


Single-port robotic management of distal ureteral pathologies: straightforward access
 0
0 
Abstract
Watch a video of this article.
BRIEF EXPLANATION
The Da Vinci Single-port (SP) system, utilizing a supine anterior retroperitoneal approach (SARA)[1], provides direct and minimally invasive access to the ureter through a 3.5 cm Gibson incision [Figure 1A and B]. Our video [Video 1] (All physicians appearing in the video have provided their informed consent for the use of their images) demonstrates the step-by-step management of three distinct distal ureteral conditions treated between January and June 2025.
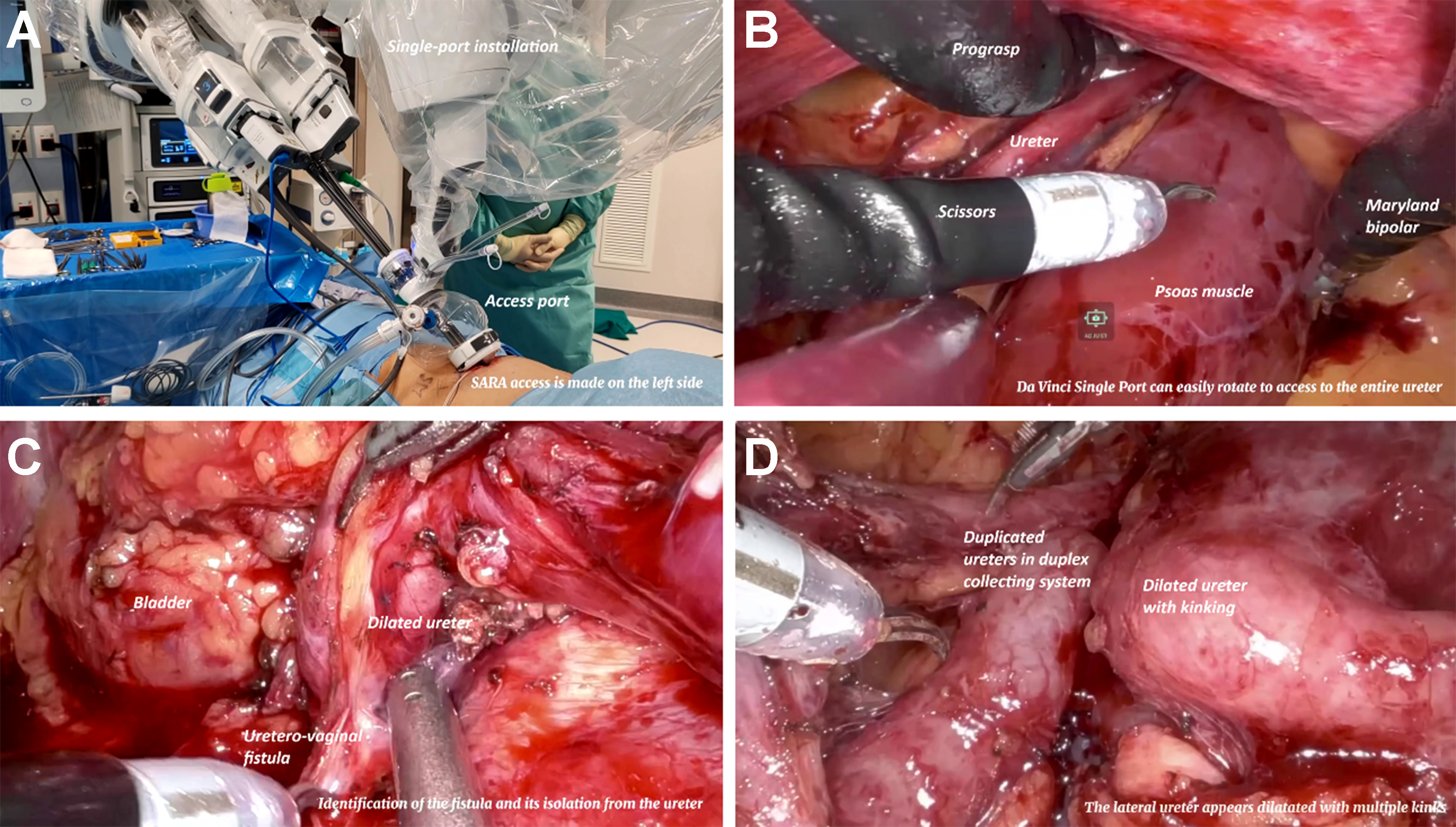
Figure 1. Straightforward access to the ureter with SP platform. (A) Docking of SP system; (B) Direct access to the ureter; (C) Hydronephrotic ureter stuck in inflammatory tissue; (D) Duplex collecting system with dilated ureters. SP: Single-port.
The first case involves a 43-year-old woman presenting with a left uretero-vaginal fistula, a complication of hysterectomy. The distal ureter was hydronephrotic and adhered to inflammatory tissue in communication with the vaginal cavity, causing continuous urine leakage [Figure 1C]. We performed direct ureteral reimplantation following meticulous dissection and closure of the fistulous tract.
The second case involves a left double ureterocutaneostomy in an 82-year-old woman with symptomatic complete left vesicoureteral reflux in a duplex collecting system [Figure 1D] and a low-compliance bladder. No space was left for reimplantation due to contractured bladder.
The third case describes a left distal ureterectomy and ipsilateral pelvic lymphadenectomy in a 76-year-old man with a 2-cm pTaG1 urothelial carcinoma. An extraperitoneal resection of the distal ureter and bladder cuff was performed, adhering strictly to oncological principles of urothelial carcinoma. Ureteral reimplantation was achieved using a small Boari flap to ensure a tension-free anastomosis. The flexibility of the SP platform facilitated the lymphadenectomy.
Detailed baseline and perioperative features for all three cases are presented in Table 1. All procedures were performed entirely within the retroperitoneum, allowing easier management of the ureter compared to extraperitoneal laparoscopic or multiport robotic approaches [Figure 1]. The SARA technique also offered anesthetic benefits, including improved pulmonary compliance for our patients, particularly those with obesity[1]. Our findings support the advantages of the SP-SARA approach compared to traditional transperitoneal access for treating distal ureteral pathologies. Furthermore, this technique may offer advantages such as shorter hospital stays, improved pain control, and superior cosmetic outcomes[2,3].
Baseline and perioperative features
| Case 1 | Case 2 | Case 3 | |
| Pathology | Iatrogenic left uretero-vaginal fistula | Left vesicoureteral reflux in duplex collecting system and low-compliance bladder | Left 2-cm distal ureter low-grade pTa urothelial carcinoma |
| Procedure | Left ureteral reimplantation | Left double ureterocutaneostomy | Left distal ureterectomy with ureteral reimplantation and pelvic lymphadenectomy |
| Age, years | 43 | 82 | 76 |
| Sex | Female | Female | Male |
| BMI | 25 | 29 | 22 |
| Total operative time (min) | 160 | 185 | 285 |
| Docking time (min) | 20 | 18 | 25 |
| Console time (min) | 110 | 130 | 230 |
| Blood loss (mL) | < 50 mL | < 50 mL | < 50 mL |
| Airseal use | Yes | Yes | Yes |
| Accessory trocar | Yes | No | Yes |
| 30-d complications | No | No | No |
| Postoperative opioid requirement for pain control | No | No | No |
| Time to return to bowel function (days) | 1 | 1 | 1 |
| Hospital stay (days) | 5 | 3 | 5 |
DECLARATIONS
Authors’ contributions
Conception and design of study: Oderda M, Gontero P
Data acquisition: Gontero P, Oderda M, Lavagno F
Video editing: Lavagno F
Manuscript writing: Oderda M
Supervision: Gontero P
Availability of data and materials
Anonymized clinical data are available upon request from the corresponding author.
AI and AI-assisted tools statement
Not applicable.
Financial support and sponsorship
None.
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
Informed consent was obtained from all subjects involved in the study.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
Supplementary Materials
Please note: The publisher is not responsible for the content or functionality of any supporting information supplied by the authors. Any queries (other than missing content) should be directed to the corresponding author for the article.
REFERENCES
1. Pellegrino AA, Chen G, Morgantini L, Calvo RS, Crivellaro S. Simplifying retroperitoneal robotic single-port surgery: novel supine anterior retroperitoneal access. Eur Urol. 2023;84:223-8.
2. Santarelli V, Valenzi FM, Haberal HB, et al. Current status of single port robotic‑assisted reconstructive urology: a systematic review, meta‑analysis and structured summary of the available literature. J Robot Surg. 2025;19:349.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Special Topic
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].