


Trephination versus wide local excision for pilonidal disease: a propensity-matched study
 0
0 
Abstract
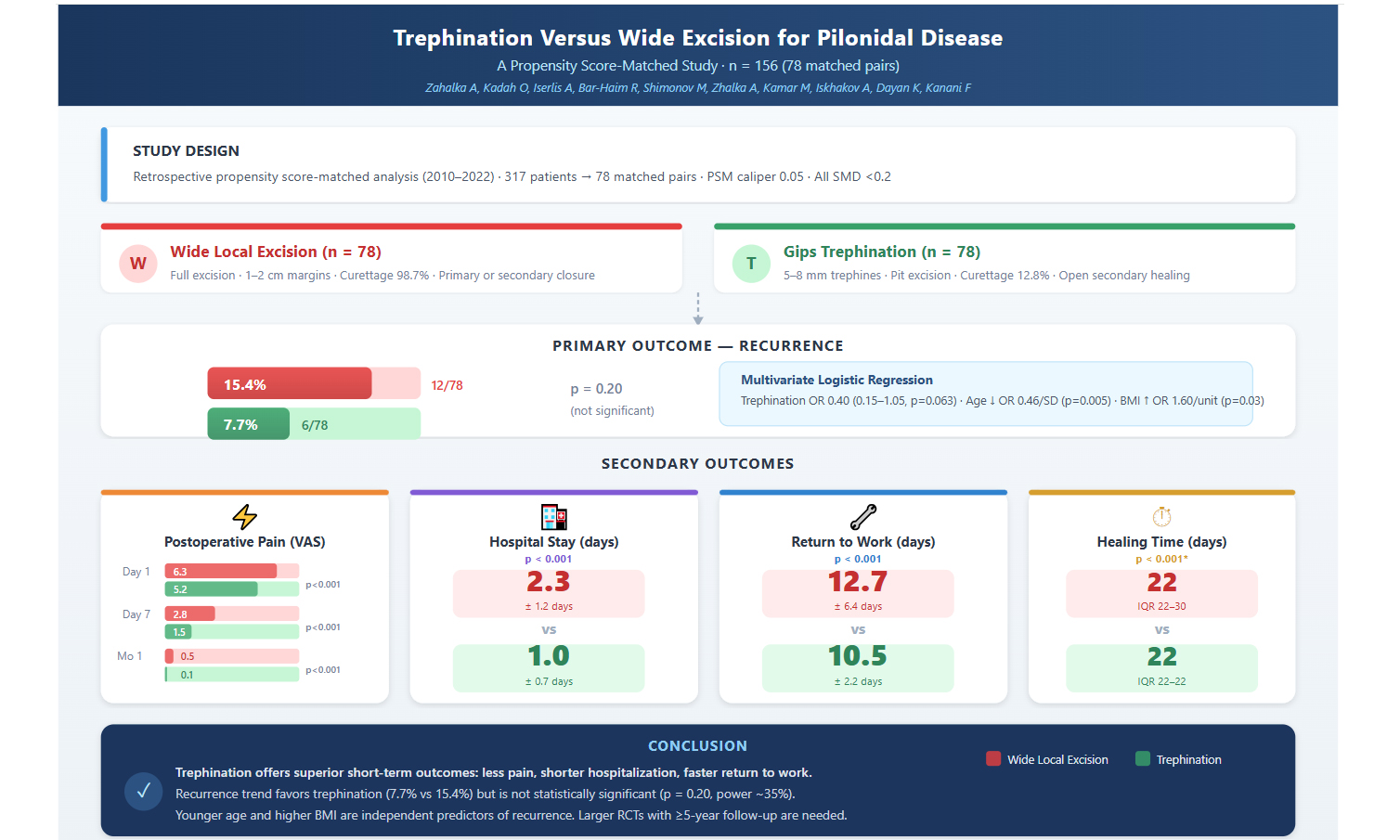
Aim: The optimal surgical technique for pilonidal sinus disease (PSD) remains controversial. This propensity score-matched study compared trephination with wide local excision to minimize selection bias.
Methods: We retrospectively analyzed 317 patients undergoing surgical treatment for PSD (2010-2022). Propensity score matching (1:1, caliper 0.05) using age, sex, body mass index (BMI), occupation, smoking, previous surgery, and symptom duration yielded 78 matched pairs. Primary outcome was recurrence; secondary outcomes included pain [Visual Analog Scale (VAS)], healing time, hospital stay, and return to work. Multivariate logistic regression identified recurrence predictors.
Results: After matching, groups were well-balanced [all standardized mean differences (SMDs) < 0.2]. Recurrence occurred in 15.4% of excision versus 7.7% of trephination patients (P = 0.20). Trephination demonstrated significantly lower pain scores at all timepoints: day 1 (5.2 ± 0.6 vs. 6.3 ± 1.7), day 7 (1.5 ± 1.1 vs. 2.8 ± 1.2), and month 1 (0.1 ± 0.2 vs. 0.5 ± 0.5; all P < 0.001). Hospital stay (1.0 ± 0.7 vs. 2.3 ± 1.2 days) and return to work (10.5 ± 2.2 vs. 12.7 ± 6.4 days) were shorter with trephination (both P < 0.001). Multivariate analysis identified younger age [odds ratio (OR) 0.46 per standard deviation (SD) increase of ~ 10-11 years; P = 0.005] and higher BMI (OR 1.60 per 1 kg/m2 increase; P = 0.03) as independent predictors of recurrence.
Conclusions: Trephination offers significant advantages in postoperative pain, hospital stay, and return to work compared to wide local excision, with a favorable but non-significant difference in recurrence. These findings support trephination when rapid recovery is prioritized. Larger trials are needed to establish long-term recurrence equivalence.
Keywords
INTRODUCTION
Pilonidal sinus disease (PSD) predominantly affects young adults aged 15-30 years with a male-to-female ratio of 3:1, causing significant quality-of-life impairment and socioeconomic burden[1-3]. Wide local excision (WLE) remains the traditional treatment, achieving cure rates of 80%-90% but with substantial morbidity including prolonged wound healing, hospitalization, and delayed return to activities[2,4-5], with outcomes varying further according to closure technique[6,7].
Interest in minimally invasive alternatives has grown considerably[8-11]. Among these, the Gips trephination technique, described in 2008, employs graduated trephines (2-9 mm) for systematic excision of sinus openings while preserving intervening tissue bridges[12,13]. Initial reports demonstrated 13.2% recurrence at five years with rapid recovery and minimal morbidity[13]. Di Castro et al. subsequently validated the technique in 2,347 patients[14].
However, recent high-quality evidence challenges this optimistic assessment. The 2023 meta-analysis by Amorim et al. of 4,286 patients reported time-dependent recurrence: 6.5% at two years, increasing to 38.9% beyond two years[15]. Similarly, Horesh et al.[16] and Khalilieh et al.[17] reported 32.9% one-year recurrence with trephination alone, reduced to 8.2% with laser adjunct therapy. These findings underscore the importance of longer follow-up and suggest that technological adjuncts may improve outcomes.
Nevertheless, advanced adjuncts remain unavailable in many healthcare settings worldwide where pilonidal disease is commonly treated. Understanding outcomes achievable with basic trephination technique is essential for resource-limited environments. Current comparative evidence suffers from heterogeneous techniques, variable follow-up duration, inconsistent outcome definitions, and inherent selection bias[12,18]. Controlled comparisons between Gips trephination and WLE using rigorous methodology remain lacking.
We performed a propensity score-matched analysis comparing Gips trephination with WLE, evaluating recurrence as the primary outcome and postoperative pain, healing time, hospital stay, and return to work as secondary outcomes. Our findings provide real-world evidence for surgical decision-making in settings without advanced technological adjuncts.
METHODS
Study design and patient selection
We conducted a retrospective analysis of patients who underwent surgical treatment for PSD at our secondary care center between January 2010 and December 2022. The institutional review board approved this study (Approval No. 0115-25-WOMC, 27 July 2025) and waived informed consent given its retrospective nature.
We included adults and adolescents aged 16-65 years presenting with PSD, diagnosed through clinical examination demonstrating characteristic sinus openings in the sacrococcygeal region. We required complete medical records and minimum 12-month follow-up. We excluded patients with extensive disease requiring flap reconstruction (defined as sinus networks extending > 5 cm laterally from midline or requiring Limberg, Karydakis, or V-Y advancement flaps), immunocompromised patients, and those with poorly controlled diabetes [hemoglobin A1c (HbA1c) > 9%]. Patient flow is detailed in Figure 1.
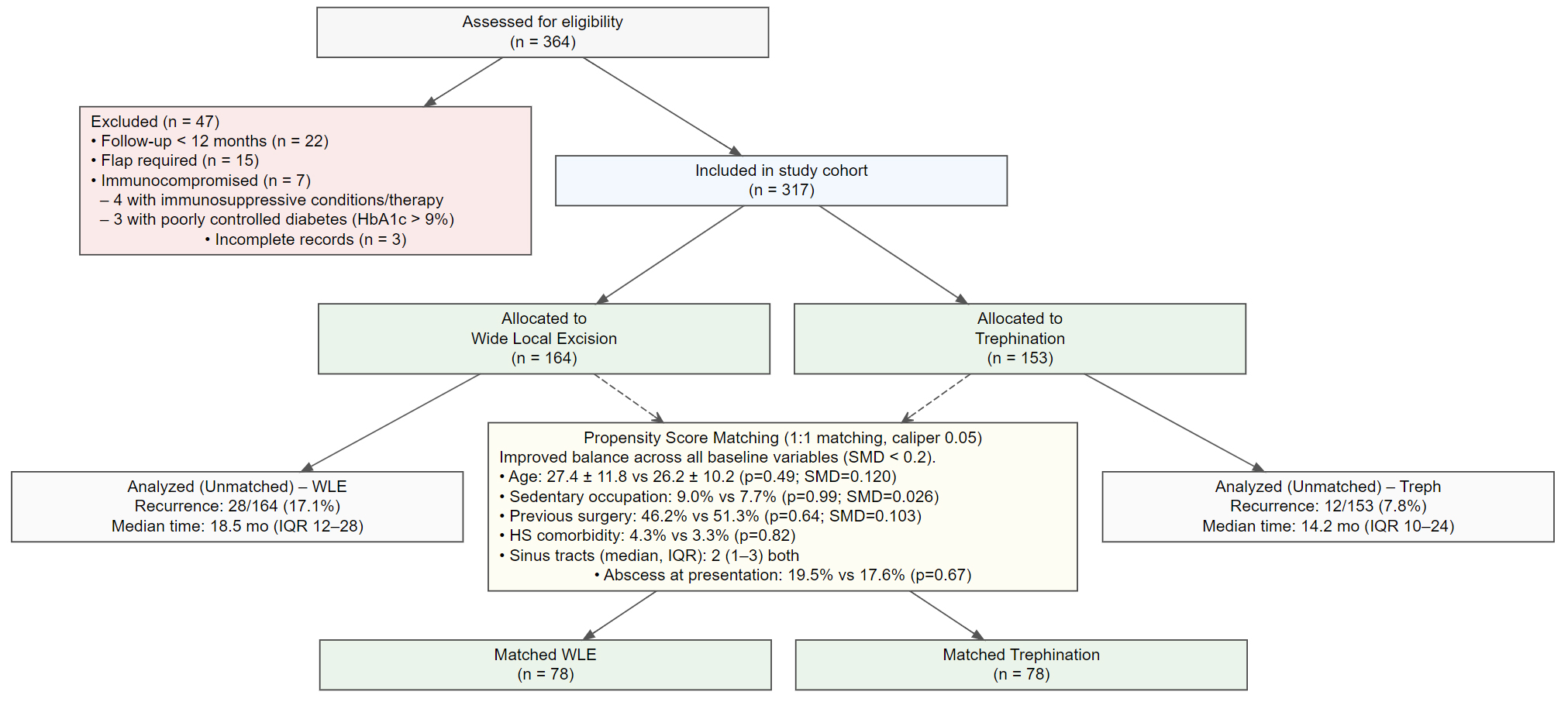
Figure 1. CONSORT flow diagram. HbA1c: hemoglobin A1c; WLE: wide local excision; SMD: standardized mean difference; IQR: interquartile range; CONSORT: Consolidated Standards of Reporting Trials.
Figure 1 illustrates patient inclusion, exclusion, treatment allocation, and matching. Of the 364 patients initially assessed for eligibility, 47 were excluded (22 due to follow-up < 12 months, 15 requiring flap reconstruction, 3 due to incomplete records, and 7 classified as immunocompromised - including 4 patients with immunosuppressive conditions or therapy and 3 patients with poorly controlled diabetes [HbA1c > 9%]). After exclusions, 317 patients were included: 164 underwent WLE and 153 underwent trephination. Propensity score matching (1:1, caliper 0.05) was performed using seven covariates: age, sex, body mass index (BMI), occupational type, smoking status, previous pilonidal surgery, and symptom duration. Following matching, 78 patients remained in each group with balanced baseline characteristics across all covariates (SMD < 0.2).
Surgical techniques [Figure 2]: All procedures were performed under general anesthesia with patients positioned prone and buttocks taped apart. Prophylactic antibiotics were administered based on surgeon preference. The choice between WLE and trephination evolved during the study period, with increasing adoption of trephination after 2020.
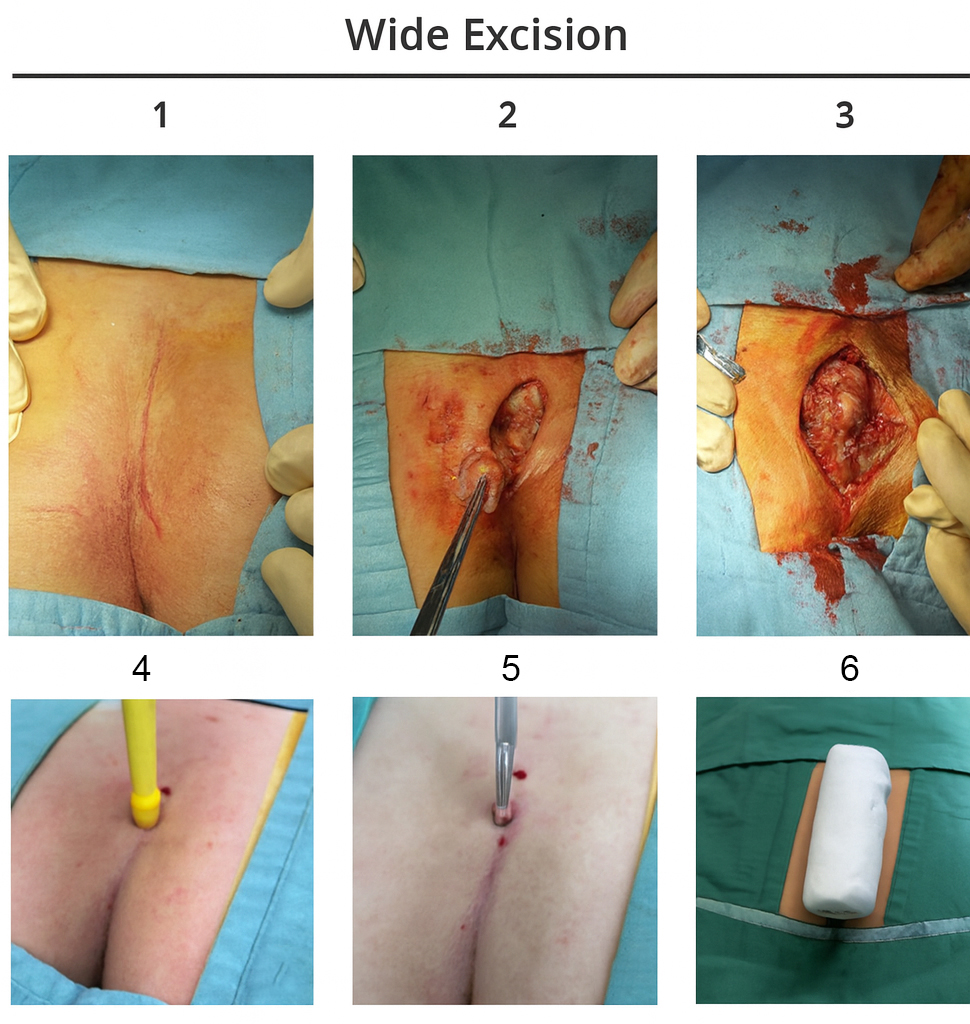
Figure 2. (1-3) Steps of wide local excision; (4-6) Trephine technique steps.
Wide local excision: Complete excision of all visible sinus tracts with 1-2 cm margins extending to presacral fascia. Formal surgical curettage was performed in 98.7% of cases. Wounds were closed primarily with interrupted mattress sutures or left open for secondary healing based on wound size and surgeon preference[19].
Gips trephination technique: Following the method described by Gips et al.[13], we performed systematic excision of all pilonidal openings using Keyes-type skin trephines (5-8 mm diameter). After identifying all pits with a probe, each opening was excised by advancing the trephine perpendicularly to skin, then aligning with tract direction. All patients underwent thorough cavity cleaning with hair and debris removal. Formal surgical curettage was possible in only 12.8% of cases where tract anatomy permitted adequate access. All trephination wounds were left open for secondary healing.
Data collection and outcome assessment
Baseline data included age, sex, BMI, occupational status (sedentary: sitting > 6 h/day; active: predominantly standing/walking), smoking status, symptom duration, and previous surgical interventions. Perioperative data included surgical technique, antibiotic use, operative time, and curettage performance. Missing data patterns are detailed in Supplementary Table 1.
Outcome definitions
Our primary outcome was recurrence, defined as clinical reappearance of PSD after initial treatment. Secondary outcomes included:
(1) Postoperative pain via Visual Analog Scale (VAS, 0-10) at baseline, day 1, day 7, and one month
(2) Healing time (days to complete wound epithelialization)
(3) Hospital length of stay
(4) Return to work (days until resuming regular activities without limitations)
(5) Patient satisfaction (10-point scale)
Follow-up assessments occurred at regular intervals. Recurrence status was determined for all patients through clinical record review. However, exact follow-up visit dates were incompletely documented in 30% of cases, limiting the precision of time-to-event analyses.
Statistical analysis
To address selection bias, we employed propensity score matching. The propensity score was derived using logistic regression incorporating age, sex, BMI, occupational type, smoking status, previous surgery, and symptom duration. We performed 1:1 nearest neighbor matching with caliper width of 0.05 standard deviations (SD) of the logit of the propensity score. Balance was assessed using standardized mean differences (SMDs), with values < 0.2 indicating adequate balance. Balance diagnostics are presented in Supplementary Table 2.
Statistical tests: Normality was assessed using the Shapiro-Wilk test. Between-group comparisons utilized independent t-tests for normally distributed continuous variables, Mann-Whitney U tests for non-normally distributed continuous variables (including healing time), and chi-square or Fisher’s exact tests for categorical variables. Continuous variables are reported as means with SDs for normally distributed data and medians with interquartile ranges (IQRs) for skewed distributions.
For time-to-event analysis, Kaplan-Meier curves illustrated recurrence-free survival with groups compared using log-rank test. Multivariate logistic regression identified independent predictors of recurrence; age was standardized (z-score) prior to model entry to facilitate interpretation as odds ratio (OR) per SD increase, while BMI was entered unstandardized (per unit increase in kg/m2).
Complete case analysis was performed for the primary outcome. Sensitivity analyses compared baseline characteristics between patients with complete versus incomplete documentation.
All analyses were performed using R version 4.5.0 (R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was defined as two-sided P < 0.05.
RESULTS
Study population and baseline characteristics before PSM
A total of 317 patients underwent surgical treatment for PSD during the study period, with 164 patients receiving WLE and 153 undergoing trephination. Before propensity score matching, significant baseline differences existed between the treatment groups [Table 1]. The mean age was 27.7 ± 11.6 years in the WLE group and 26.7 ± 10.2 years in the trephination group (P = 0.436). Male patients comprised 81.7% of the WLE group and 83.7% of the trephination group (P = 0.756). Mean BMI was 25.8 ± 3.9 kg/m² in the WLE group compared to 26.7 ± 3.4 kg/m2 in the trephination group (P = 0.026). Sedentary occupation was present in 3.7% of WLE patients versus 48.4% of trephination patients (P < 0.001, SMD = 1.184). Current smoking was reported by 32.3% of WLE patients and 19.0% of trephination patients (P = 0.010, SMD = 0.310). Noteworthy, before propensity score matching, recurrence occurred in 28/164 (17.1%) patients in the WLE group and 12/153 (7.8%) in the trephination group (P = 0.014). The median time to recurrence was 18.5 months (IQR 12-28) for WLE and 14.2 months (IQR 10-24) for trephination. Forty-seven patients (12.7% of the initial 364 eligible patients) were excluded [22 due to follow-up < 12 months, 15 requiring flap reconstruction, 3 due to incomplete records, and 7 classified as immunocompromised - including 4 patients with immunosuppressive conditions or therapy and 3 patients with poorly controlled diabetes (HbA1c > 9%)], as illustrated in Figure 1.
Baseline demographics and clinical characteristics before propensity score matching
| Characteristic | Wide local excision (n = 164) | Trephination (n = 153) | P-value | SMD |
| Demographics | ||||
| Age (years), mean ± SD | 27.7 ± 11.6 | 26.7 ± 10.2 | 0.436 | 0.088 |
| Male sex, n (%) | 134 (81.7) | 128 (83.7) | 0.756 | 0.052 |
| BMI (kg/m2), mean ± SD | 25.8 ± 3.9 | 26.7 ± 3.4 | 0.026 | 0.252 |
| Risk factors | ||||
| Sedentary occupation, n (%) | 6 (3.7) | 74 (48.4) | < 0.001 | 1.184 |
| Current smoker, n (%) | 53 (32.3) | 29 (19.0) | 0.010 | 0.310 |
| Disease characteristics | ||||
| Previous surgery, mean ± SD | 1 ± 0.49 | 1 ± 0.50 | - | 0.08 |
| Symptom duration (months), mean ± SD | 19.3 ± 38.3 | 25.5 ± 26.8 | 0.099 | 0.187 |
Study population and baseline characteristics after PSM
After 1:1 propensity score matching with a caliper of 0.05, 78 patients remained in each group [Table 2]. The matched cohorts showed improved balance across all baseline variables with SMD values less than 0.2. In the matched cohort, mean age was 27.4 ± 11.8 years for WLE and 26.2 ± 10.2 years for trephination (P = 0.49, SMD = 0.120). Sedentary occupation was present in 9.0% and 7.7%, respectively (P = 0.99, SMD = 0.026). Previous surgery rates were 46.2% in the WLE group and 51.3% in the trephination group (P = 0.64, SMD = 0.103). Clinical characteristics of the cohort included: hidradenitis suppurativa as a comorbidity in 12 patients (3.8%), with no significant difference between groups (4.3% vs. 3.3%, P = 0.82). The median number of sinus tracts was 2 (IQR 1-3) in both groups. Abscess at presentation was documented in 59 patients (18.6%), with similar rates between WLE (19.5%) and trephination (17.6%) groups (P = 0.67) [Figure 1].
Baseline demographics and clinical characteristics after propensity score matching
| Characteristic | Wide local excision (n = 78) | Trephination (n = 78) | P-value | SMD |
| Demographics | ||||
| Age (years), mean ± SD | 27.4 ± 11.8 | 26.2 ± 10.2 | 0.49 | 0.120 |
| Male sex, n (%) | 62 (79.5) | 65 (83.3) | 0.68 | 0.104 |
| BMI (kg/m2), mean ± SD | 26.5 ± 3.5 | 25.9 ± 3.8 | 0.31 | 0.176 |
| Risk factors | ||||
| Sedentary occupation, n (%) | 7 (9.0) | 6 (7.7) | 0.99 | 0.026 |
| Current smoker, n (%) | 18 (23.1) | 17 (21.8) | 0.99 | 0.033 |
| Disease characteristics | ||||
| Previous surgery, n (%) | 36 (46.2) | 40 (51.3) | 0.64 | 0.103 |
| Symptom duration (months), mean ± SD | 25.4 ± 26.8 | 25.2 ± 38.3 | 0.98 | 0.005 |
Operative characteristics
Operative details differed significantly between the two techniques [Table 3]. Curettage was performed in 98.7% of WLE procedures compared to 12.8% of trephination procedures (P < 0.001). All patients in both groups underwent surgery in prone position with general anesthesia. Intraoperative antibiotics were administered to 48.7% of WLE patients versus 7.7% of trephination patients (P < 0.001). Mean operative time was 22.7 ± 8.2 min for WLE and 33.6 ± 17.7 min for trephination (P < 0.001).
Operative and perioperative characteristics
| Variable | Wide local excision (n = 78) | Trephination (n = 78) | P-value |
| Operative details | |||
| Curettage performed, n (%) | 77 (98.7) | 10 (12.8) | < 0.001 |
| Intraoperative antibiotics, n (%) | 38 (48.7) | 6 (7.7) | < 0.001 |
| Operative time (min), mean ± SD | 22.7 ± 8.2 | 33.6 ± 17.7 | < 0.001 |
Postoperative pain outcomes
Pain assessment using the VAS demonstrated differences between groups at all time points [Table 4]. Baseline VAS scores were 1.0 ± 0.0 in both groups. On postoperative day 1, mean VAS scores were 6.3 ± 1.7 for WLE and 5.2 ± 0.6 for trephination (P < 0.001). At day 7, scores decreased to 2.8 ± 1.2 and 1.5 ± 1.1, respectively (P < 0.001). By one month, mean VAS scores were 0.5 ± 0.5 for WLE and 0.1 ± 0.2 for trephination (P < 0.001).
Postoperative pain outcomes
| Time point | Wide local excision (n = 78) | Trephination (n = 78) | Mean difference (95% CI) | P-value |
| Baseline VAS, mean ± SD | 1.0 ± 0.0 | 1.0 ± 0.0 | - | - |
| Day 1 VAS, mean ± SD | 6.3 ± 1.7 | 5.2 ± 0.6 | 1.1 (0.7-1.5) | < 0.001 |
| Day 7 VAS, mean ± SD | 2.8 ± 1.2 | 1.5 ± 1.1 | 1.3 (0.9-1.7) | < 0.001 |
| Month 1 VAS, mean ± SD | 0.5 ± 0.5 | 0.1 ± 0.2 | 0.4 (0.2-0.6) | < 0.001 |
Clinical outcomes and recovery
Primary and secondary outcomes showed differences between the surgical approaches [Table 5]. Recurrence occurred in 12 patients (15.4%) in the WLE group and six patients (7.7%) in the trephination group (P = 0.20). Median healing time was 22 days (IQR 22-30) for WLE and 22 days (IQR 22-22) for trephination (P < 0.001). Hospital stays averaged 2.3 ± 1.2 days for WLE versus 1 ± 0.7 days for trephination (P < 0.001). Return to work occurred at 12.7 ± 6.4 days and 10.5 ± 2.2 days respectively (P < 0.001). Patient satisfaction scores were 4.1 ± 3.4 for WLE and 4.3 ± 1.7 for trephination (P = 0.64). Median follow-up duration was 24.5 months (IQR 18-35) for WLE and 23.8 months (IQR 17-36) for trephination (P = 0.73).
Clinical outcomes and recovery parameters
| Outcome | Wide local excision (n = 78) | Trephination (n = 78) | P-value |
| Primary outcome | |||
| Recurrence, n (%) | 12 (15.4) | 6 (7.7) | 0.20 |
| Secondary outcomes | |||
| Healing time (days), median (IQR) | 22 (22-30) | 22 (22-22) | < 0.001 |
| Hospital stay (days), mean ± SD | 2.3 ± 1.2 | 1 ± 0.7 | < 0.001 |
| Return to work (days), mean ± SD | 12.7 ± 6.4 | 10.5 ± 2.2 | < 0.001 |
| Patient satisfaction (1-10), mean ± SD | 4.1 ± 3.4 | 4.3 ± 1.7 | 0.64 |
Multivariate analysis for recurrence
Multivariate logistic regression analysis identified predictors of recurrence [Table 6]. Trephination showed an OR of 0.40 (95% CI: 0.15-1.05, P = 0.063) compared to WLE. Age demonstrated a protective effect with OR 0.46 per SD increase (approximately 10-11 years; 95% CI 0.26-0.80, P = 0.005). BMI was associated with increased recurrence risk (OR 1.60 per 1 kg/m2 increase, 95% CI 1.04-2.45; P = 0.03). Male sex (OR 0.17, 95% CI 0.02-1.63, P = 0.12) and current smoking (OR 1.24, 95% CI 0.23-6.75, P = 0.80) were not significant predictors.
Multivariate logistic regression analysis for recurrence (n = 156)
| Variable | Odds ratio | 95% CI | P-value |
| Trephination (vs. Wide local excision) | 0.40 | 0.15-1.05 | 0.063 |
| Age (per SD increase, ~ 10-11 years) | 0.46 | 0.26-0.80 | 0.005 |
| Male sex | 0.17 | 0.02-1.63 | 0.12 |
| BMI (per unit increase) | 1.60 | 1.04-2.45 | 0.03 |
| Current smoker | 1.24 | 0.23-6.75 | 0.80 |
Recurrence-free survival analysis
Kaplan-Meier analysis demonstrated recurrence-free survival over the follow-up period [Figure 3]. The survival curves showed similar patterns between groups with no significant difference (log-rank test, P = 0.85). At 25 months, 62 patients in the WLE group and 60 in the trephination group remained at risk. By 50 months, nine and six patients remained at risk, respectively. The curves showed that most recurrences occurred within the first 50 months, with survival probabilities plateauing around 70% for both groups. Recurrence status was ascertained for all 156 matched patients. However, exact follow-up visit dates were incompletely documented in 30% of cases, limiting the precision of Kaplan-Meier survival estimates, which should be interpreted with caution. The recurrence rates reported (15.4% vs. 7.7%) remain valid as they reflect confirmed clinical outcomes regardless of timing precision.
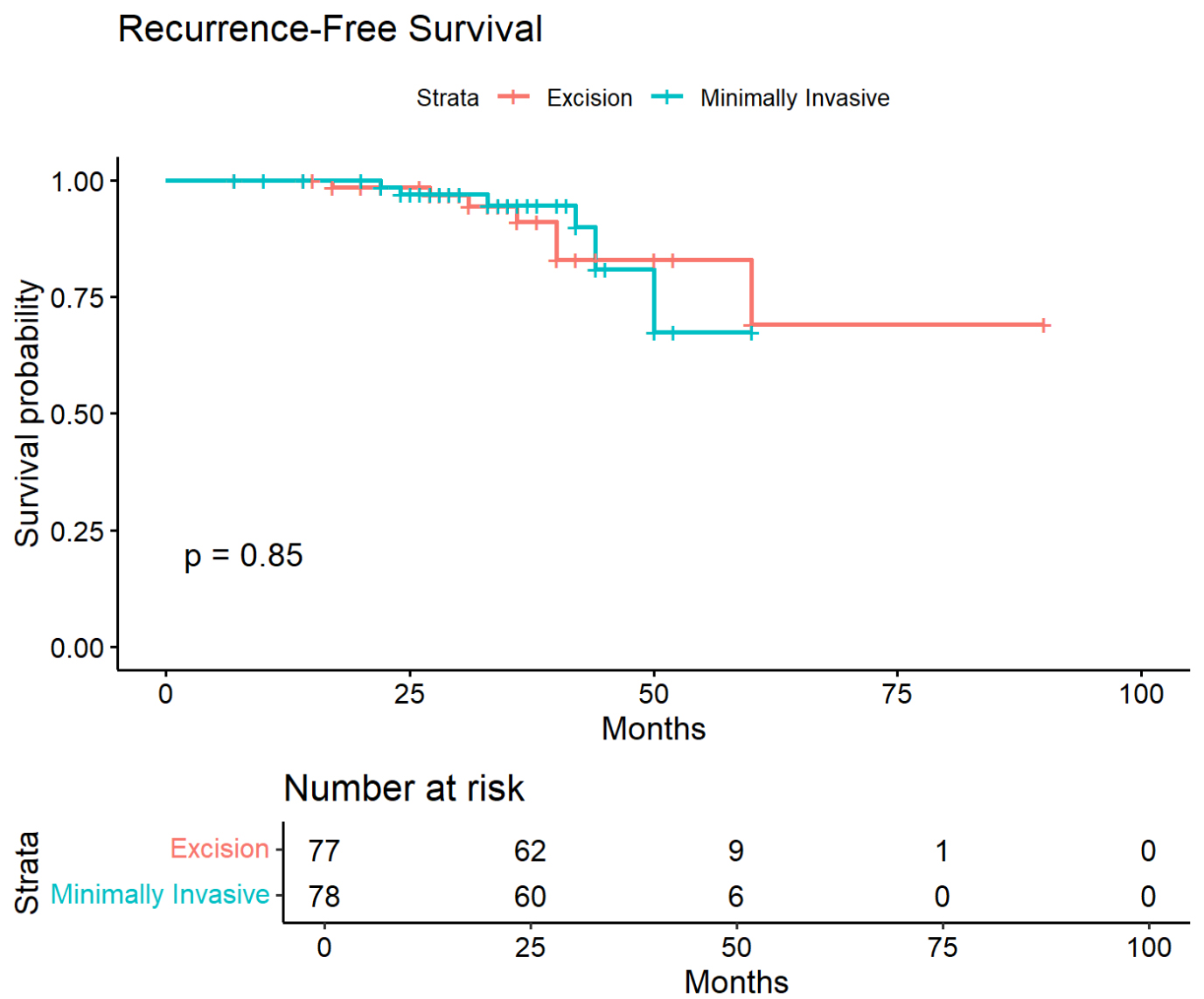
Figure 3. Kaplan-Meier recurrence-free survival curves. Comparison between wide local excision (blue) and trephination (red) groups. Groups compared using log-rank test (P = 0.85). Numbers at risk shown at 0, 25, 50, 75, and 100 months. Follow-up timing was incomplete in approximately 30% of patients; these curves should be interpreted with caution as imprecise timing data may affect survival estimates.
DISCUSSION
This propensity score-matched analysis revealed that the Gips trephination technique achieved significantly superior short-term outcomes compared to WLE, with reduced postoperative pain, shorter hospitalization, and faster functional recovery. However, these findings require careful contextualization within the evolving evidence base for minimally invasive pilonidal surgery.
The contemporary landscape of pilonidal surgery has shifted dramatically since the seminal 2008 report by Gips et al.[13]. Their initial series of 1,358 patients demonstrated seemingly acceptable recurrence rates of 13.2% at five years, establishing trephination as a viable minimally invasive alternative. However, recent high-quality evidence challenges this optimistic assessment. The comprehensive 2023 meta-analysis by Amorim et al., encompassing 4,286 patients across 13 studies, revealed a concerning temporal pattern: 2-year recurrence rates of 6.5% aligned with our observed 7.7%, increasing sharply to 38.9% beyond two years[15]. This time-dependent pattern has profound implications for surgical decision-making, particularly for young patients facing potential decades of disease risk.
Our findings align with other comparative studies demonstrating superior perioperative outcomes for minimally invasive techniques. The randomized trial by Milone et al. on video-assisted ablation reported a return to work at 1.6 days[20], while Pronk et al. documented 5.2 days for phenolization[21]. Our longer recovery time of 10.5 days likely reflects institutional factors including universal general anesthesia, mandatory overnight observation, and a patient population dominated by manual laborers requiring complete wound stability before resuming physical work.
The paradoxical finding of longer operative times for trephination (33.6 vs. 22.7 min) challenges conventional assumptions about minimally invasive surgery. Systematic identification and excision of multiple sinus openings through limited access points requires meticulous attention, whereas WLE provides immediate visualization of the entire disease complex. This technical complexity may partially explain variable outcomes reported across different centers.
Recent evidence highlights the potential for technological adjuncts to improve outcomes. A propensity-matched study by Horesh et al.[16], Algazar et al.[22] and Romic et al.[23] demonstrated that basic trephination yielded 32.9% recurrence at one year, substantially higher than our findings, yet decreased to 8.2% with laser adjunct therapy. While promising, such technology remains inaccessible in many global healthcare settings. Our study specifically addresses this gap by evaluating outcomes achievable with basic surgical instruments available universally. Younger age and higher BMI were identified as independent predictors of recurrence, consistent with established risk factors for pilonidal disease[24].
Limitations
This study has several limitations inherent to its retrospective design. First, the incomplete documentation of follow-up dates in 30% of patients represents a significant limitation for time-to-event analyses. Recurrence status was definitively ascertained for all patients. However, the precision of Kaplan-Meier survival estimates is compromised by incomplete data documentation, and patients with incomplete records may differ systematically from those with complete documentation.
Second, a critical limitation is the absence of disease severity parameters. Variables including sinus extent, tract complexity, number and depth of openings, lateral spread from midline, and prior abscess history were not systematically recorded in our retrospective database. These parameters typically guide surgical decision-making, and it cannot be excluded that patients selected for trephination represented a less complex disease subset. This potential selection bias may have favored trephination outcomes, and our findings should be interpreted accordingly. Future prospective studies should incorporate standardized disease severity classification systems to enable meaningful stratification.
Third, the temporal evolution of our surgical practice, with increased adoption of trephination after 2020, introduces potential confounding related to evolving surgical expertise, patient selection refinement, and period effects. Surgery year could not be included in the propensity score model without substantially reducing the matched cohort size, given the strong correlation between technique and time period.
Fourth, the small number of recurrence events (n = 18 in the matched cohort) substantially limits statistical power. Post-hoc analysis indicates approximately 35% power to detect the observed effect size at significance level alpha (α) =0.05. The non-significant trend favoring trephination (P = 0.20) may represent a Type II error, and larger multicenter studies are needed to definitively establish whether recurrence rates differ between techniques.
Fifth, the median follow-up of 24 months may underestimate true recurrence rates. Recent literature demonstrates that pilonidal recurrences can manifest beyond 5 years postoperatively, and longer surveillance periods are necessary to capture late events.
Sixth, patient satisfaction scores showed no significant difference between groups; however, these retrospectively collected self-reported measures are subject to recall bias and ceiling effects, limiting their interpretability. Similarly, the longer operative time observed with trephination reflects the technical demands of systematic pit identification and excision through limited access, rather than overall surgeon efficiency. Direct comparison with WLE - which addresses more extensive disease - requires cautious interpretation.
Finally, as a single-center study from a secondary care institution, generalizability to other settings, particularly tertiary referral centers managing more complex cases, may be limited.
Clinical implications and future directions
The clinical implications of our findings are nuanced. For patients prioritizing rapid recovery and minimal perioperative morbidity, trephination offers clear short-term advantages. Reductions in hospitalization and postoperative pain translate to meaningful quality-of-life benefits and reduced healthcare resource utilization. However, these benefits must be weighed against accumulating evidence of potentially high long-term recurrence rates, particularly beyond two years[15]. The potential need for reoperation in a substantial proportion of patients fundamentally alters the risk-benefit calculation for young patients.
Future research priorities should include prospective randomized trials with minimum five-year follow-up to definitively establish long-term recurrence rates. Standardized reporting of disease severity, technical variations, and patient-reported outcomes would facilitate meaningful cross-study comparisons. Investigation of risk stratification tools and hybrid approaches combining minimally invasive techniques with targeted adjuncts may identify optimal treatment algorithms.
In conclusion, while the Gips trephination technique demonstrates superior short-term outcomes compared to WLE, recent evidence of high late recurrence rates necessitates careful patient selection and counseling. Our findings support trephination as a reasonable option for patients prioritizing rapid recovery who accept potential reoperation risk. However, the concerning trajectory of time-dependent recurrence underscores the need for continued innovation in pilonidal surgery to achieve both minimal morbidity and durable cure.
DECLARATIONS
Acknowledgments
We thank the medical records department for assistance with data retrieval and the wound care nursing team for their meticulous documentation of healing outcomes.
Authors’ contributions
Conceptualization: Zahalka A, Shimonov M, Kanani F
Data curation: Kadah O, Zhalka A, Iskhakov A, Kanani F
Formal analysis: Kadah O, Iserlis A, Bar-Haim R, Iskhakov A, Dayan K, Kanani F
Investigation: Zahalka A, Kadah O, Bar-Haim R, Zhalka A, Dayan K, Kanani F
Methodology: Zahalka A, Kadah O, Iserlis A, Bar-Haim R, Zhalka A, Kamar M, Iskhakov A, Dayan K, Kanani F
Project administration: Shimonov M, Kanani F
Resources: Kanani F
Software: Kanani F
Supervision: Shimonov M, Kamar M, Dayan K, Kanani F
Validation: Kamar M, Kanani F
Visualization: Kanani F
Writing - original draft: Zahalka A, Kadah O, Iserlis A, Kanani F
Writing - review & editing: Zahalka A, Kanani F
All authors read and approved the final manuscript.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
AI and AI-assisted tools statement
Not applicable.
Financial support and sponsorship
Not applicable.
Conflicts of interest
The authors declare no competing interests.
Ethical approval and consent to participate
This study was conducted in accordance with the principles of the Declaration of Helsinki (1975, revised in 2013). Approval was obtained from the Wolfson Medical Center Institutional Review Board (IRB) prior to commencing the study (Approval No. 0115-25-WOMC, dated 27 July 2025). The requirement for informed consent was waived due to the retrospective nature of the study.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
Supplementary Materials
REFERENCES
1. Doll D, Luedi MM, Evers T, Kauf P, Matevossian E. Recurrence-free survival, but not surgical therapy per se, determines 583 patients’ long-term satisfaction following primary pilonidal sinus surgery. Int J Colorectal Dis. 2015;30:605-11.
2. Stauffer VK, Luedi MM, Kauf P, et al. Common surgical procedures in pilonidal sinus disease: a meta-analysis, merged data analysis, and comprehensive study on recurrence. Sci Rep. 2018;8:3058.
3. Grabowski J, Oyetunji TA, Goldin AB, et al. The management of pilonidal disease: a systematic review. J Pediatr Surg. 2019;54:2210-21.
4. Doll D, Orlik A, Maier K, et al. Impact of geography and surgical approach on recurrence in global pilonidal sinus disease. Sci Rep. 2019;9:15111.
5. Doll D, Matevossian E, Luedi MM, Schneider R, van Zypen D, Novotny A. Does full wound rupture following median pilonidal closure alter long-term recurrence rate? Med Princ Pract. 2015;24:571-7.
6. Sevinç B, Karahan Ö, Okuş A, Ay S, Aksoy N, Şimşek G. Randomized prospective comparison of midline and off-midline closure techniques in pilonidal sinus surgery. Surgery. 2016;159:749-54.
7. Enriquez-Navascues JM, Emparanza JI, Alkorta M, Placer C. Meta-analysis of randomized controlled trials comparing different techniques with primary closure for chronic pilonidal sinus. Tech Coloproctol. 2014;18:863-72.
8. Brown SR, Lund JN. The evidence base for pilonidal sinus surgery is the pits. Tech Coloproctol. 2019;23:1173-5.
9. Iesalnieks I, Ommer A, Herold A, Doll D. German national guideline on the management of pilonidal disease: update 2020. Langenbeck’s Arch Surg. 2021;406:2569-80.
10. Milone M, Basso L, Manigrasso M, et al. Consensus statement of the Italian society of colorectal surgery (SICCR): management and treatment of pilonidal disease. Tech Coloproctol. 2021;25:1269-80.
11. Emile SH, Elfeki H, Shalaby M, et al. Endoscopic pilonidal sinus treatment: a systematic review and meta-analysis. Surg Endosc. 2018;32:3754-62.
12. Johnson EK, Vogel JD, Cowan ML, Feingold DL, Steele SR. ; Clinical Practice Guidelines Committee of the American Society of Colon and Rectal Surgeons. The American society of colon and rectal surgeons’ clinical practice guidelines for the management of pilonidal disease. Dis Colon Rectum. 2019;62:146-57.
13. Gips M, Melki Y, Salem L, Weil R, Sulkes J. Minimal surgery for pilonidal disease using trephines: description of a new technique and long-term outcomes in 1,358 patients. Dis Colon Rectum. 2008;51. 1656-62; discussion 1662-3.
14. Di Castro A, Guerra F, Levi Sandri GB, Ettorre GM. Minimally invasive surgery for the treatment of pilonidal disease. The Gips procedure on 2347 patients. Int J Surg. 2016;36:201-5.
15. Amorim M, Estevão-Costa J, Santos C, Fernandes S, Fragoso AC. Minimally invasive surgery for pilonidal disease: outcomes of the Gips technique-A systematic review and meta-analysis. Surgery. 2023;174:480-6.
16. Horesh N, Maman R, Zager Y, et al. Surgical outcomes of minimally invasive trephine surgery for pilonidal sinus disease with and without laser therapy: a comparative study. Tech Coloproctol. 2023;28:13.
17. Khalilieh S, Horesh N, Cordoba M, et al. Surgical outcomes of minimally invasive trephine surgery for pilonidal sinus disease and risk factors for recurrence. J Laparoendosc Adv Surg Tech A. 2022;32:288-92.
18. Bi S, Sun K, Chen S, Gu J. Surgical procedures in the pilonidal sinus disease: a systematic review and network meta-analysis. Sci Rep. 2020;10:13720.
19. McCallum I, King PM, Bruce J. Healing by primary versus secondary intention after surgical treatment for pilonidal sinus. Cochrane Database Syst Rev. 2007:CD006213.
20. Milone M, Fernandez LM, Musella M, Milone F. Safety and efficacy of minimally invasive video-assisted ablation of pilonidal sinus: a randomized clinical trial. JAMA Surg. 2016;151:547-53.
21. Pronk AA, Smakman N, Furnee EJB. Short-term outcomes of radical excision vs. phenolisation of the sinus tract in primary sacrococcygeal pilonidal sinus disease: a randomized-controlled trial. Tech Coloproctol. 2019;23:665-73.
22. Algazar M, Zaitoun MA, Khalil OH, Abdalla WM. Sinus laser closure (SiLaC) versus Limberg flap in management of pilonidal disease: a short-term non-randomized comparative prospective study. Asian J Surg. 2022;45:179-83.
23. Romic I, Augustin G, Bogdanic B, Bruketa T, Moric T. Laser treatment of pilonidal disease: a systematic review. Lasers Med Sci. 2022;37:723-32.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].