


fig12
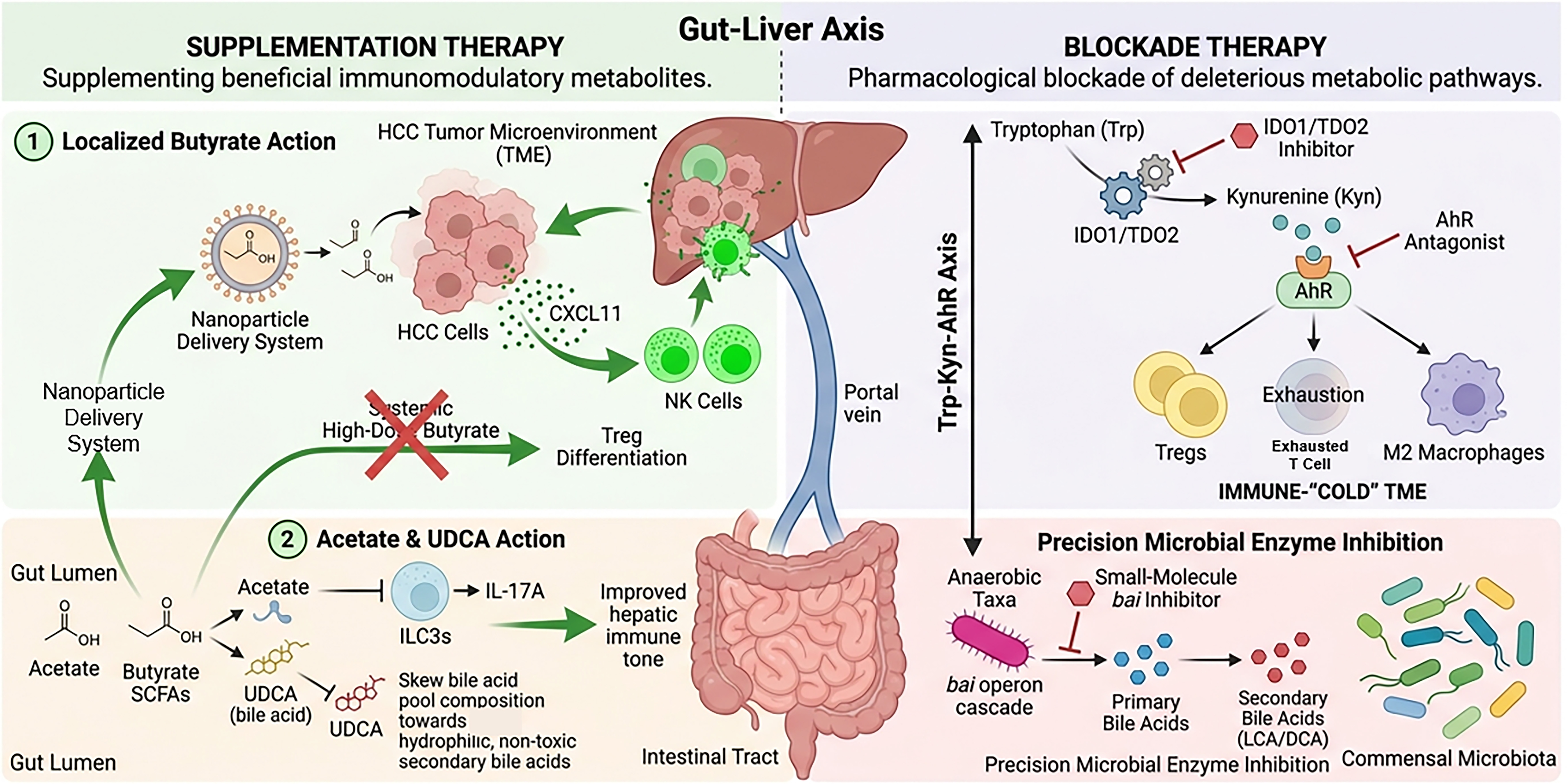
Figure 12. Microbiota-derived metabolite therapies for modulating the HCC immune microenvironment. The schematic illustrates two distinct pharmacological strategies. (Left) Supplementation Therapy: Localized delivery of butyrate (e.g., via nanoparticles) promotes CXCL11-mediated NK cell recruitment while avoiding systemic Treg induction. Acetate inhibits IL-17A production by ILC3s, and UDCA skews the bile acid pool toward non-toxic profiles. (Right) Blockade Therapy: Pharmacological interventions target the immunosuppressive Trp-Kyn-AhR axis using IDO1/TDO2 inhibitors or AhR antagonists. Furthermore, precision microbial enzyme inhibition targets specific bacterial operons (e.g., bai) to block the synthesis of pro-tumorigenic secondary bile acids without disrupting overall microbiota ecology. Detailed mechanisms are discussed in the corresponding text. HCC: Hepatocellular carcinoma; NK: natural killer; ILC3s: type 3 innate lymphoid cells; UDCA: ursodeoxycholic acid; IDO1: indoleamine 2,3-dioxygenase 1; AhR: aryl hydrocarbon receptor; TME: tumor microenvironment; SCFAs: short-chain fatty acids; LCA: lithocholic acid; DCA: deoxycholic acid; Tregs: regulatory T cells; CXCL11: C-X-C motif chemokine ligand 11; IL-17A: interleukin 17A; TDO2: tryptophan 2,3-dioxygenase.




