


Laparoscopic partial splenectomy for upper pole lesions key technical considerations
 0
0 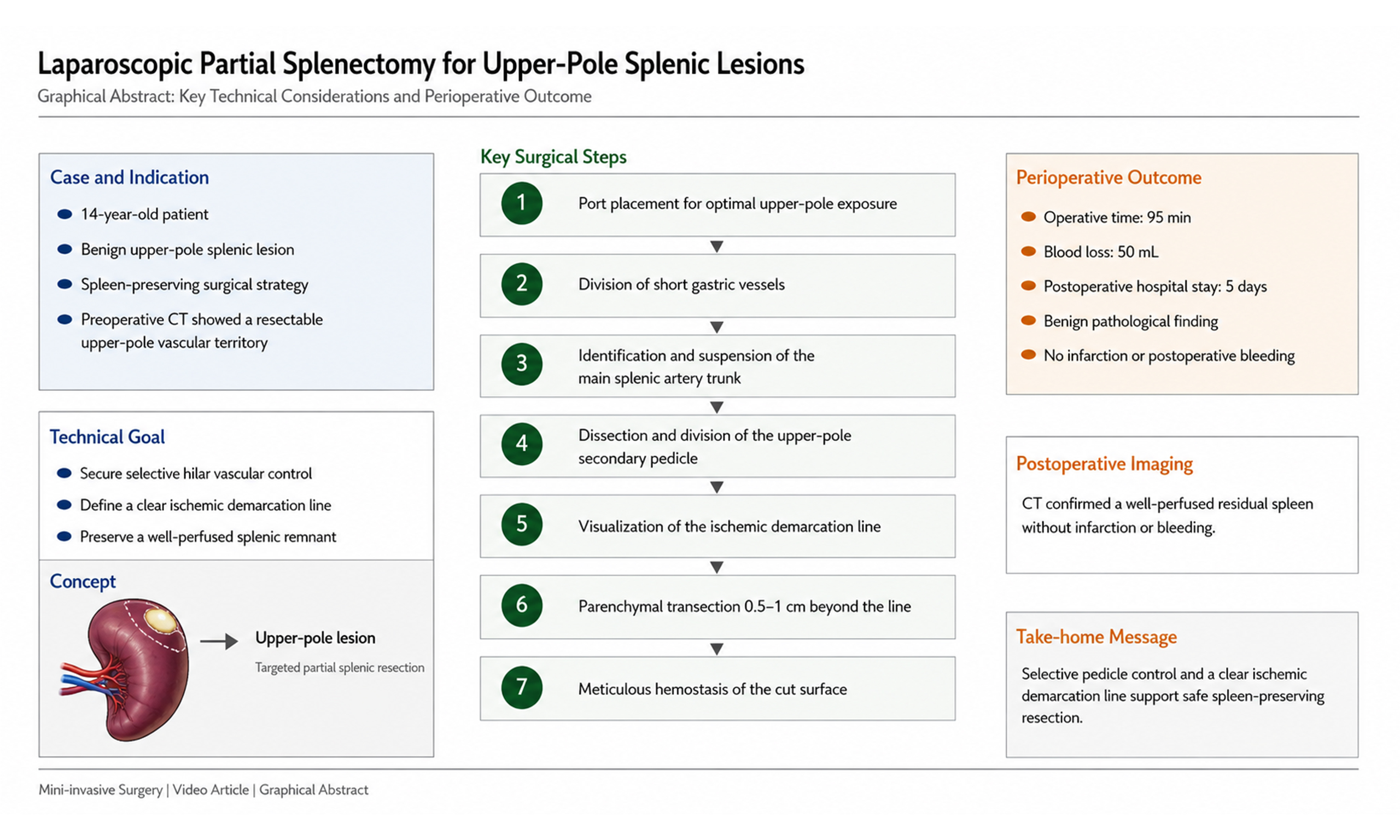
Watch a video of this article.
BRIEF EXPLANATION
Partial splenectomy is mainly indicated for benign splenic lesions and selected mild traumatic injuries when preservation of splenic immune function is desirable[1,2]. A 14-year-old patient with a benign upper pole splenic lesion underwent laparoscopic partial splenectomy. Preoperative enhanced computed tomography (CT) demonstrated an upper pole lesion with a resectable vascular territory. Laparoscopic partial splenectomy offers the advantages of splenic preservation, less surgical trauma, and faster postoperative recovery[3,4], but it also requires precise hilar vascular dissection and reliable control of the transection plane[5]. In selected complex cases, preoperative three-dimensional vascular reconstruction may help clarify hilar anatomy, and intraoperative ultrasound may be considered when lesion localization or the resection margin is uncertain[6,7].
Surgical technique
The port placement strategy is shown in Figure 1, and the key operative steps are shown in Figures 2-4 and Video 1. After division of the short gastric vessels within the gastrosplenic ligament, the main splenic artery trunk was identified along the superior pancreatic border and suspended with a silk suture for traction and vascular control. The secondary pedicular vessels supplying the splenic upper pole were then dissected and divided close to the splenic parenchyma en bloc [Figure 2A]. An ischemic demarcation line became evident, and the splenic parenchyma was transected 0.5-1 cm distal to this line using an electrocautery hook [Figure 2B]. Visible vessels on the cut surface were clipped or coagulated carefully, and low-temperature electrocoagulation was applied to achieve hemostasis while minimizing thermal injury [Figure 2C]. Only the ligaments adjacent to the resected segment were divided, whereas the remaining perisplenic ligaments were preserved whenever possible. Operative time was 95 min, blood loss was 50 mL, and the postoperative hospital stay was 5 days. Pathology confirmed a benign lesion [Figure 3], and postoperative CT demonstrated a well-perfused splenic remnant without infarction or bleeding [Figure 4].
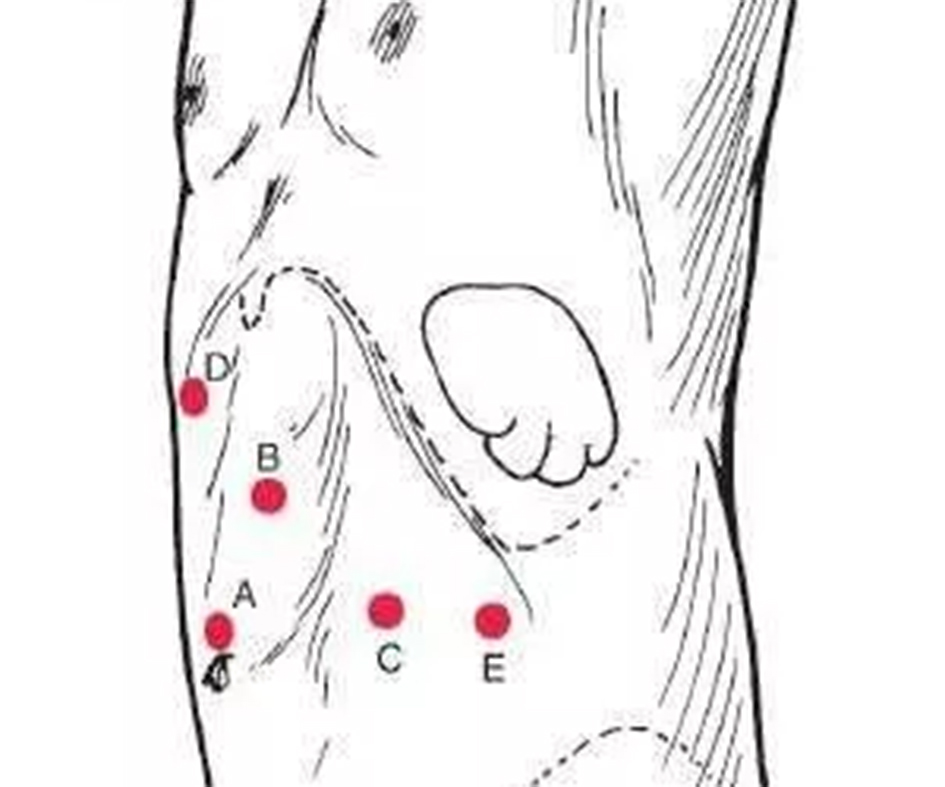
Figure 1. Port placement for laparoscopic partial splenectomy. A: Umbilical trocar; B, C, D, and E: operating trocars.

Figure 2. Key steps in vascular management and parenchymal transection. (A) Dissection of the secondary splenic pedicle; (B) Visualization of the splenic ischemic demarcation line; (C) Hemostasis of the splenic transection surface.
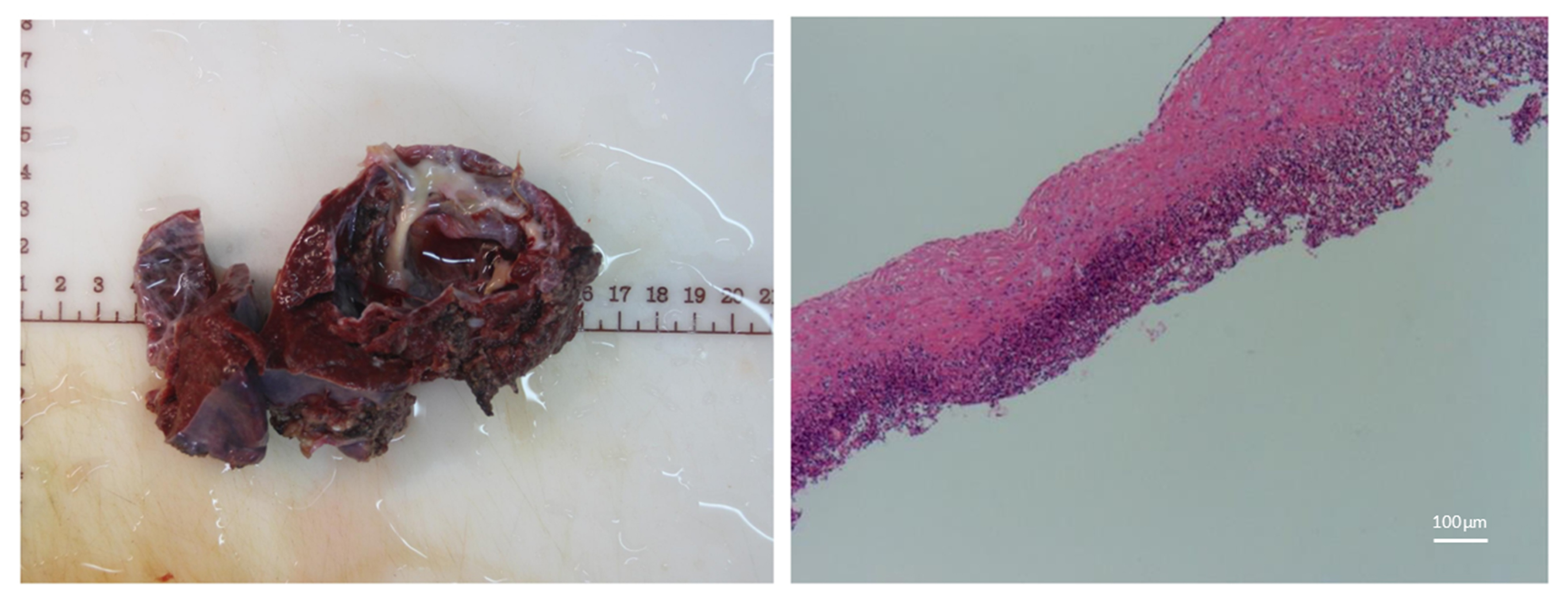
Figure 3. Postoperative pathological findings confirming a benign splenic lesion.
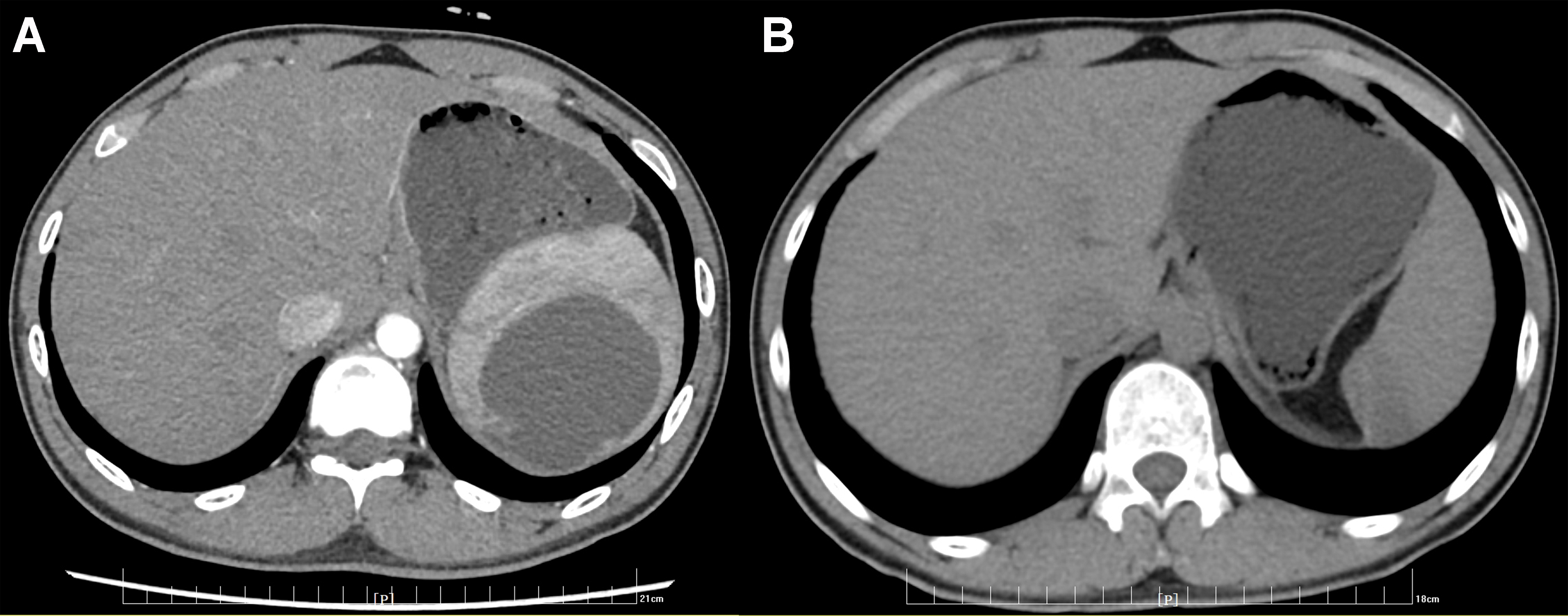
Figure 4. Abdominal computed tomography images. (A) Preoperative CT scan; (B) Postoperative CT scan demonstrating preservation of the residual spleen. CT: Computed tomography.
DECLARATIONS
Authors’ contributions
Conceptualization and manuscript drafting: Wei K, Du ZQ
Video preparation: Wei K, Geng XL
Manuscript revision and final approval: Du ZQ
Availability of data and materials
Not applicable.
AI and AI-assisted tools statement
Not applicable.
Financial support and sponsorship
None.
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
According to institutional policy, ethics committee approval was not required for this video article/case-based educational report. Informed consent was obtained from the patient.
Consent for publication
Written informed consent for publication of the video and related images was obtained from the patient’s legal guardian.
Copyright
© The Author(s) 2026.
Supplementary Materials
Please note: The publisher is not responsible for the content or functionality of any supporting information supplied by the authors. Any queries (other than missing content) should be directed to the corresponding author for the article.
REFERENCES
1. Li Y, Tian Y, Meng L, et al. The safety and feasibility of laparoscopic partial splenectomy: analysis of perioperative indications from different vascular subtypes and improvement of surgical approach. Surg Endosc. 2024;38:7329-40.
2. Xu J, Zhou W, He Q, Tao L. Laparoscopic partial splenectomy for traumatic splenic rupture patients is safe and feasible. Front Surg. 2025;12:1704119.
3. Lin J, Ou H, Liu Q, Ma J, Chen J, Wang W. Ten-year experience of laparoscopic partial splenectomy for patients with splenic benign lesions. Asian J Surg. 2025;48:245-9.
4. Xing D, Li P, Yang Y, Yao J. Retrospective assessment of the clinical efficacy of laparoscopic partial splenectomy. Exp Ther Med. 2023;25:210.
5. Ye T, Tan W, Qian D, Chen X, Zhao Z. Laparoscopic partial splenectomy with linear cutting stapler-assisted parenchymal transection: a novel technique. Ann Surg Oncol. 2025;32:7245-6.
6. Chen X, Jiang T, Peng Y, et al. Feasibility and outcomes of robot-assisted partial splenectomy for benign splenic lesions: a single-center experience. Front Surg. 2025;12:1726163.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].