Preservation of pancreatic endocrine function represents a key theoretical advantage of function-preserving pancreatic surgery. In the present study, new-onset diabetes mellitus occurred in only 7.7% of patients during follow-up, a rate substantially lower than that reported after conventional pancreatic resections. This finding supports the concept that preservation of pancreatic parenchyma translates into meaningful metabolic benefits, particularly in patients without pre-existing glucose intolerance. A recent comparison of laparoscopic enucleation vs. formal resection for pancreatic neuroendocrine neoplasms also suggests a potential advantage of parenchyma-sparing techniques in preserving endocrine function, although long-term data remain limited[12]. Although longer follow-up is required to confirm the durability of these findings, the present results further reinforce the functional rationale for parenchyma-sparing approaches.
Pancreatic exocrine insufficiency is more difficult to interpret, given the complex interplay among pancreatic volume, ductal integrity, and postoperative inflammation. In our cohort, pancreatic exocrine insufficiency was identified in 28.2% of patients based on clinical symptoms, and symptoms were effectively controlled with pancreatic enzyme supplementation when required. Although this incidence is not negligible, it compares favorably with rates reported after standard pancreatic resections and underscores the multifactorial nature of postoperative digestive dysfunction. Parenchyma-preserving approaches, particularly for cystic pancreatic lesions, have been shown to preserve exocrine function without increasing the risk of severe complications, further supporting the functional benefits of these strategies in carefully selected patients[4,24,25]. Importantly, most patients maintained satisfactory nutritional status, as indicated by only modest changes in body weight during follow-up.
When placed in the context of existing literature, our findings are consistent with previously reported experiences summarized in Table 5. Most available studies on minimally invasive function-preserving pancreatic surgery are retrospective, single-center series characterized by limited sample sizes and heterogeneous indications. Reported rates of clinically relevant POPF vary widely, and only a minority of studies have systematically assessed postoperative functional outcomes. In this context, the present study adds incremental evidence by integrating perioperative outcomes with systematic assessment of both endocrine and exocrine pancreatic function, thereby addressing an important gap in the current literature.
Summary of published studies on minimally invasive function-preserving pancreatic surgery
| Author (year) | Country | Study design | No. of patients | Surgical approach | Type of procedure | Indication/pathology | Clinically relevant POPF | Functional outcomes reported |
| Fernández-Cruz et al. (2012)[26] | Spain | Retrospective single-center | 13 | Laparoscopic | EN | Non-functional pNETs | 23.1% | No |
| Peng et al. (2012)[27] | China | Case series | 4 | Robotic | DPPHR | Chronic pancreatitis or benign lesions | 75% | Yes |
| Senthilnathan et al. (2015)[28] | India | Retrospective single-center | 14 | Laparoscopic | CP | Benign/low-grade tumors | 21.4% | Yes |
| Jin et al. (2016)[29] | China | Retrospective comparative | 56 | Robotic vs. open | EN | Benign or borderline tumors | 38.7% | No |
| Jiang et al. (2018)[30] | China | Retrospective comparative | 34 | Robotic vs. open | DPPHR | Benign/pre-malignant disease | 32.4% | Yes |
| Cao et al. (2018)[31] | China | Retrospective single-center | 12 | Laparoscopic | DPPHR | Benign/low-grade tumors | 16.7% | No |
| Lin et al. (2021)[32] | China | Retrospective consecutive series | 61 | Robotic | SPDP | Benign/low-grade tumors | 9.8% | No |
| Esposito et al. (2020)[33] | Italy | Retrospective single-center | 34 | Robotic | SPDP | Benign/pre-malignant disease | 12.0% | No |
| Cai et al. (2020)[34] | China | Retrospective single-center | 24 | Laparoscopic | DPPHR | Benign/low-grade tumors | 4.2% | No |
| Zhou et al. (2022)[35] | China | Retrospective single-center | 30 | Laparoscopic | DPPHR | Benign/low-grade tumors | 6.7% | No |
| Lu et al. (2022)[36] | China | Retrospective single-center | 25 | Laparoscopic | DPPHR | Benign/low-grade tumors | 48% | Yes |
| Liu et al. (2022)[37] | China | Retrospective comparative | 12 | Laparoscopic | DPPHR | Pancreatic-head IPMN | 16.7% | Yes |
| Abu Hilalet al. (2023)[38] | Italy | Retrospective single-center | 50 | Robotic/laparoscopic | SPDP | Benign/low-grade tumors | 24% | No |
| Wu et al. (2024)[39] | China | Retrospective single-center | 151 | Laparoscopic | EN | Benign/low-grade tumors | 21.9% | No |
| Xiang et al. (2024)[40] | China | Retrospective single-center | 16 | Laparoscopic | CP | Benign/low-grade tumors | 31.3% | No |
| Murata et al. (2024)[41] | Japan | Retrospective comparative | 33 | Robotic vs. laparoscopic | SPDP | Benign/low-grade tumors | 24.2% | No |
| Liang et al. (2024)[42] | China | Case series | 10 | Laparoscopic | DPPHR | Benign/low-grade tumors | 30.0% | No |
| Zhou et al. (2025)[43] | China | Retrospective comparative | 131 | Robotic vs. laparoscopic | SPDP | Benign/low-grade tumors | 6.1% | No |
| Present study | China | Retrospective single-center | 39 | Robotic/laparoscopic | EN, CP, SPDP, DPPHR | Low-grade or benign lesions | 12.8% | Yes |
Several limitations of this study should be acknowledged. First, this was a retrospective, single-center study, which inevitably introduces selection bias and limits the generalizability of the findings. Second, the overall sample size was modest, and the cohort included heterogeneous pathological diagnoses, procedure types, and minimally invasive approaches, which restricted the ability to perform robust subgroup analyses and may have affected the interpretability of procedure-specific outcomes. Third, all operations were performed by a single experienced pancreatic surgeon. Although this ensured technical consistency and reduced inter-operator variability, it may also limit the extrapolation of our results to lower-volume centers or surgeons at an earlier stage of the learning curve. Fourth, pancreatic exocrine insufficiency was assessed primarily on the basis of clinical symptoms and the requirement for enzyme supplementation rather than standardized biochemical testing, which may have underestimated subclinical dysfunction. In addition, the follow-up duration was relatively short, precluding definitive assessment of long-term endocrine and exocrine durability as well as oncologic adequacy, particularly in patients with unexpected pathological findings. Furthermore, outcomes of other pancreatic procedures performed during the same period were not included for comparison, and this should be considered when interpreting the relative benefits of minimally invasive function-preserving surgery. These limitations suggest that the present findings should be interpreted cautiously and regarded mainly as descriptive evidence from a real-world institutional experience.
In conclusion, minimally invasive function-preserving pancreatic surgery appears to be a feasible and safe option for carefully selected patients with benign or low-grade pancreatic lesions, offering acceptable perioperative outcomes and preservation of pancreatic function when performed within a standardized framework by experienced surgeons. Further multicenter studies with larger cohorts, longer follow-up, and more standardized functional assessments are warranted to refine patient selection and clarify the long-term value of these parenchyma-sparing approaches.
DECLARATIONS
Authors’ contributions
Conceptualization, investigation, data analysis, writing - original draft, review, and editing: Wei P
Conceptualization, investigation, data acquisition, writing - original draft, review, and editing: Ni Y, Chen Z, Li X, Gao J
Conceptualization, supervision, funding acquisition, writing - review and editing: Li Z
All authors contributed to data interpretation, critically revised the manuscript for important intellectual content, and approved the final version of the manuscript.
Availability of data and materials
All data are available from the corresponding author upon reasonable request.
AI and AI-assisted tools statement
During the preparation of this manuscript, the AI tools ChatGPT (version GPT-5.1, released 2025-11-12) and Gemini (version Gemini 3 Flash, released 2025-12-17) were used solely for limited visual support in the preparation of the graphical abstract and Figure 2. The generated elements were subsequently substantially modified, redrawn, integrated, and finalized by the authors. These tools did not influence the study design, data collection, analysis, interpretation, or the scientific content of the work. All authors take full responsibility for the accuracy, integrity, and final content of the manuscript.
Financial support and sponsorship
The research was funded by the National Natural Science Foundation of China (Grant No. 82472662), the Beijing Municipal Natural Science Foundation (Grant No. L258067), and the Noncommunicable Chronic Diseases-National Science and Technology Major Project (Project No. 2023ZD0502003).
Conflicts of interest
Li Z is an Editorial Board Member of the journal Mini-invasive Surgery. Li Z was not involved in any stage of the editorial process, notably including reviewer selection, manuscript handling, or decision-making. The other authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
The study was approved by the Medical Ethics Committee of Peking University People’s Hospital (approval number: 2025PHB066-001) and was conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all patients.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Elliott IA, Epelboym I, Winner M, Allendorf JD, Haigh PI. Population-level incidence and predictors of surgically induced diabetes and exocrine insufficiency after partial pancreatic resection. Perm J. 2017;21:16-095.
2. Yu J, Sun R, Han X, Liu Z. New-onset diabetes mellitus after distal pancreatectomy: a systematic review and meta-analysis. J Laparoendosc Adv Surg Tech A. 2020;30:1215-22.
3. Kusakabe J, Anderson B, Liu J, et al. Long-term endocrine and exocrine insufficiency after pancreatectomy. J Gastrointest Surg. 2019;23:1604-13.
4. Li YQ, Pan SB, Yan SS, Jin ZD, Huang HJ, Sun LQ. Impact of parenchyma-preserving surgical methods on treating patients with solid pseudopapillary neoplasms: a retrospective study with a large sample size. World J Gastrointest Surg. 2022;14:174-84.
5. Zheng R, Ghabi E, He J. Robotic parenchymal-sparing pancreatectomy: a systematic review. Cancers. 2023;15:4369.
6. Rocca A, Scacchi A, Ceccarelli G. The impact of minimally invasive surgery and robot-assisted surgery on distal pancreatic resection: a snapshot on literature review and future technical innovations. Laparosc Surg. 2019;3:29-29.
7. Takahashi C, Shridhar R, Huston J, Meredith K. Outcomes associated with robotic approach to pancreatic resections. J Gastrointest Oncol. 2018;9:936-41.
8. Lefor AK. Robotic and laparoscopic surgery of the pancreas: an historical review. BMC Biomed Eng. 2019;1:2.
9. Cawich SO, Kluger MD, Francis W, et al. Review of minimally invasive pancreas surgery and opinion on its incorporation into low volume and resource poor centres. World J Gastrointest Surg. 2021;13:1122-35.
10. Teo RYA, Goh BKP. Surgical resection of pancreatic neuroendocrine neoplasm by minimally invasive surgery-the robotic approach? Gland Surg. 2018;7:1-11.
11. Roesel R, Bernardi L, Bonino MA, Popeskou SG, Garofalo F, Cristaudi A. Minimally-invasive versus open pancreatic enucleation: systematic review and metanalysis of short-term outcomes. HPB. 2023;25:603-13.
12. Miura T, Aoki S, Maeda S, et al. Laparoscopic enucleation vs. pancreatectomy for small pancreatic neuroendocrine neoplasms: long-term functional and oncological outcomes. Surg Endosc. 2025;39:7407-16.
13. Alzelfawi L, Almajed E, Alzabin A, et al. Prevention of postoperative pancreatic fistula: systematic review and meta-analysis. Surgeries. 2024;5:875-95.
14. Hajibandeh S, Hajibandeh S, Mowbray NG, et al. Minimally invasive versus open central pancreatectomy: a systematic review and meta-analysis. Ann Hepatobiliary Pancreat Surg. 2024;28:412-22.
15. Farrarons SS, van Bodegraven EA, Sauvanet A, Hilal MA, Besselink MG, Dokmak S. Minimally invasive versus open central pancreatectomy: systematic review and meta-analysis. Surgery. 2022;172:1490-501.
16. Jung D, Bari H, Hwang HK, Lee WJ, Kang CM. Short and long-term outcomes of minimally invasive central pancreatectomy: comparison with minimally invasive spleen-preserving subtotal distal pancreatectomy. Asian J Surg. 2023;46:824-8.
17. Beger HG, Mayer B, Poch B. Duodenum-preserving pancreatic head resection for benign and premalignant tumors-a systematic review and meta-analysis of surgery-associated morbidity. J Gastrointest Surg. 2023;27:2611-27.
18. Zu G, Chen W, Wu D, Zhang Y, Chen X. Clinical outcomes of minimally invasive duodenum-preserving pancreatic head resection. BMC Surg. 2023;23:288.
19. Choi M, Kang CM. Minimally invasive pancreatoduodenectomy for pancreatic cancer: current perspectives and future directions. Cancers. 2026;18:197.
20. Weksler Y, Lifshitz G, Avital S, Rudnicki Y. Robotic surgery for gastrointestinal malignancies-a review of how far have we come in pancreatic, gastric, liver, and colorectal cancer surgery. Cancers. 2025;17:3802.
21. Loiaco G, Rompianesi G, Giglio M, et al. Intraoperative celiac axis flow measurement and dynamic surgical strategies in robotic distal pancreatectomy. Mini-invasive Surg. 2025;9:9.
22. Riachi ME, Hewitt DB. Advances in pancreas surgery: robotic pancreaticoduodenectomy. Mini-invasive Surg. 2023;7:14.
23. Abu Hilal M, van Ramshorst TME, Boggi U, et al.; Collaborators. The Brescia Internationally Validated European Guidelines on Minimally Invasive Pancreatic Surgery (EGUMIPS). Ann Surg. 2024;279:45-57.
24. Sperti C, Beltrame V, Milanetto AC, Moro M, Pedrazzoli S. Parenchyma-sparing pancreatectomies for benign or border-line tumors of the pancreas. World J Gastrointest Oncol. 2010;2:272-81.
25. Li C, Yu Y, Guo W, et al. Laparoscopic enucleation: a safe and feasible treatment option for large (≥ 4 cm) benign or low-grade malignant pancreatic tumors. Front Med. 2025;12:1666758.
26. Fernández-Cruz L, Molina V, Vallejos R, Jiménez Chavarria E, López-Boado MA, Ferrer J. Outcome after laparoscopic enucleation for non-functional neuroendocrine pancreatic tumours. HPB. 2012;14:171-6.
27. Peng CH, Shen BY, Deng XX, Zhan Q, Han B, Li HW. Early experience for the robotic duodenum-preserving pancreatic head resection. World J Surg. 2012;36:1136-41.
28. Senthilnathan P, Gul SI, Gurumurthy SS, et al. Laparoscopic central pancreatectomy: our technique and long-term results in 14 patients. J Minim Access Surg. 2015;11:167-71.
29. Jin JB, Qin K, Li H, et al. Robotic enucleation for benign or borderline tumours of the pancreas: a retrospective analysis and comparison from a high-volume centre in Asia. World J Surg. 2016;40:3009-20.
30. Jiang Y, Jin JB, Zhan Q, Deng XX, Peng CH, Shen BY. Robot-assisted duodenum-preserving pancreatic head resection with pancreaticogastrostomy for benign or premalignant pancreatic head lesions: a single-centre experience. Int J Med Robot. 2018;14:e1903.
31. Cao J, Li GL, Wei JX, et al. Laparoscopic duodenum-preserving total pancreatic head resection: a novel surgical approach for benign or low-grade malignant tumors. Surg Endosc. 2018;33:633-8.
32. Lin X, Lin R, Lu F, et al. “Kimura-first” strategy for robotic spleen-preserving distal pancreatectomy: experiences from 61 consecutive cases in a single institution. Gland Surg. 2021;10:186-200.
33. Esposito A, Casetti L, De Pastena M, et al. Robotic spleen-preserving distal pancreatectomy: the Verona experience. Updates Surg. 2020;73:923-8.
34. Cai Y, Zheng Z, Gao P, Li Y, Peng B. Laparoscopic duodenum-preserving total pancreatic head resection using real-time indocyanine green fluorescence imaging. Surg Endosc. 2020;35:1355-61.
35. Zhou M, Xu S, Chao D, et al. Intracapsular approach used in laparoscopic duodenum-preserving total pancreatic head resection for pancreatic head benign or low-grade malignant tumors. Langenbecks Arch Surg. 2022;407:3851-8.
36. Lu C, Xu B, Mou Y, et al. Laparoscopic duodenum-preserving pancreatic head resection with real-time indocyanine green guidance of different dosage and timing: enhanced safety with visualized biliary duct and its long-term metabolic morbidity. Langenbecks Arch Surg. 2022;407:2823-32.
37. Liu W, Peng B. Laparoscopic duodenum-preserving total pancreatic-head resection versus standard pancreaticoduodenectomy for pancreatic-head intraductal papillary mucinous neoplasm. Asian J Surg. 2022;46:2293-8.
38. Abu Hilal M, Carvalho L, van Ramshorst TME, Ramera M. Minimally invasive vessel-preservation spleen preserving distal pancreatectomy-how I do it, tips and tricks and clinical results. Surg Endosc. 2023;37:7024-38.
39. Wu J, Guo W, Li C, et al. Laparoscopic enucleation of tumors embedded in the pancreatic head: safety and feasibility. Asian J Surg. 2024;48:267-73.
40. Xiang J, Zhu J, Wang H, Zhou X, Li H. Sixteen cases of laparoscopic central pancreatectomy for benign or low-grade malignant tumours in the pancreatic neck and proximal body. ANZ J Surg. 2024;94:888-93.
41. Murata Y, Noguchi D, Ito T, et al. Superiority of robotic over laparoscopic spleen-preserving distal pancreatectomy with warshaw procedure for reducing the incidence of postoperative splenic infarction. Surg Laparosc Endosc Percutan Tech. 2024;34:472-8.
42. Liang X, Gu Y, Chen Y, Liu Y, Wang S, Fu Y. Laparoscopic duodenum-preserving pancreatic head resection: a technique for the treatment of benign or low-grade malignant tumors (10 cases report). J Laparoendosc Adv Surg Tech A. 2024;34:135-40.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].