


Study on three-dimensional reconstruction-enhanced case-based learning for teaching nasal base depression to trainees
 0
0 Abstract
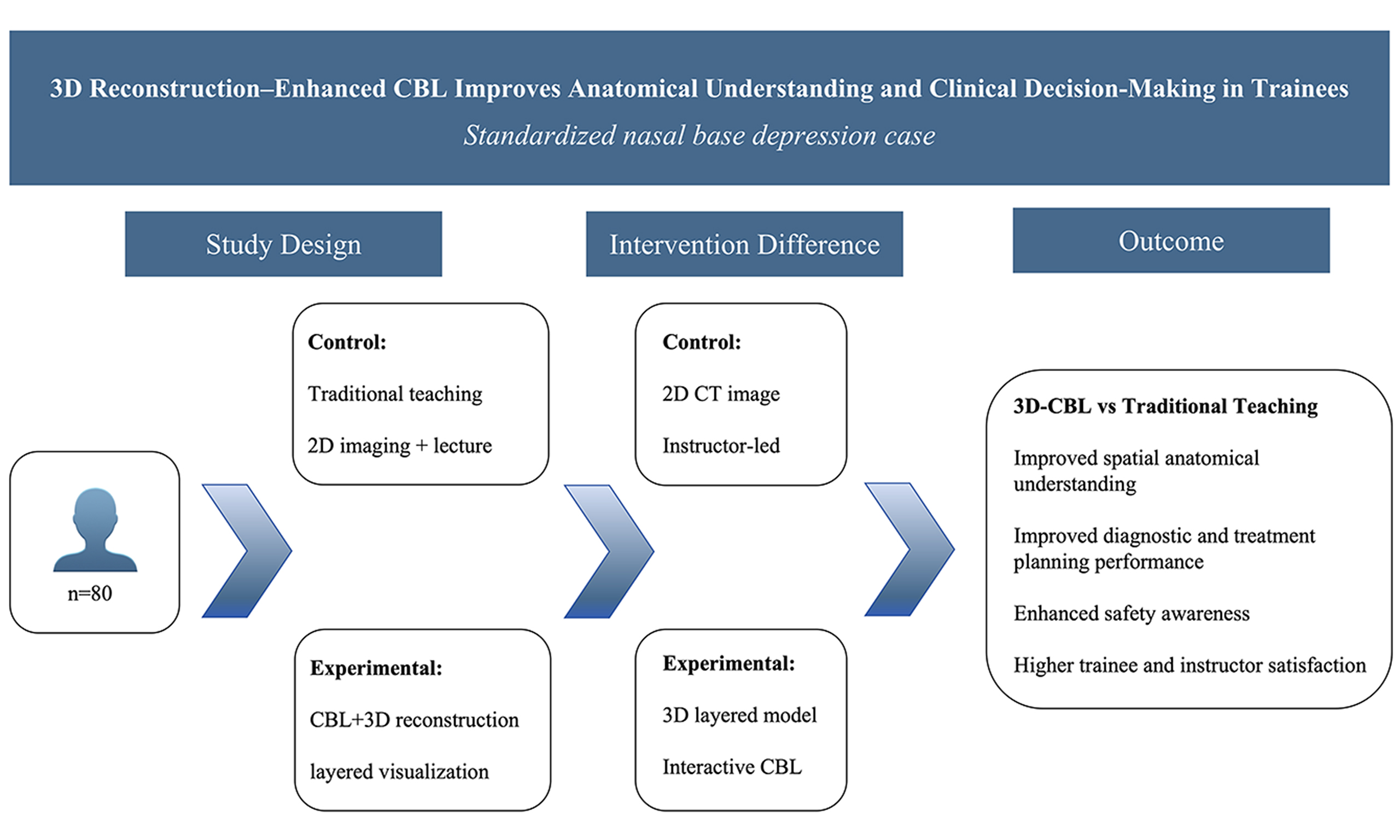
Aim: To evaluate the feasibility and preliminary educational impact of integrating case-based learning (CBL) with three-dimensional (3D) reconstruction in teaching nasal base depression to plastic and reconstructive surgery trainees, focusing on spatial anatomical cognition and clinical decision-making.
Methods: Eighty trainees from a tertiary academic hospital were randomly assigned to a traditional case-based instruction group or a 3D reconstruction-integrated CBL group. Both groups were instructed using a standardized nasal base depression case. The control group was taught using physical examination findings and two-dimensional images, whereas the experimental group additionally received a layered 3D reconstruction of skin-skeletal anatomy. Learning outcomes and satisfaction were assessed using self-assessment questionnaires and a structured in-class case-based assessment. Effect sizes were calculated to quantify between-group differences.
Results: Compared with the control group, the experimental group achieved significantly higher scores in understanding disease mechanisms, interpreting bone-soft tissue spatial relationships, and demonstrating proficiency in filler placement. Overall performance in the case-based diagnostic and treatment planning assessment was also superior in the experimental group, with large between-group effect sizes. In addition, satisfaction and perceived clinical relevance were higher in the experimental group.
Conclusion: The integration of CBL with 3D reconstruction was associated with improved spatial anatomical understanding and enhanced clinical decision-making within a standardized nasal base depression case model. These findings support the feasibility of this instructional approach and provide preliminary evidence for its application in anatomically complex domains of plastic and reconstructive surgery training.
Keywords
INTRODUCTION
Nasal base depression is a common, representative midfacial morphological abnormality, primarily resulting from insufficient bony support around the pyriform aperture, reduced soft tissue volume in the alar base region, and altered bone-soft tissue spatial relationships[1,2]. This region is adjacent to critical neurovascular structures, making it a high-risk anatomical area for facial filler procedures and rhinoplasty evaluation[3]. A precise understanding of its pathogenesis and deep anatomical structures is essential for aesthetic assessment and procedural safety. Accordingly, the development of robust three-dimensional (3D) spatial-anatomical cognition among trainees represents a key challenge in plastic and reconstructive surgery education.
Traditional medical education predominantly relies on lectures combined with two-dimensional imaging demonstrations[4,5]. Although effective for basic knowledge transmission, this approach may be insufficient in plastic surgery, where understanding complex spatial structures, bone-soft tissue relationships, and high-risk procedural skills is critical. In anatomically complex regions such as the nasal base, where layers are intricate and variable, reliance on surface observation and planar images may hinder the development of consistent 3D spatial cognition.
Since the inception of the residency training program over the past two decades, our department of plastic surgery has established a systematic continuing medical education framework. Previous surveys conducted by our team on residents trained between 2019 and 2023 revealed substantial variation in educational background, foundational training, and anatomical knowledge[6]. Although the current educational system has contributed to standardized training, gaps remain in the understanding of complex facial anatomy and the acquisition of skills for high-risk procedures. This underscores the need for educational strategies that better support spatial cognition and clinical reasoning.
Case-based learning (CBL) uses real clinical cases to guide discussion and problem-solving, promotes practical clinical skills and critical thinking, and has gained increasing attention in medical education[7,8]. Its application in anatomically complex regions may facilitate the translation of theoretical knowledge into clinical decision-making.
The 3D reconstruction enables layered visualization of skin, soft tissue, and skeletal structures, providing a more intuitive representation of complex facial anatomy[9]. Integrating 3D reconstruction into CBL may overcome the limitations of two-dimensional imaging and further reinforce trainees’ comprehension of bone-soft tissue relationships and safe procedural layers.
Against this background, the present study enrolled plastic surgery trainees at a tertiary hospital in Shanghai and used a standardized nasal base depression case in a controlled teaching design to evaluate the feasibility and preliminary educational impact of combining CBL with 3D reconstruction for improving spatial anatomical cognition and clinical decision-making. This study aimed to provide an initial empirical basis for refining instructional strategies in anatomically complex and high-risk domains of plastic surgery training.
METHODS
Participants
Eighty trainees undertaking advanced training in plastic and reconstructive surgery at a tertiary hospital in Shanghai were enrolled in this study. All participants had completed foundational training in anatomy and head and neck surgery and had not received structured training specifically in nasal base depression. Participants were randomly assigned to a control group or an experimental group (n = 40 each) using a random number table. Baseline characteristics, including age, professional rank, duration of training, and prior relevant clinical experience, were comparable between the two groups [Table 1]. A formal pretest to assess baseline knowledge of nasal base depression was not conducted, primarily due to time constraints and the feasibility-focused design of the instructional intervention. Randomization was implemented to minimize potential baseline imbalances in prior knowledge between groups.
Baseline characteristics of the participants in the control and experimental groups
| Variable | Control group (n = 40) | Experimental group (n = 40) | P value |
| Age (years) | 31.6 ± 3.8 | 32.1 ± 4.1 | 0.58 |
| Sex (male/female) | 22/18 | 21/19 | 0.82 |
| Prior facial injection experience (cases) | 4 (10%) | 3 (7.5%) | 0.69 |
Teaching case and materials
One patient with nasal base depression was selected as a standardized teaching case based on predefined instructional criteria. The inclusion criteria were clear radiological and clinical evidence of structural nasal base depression, the absence of prior injection or surgical intervention, and the concurrent involvement of bony deficiency, soft tissue imbalance, and altered bone-soft tissue spatial relationships. These characteristics ensured that the case incorporated multiple anatomical layers and considerations relevant to clinical decision-making within a single instructional scenario.
De-identified patient imaging data in Digital Imaging and Communications in Medicine (DICOM) format were used to generate 3D reconstruction models. Image processing and reconstruction were performed using Mimics Medical 21.0 (Materialise, Belgium). After data import, tissue segmentation was conducted based on Hounsfield unit (HU) thresholds to differentiate soft tissue and osseous structures. Separate masks were created for bone and soft tissue, followed by 3D reconstruction to generate a skin surface model, a skeletal model, and a combined skin-skeletal model. These models were subsequently used to facilitate layered anatomical instruction in the experimental group [Figure 1]. All imaging data were anonymized before analysis and educational application.
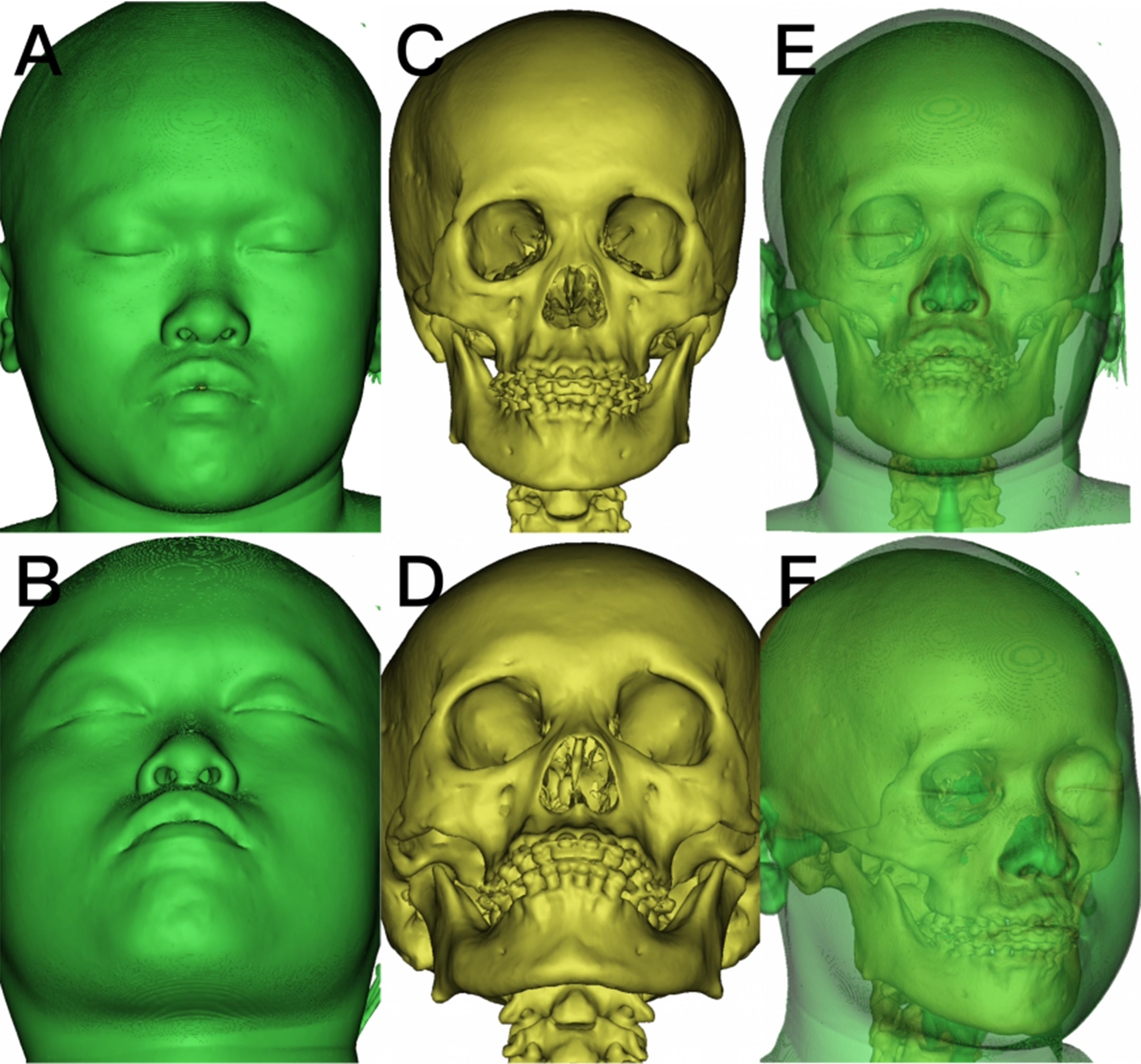
Figure 1. 3D reconstruction models used for layered teaching in the experimental group. (A and B) Frontal and upward-tilted views of the skin surface model; (C and D) Frontal and upward-tilted views of the skeletal model; (E and F) Frontal and lateral views of the combined skin-skeletal model. All models were generated using 3D reconstruction software to visualize the spatial relationships between soft tissue and bone for instructional purposes. All images are original and de-identified. 3D: Three-dimensional.
By using a standardized instructional case, this study design enabled a controlled comparison of teaching strategies and facilitated the evaluation of the feasibility and preliminary educational impact of integrating CBL with 3D reconstruction.
Design of the teaching procedure
The control group received traditional two-dimensional lecture-based case instruction, whereas the experimental group received CBL enhanced by 3D reconstruction, with standardized teaching objectives and identical instructional time. The teaching objectives were to: (1) develop a systematic understanding of the pathogenesis of nasal base depression; (2) understand the characteristics of relevant bony structures; (3) understand the soft tissue features of the nasal base region; and (4) identify safe filler layers and precise injection sites. All participants were exposed to the same standardized case to ensure consistency across groups. A participant flow diagram is shown in Figure 2.
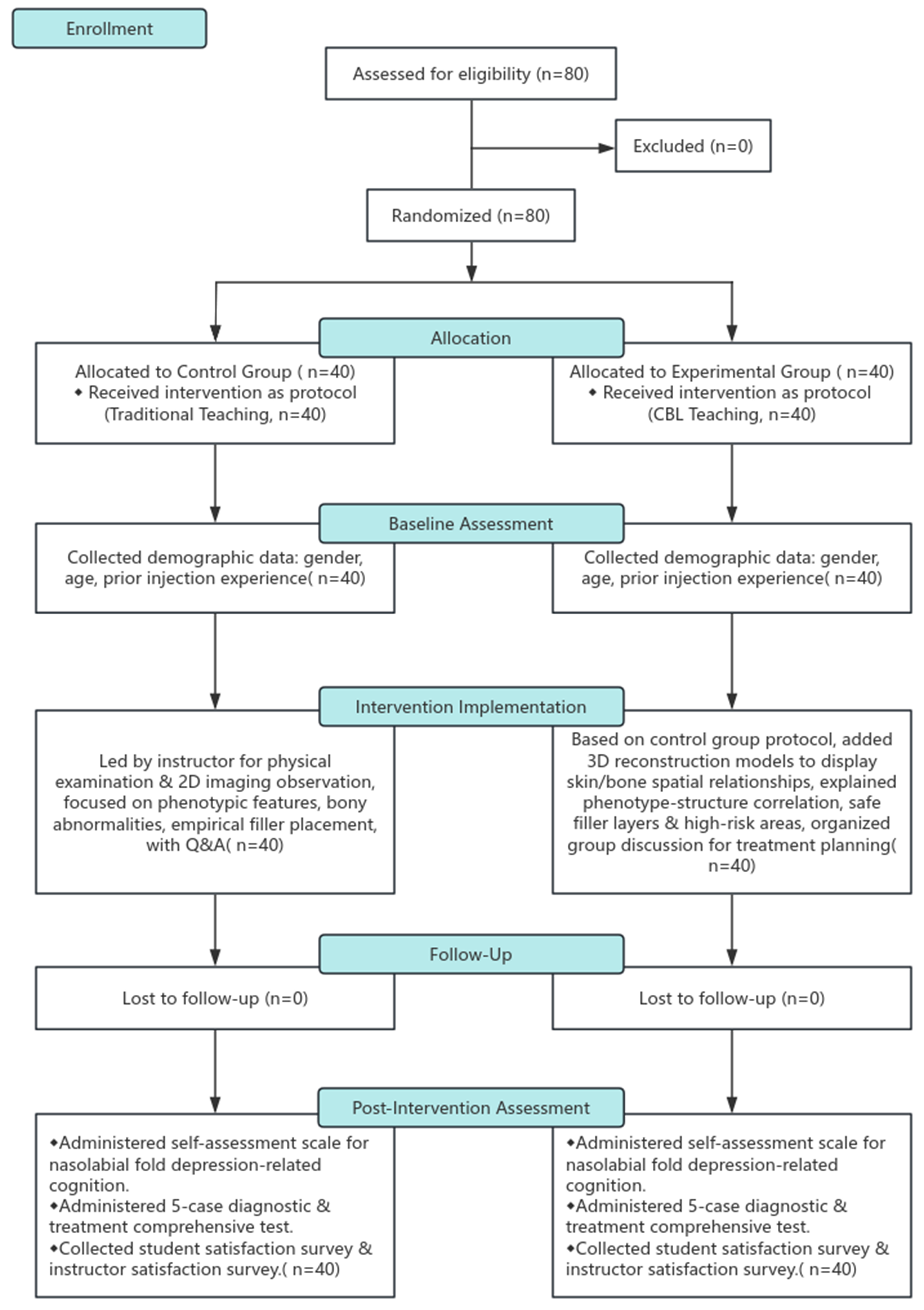
Figure 2. Teaching process flow diagram. The diagram summarizes the teaching process, including participant enrollment, random allocation to the control group (traditional instruction) or experimental group (CBL), baseline assessment, intervention implementation, follow-up, and post-intervention assessment. All participants provided informed consent, and the data were de-identified. 2D: Two-dimensional; 3D: three-dimensional; CBL: case-based learning; Q&A: questions and answers.
Teaching methods
Both groups received a standardized 60-min teaching session delivered separately by the same senior instructor to minimize instructor-related variability. The teaching objectives, instructional structure, subgroup size, discussion prompts, and assessment procedures were kept consistent between groups to ensure methodological comparability. The instructional design consisted of five sequential components.
Step 1. Case presentation (10 min)
A standardized case of nasal base depression was introduced using a de-identified clinical history, frontal and upward-tilted facial photographs, and relevant imaging data. Key clinical features were highlighted to establish an initial diagnostic framework.
Step 2. Anatomical analysis (15 min)
Control group:
Anatomical analysis was conducted using physical examination findings and two-dimensional computed tomography (CT) images. The instructor guided trainees in identifying structural deficiencies, soft tissue characteristics, and high-risk anatomical regions based on planar imaging. Instructor-led explanations served as the primary instructional approach[10].
Experimental group:
In addition to the instructional materials used in the control group, 3D reconstruction models were incorporated during this phase. Layered visualizations of the skin surface, skeletal, and combined skin-skeletal models were used to demonstrate spatial relationships. The models were rotated and viewed from multiple perspectives to facilitate a spatial understanding of bone-soft tissue relationships.
Step 3. Structured small-group discussion (15 min)
Participants were divided into subgroups of five trainees. Each subgroup addressed three predefined clinical questions:
What is the primary structural contributor to the deformity?
Which anatomical layers are appropriate and safe for filler placement?
What potential complications should be anticipated and avoided?
The instructor facilitated discussion using a standardized guide to ensure consistency in both questioning and analytical depth across groups.
Step 4. Independent treatment planning exercise (10 min)
Each trainee independently formulated a diagnostic conclusion and treatment plan on the basis of the case. Written responses were collected for subsequent evaluation.
Step 5. Summary and feedback (10 min)
The instructor provided structured feedback summarizing key anatomical insights, clinical reasoning processes, and safety considerations.
The two groups were instructed in separate sessions to prevent interaction or cross-group influence. Thus, the only experimental variable between groups was the mode of anatomical visualization during the analysis phase.
Evaluation of teaching effectiveness
Nasal base depression-related cognitive self-assessment questionnaire
Upon completion of the teaching session, participants completed a standardized self-assessment questionnaire [Supplementary Table 1] designed to evaluate their level of mastery of nasal base depression across five domains.
In-class case-based assessments
After the teaching session, participants were presented with five case-based questions requiring them to make diagnostic judgments and develop treatment plans. The case-based assessments were evaluated by a single senior instructor according to predefined scoring criteria encompassing diagnostic accuracy, the rationality of treatment plans, and procedural safety awareness. Each domain was scored on a scale of 0 to 100, with higher scores indicating better performance. The total score was calculated as the unweighted mean of the three domain scores, with equal weighting assigned to each component. To reduce potential assessment bias, all response sheets were anonymized and randomized prior to evaluation, and the evaluator was blinded to group allocation throughout the scoring process.
Trainee and instructor satisfaction assessment
Trainee satisfaction was measured with a five-point questionnaire: 1 = very dissatisfied, 2 = dissatisfied, 3 = neutral, 4 = satisfied, and 5 = very satisfied. The instructor’s evaluation of participants’ knowledge mastery was conducted using a five-point scale: 1 = not mastered, 2 = basic, 3 = familiar, 4 = proficient, and 5 = highly proficient. Higher scores indicated greater satisfaction or mastery. The mean scores were calculated for each domain and compared between groups.
Reliability assessment
To evaluate the internal consistency of the evaluation instruments, Cronbach’s α coefficients were calculated for the self-assessment questionnaire and the case-based assessment domains. Pearson correlation analysis was performed to examine the relationships among the three scoring domains of the case-based test.
Statistical analysis
Data were analyzed using SPSS version 24.0 (IBM Corp., Armonk, NY, USA). Continuous variables are presented as the mean ± standard deviation (SD) and compared between groups using independent-samples t-test. Categorical variables are presented as counts and percentages and were compared using chi-square tests. For the five domain-specific comparisons in the self-assessment questionnaire, the Bonferroni correction was applied to adjust for multiple comparisons. All tests were two-sided, and a P < 0.05 was considered statistically significant.
A post hoc power analysis was conducted for an independent-samples t-test (two-tailed, α = 0.05). With 80 participants (40 per group), the study had 80% power to detect a medium effect size (Cohen’s d ≈ 0.63).
RESULTS
Reliability analysis of the evaluation instruments
The self-assessment questionnaire demonstrated satisfactory internal consistency (Cronbach’s α = 0.819). Moderate correlations were observed among diagnostic accuracy, treatment plan rationality, and safety awareness (r = 0.423-0.638; P < 0.01). The internal consistency of the case-based assessment was acceptable (Cronbach’s α = 0.672), indicating overall coherence across multidimensional scoring domains.
Comparison of the nasal base depression-related cognitive self-assessments between groups
Significant between-group differences were observed in nasal base depression-related cognitive performance. Participants in the experimental group achieved higher scores across all five domains of the self-assessment questionnaire. After Bonferroni correction, all five domain differences remained statistically significant (adjusted P < 0.05) [Table 2]. The between-group difference corresponded to a large effect size (Cohen’s d = 3.52).
Self-assessment scores of the nasal base depression-related cognitive domains
| Evaluation domain | Control group (n = 40) | Experimental group (n = 40) | P value | Adjusted P value |
| Understanding of pathogenesis | 2.7 ± 0.58 | 3.3 ± 0.49 | 0.003 | 0.015 |
| Comprehension of bony structure characteristics | 2.5 ± 0.61 | 3.4 ± 0.50 | < 0.001 | 0.004 |
| Comprehension of soft tissue features | 2.6 ± 0.55 | 3.3 ± 0.52 | 0.002 | 0.010 |
| Interpretation of bone-soft tissue spatial relationships | 2.4 ± 0.62 | 3.5 ± 0.48 | < 0.001 | 0.003 |
| Proficiency in filler placement layers and locations | 2.4 ± 0.59 | 3.4 ± 0.51 | < 0.001 | 0.005 |
| Total score | 12.6 ± 1.32 | 16.9 ± 1.12 | < 0.05 |
Comparison of diagnostic and treatment planning performance between groups
Participants in the experimental group outperformed those in the control group in case diagnosis, filler-placement planning, and treatment strategy design, demonstrating greater safety awareness and risk avoidance. The total score was significantly higher in the experimental group (84.1 ± 6.2) than in the control group (70.4 ± 7.9) [Table 3]. The composite performance difference yielded a large effect size (Cohen’s d = 1.93).
Scores of diagnostic and treatment planning assessment
| Assessment item | Control group (n = 40) | Experimental group (n = 40) | P value |
| Diagnostic accuracy | 72.4 ± 8.6 | 82.9 ± 7.4 | < 0.05 |
| Treatment plan rationality | 70.1 ± 9.2 | 84.3 ± 6.8 | < 0.05 |
| Safety awareness and risk avoidance | 68.6 ± 8.9 | 85.6 ± 6.5 | < 0.05 |
| Total score | 70.4 ± 7.9 | 84.1 ± 6.2 | < 0.05 |
Comparison of trainee and instructor satisfaction between groups
Participants in the experimental group reported higher levels of trainee satisfaction, greater acceptance of the teaching method, and stronger recognition of its clinical value [Table 4]. Instructor satisfaction was also higher. All between-group differences were statistically significant. The overall difference in satisfaction corresponded to a large effect size (Cohen’s d = 3.31).
Trainee and instructor satisfaction scores
| Assessment item | Control group (n = 40) | Experimental group (n = 40) | P value |
| Overall trainee satisfaction | 3.6 ± 0.71 | 4.4 ± 0.53 | < 0.05 |
| Acceptance of teaching method | 3.3 ± 0.50 | 4.5 ± 0.49 | < 0.05 |
| Recognition of clinical instructional value | 3.5 ± 0.68 | 4.6 ± 0.50 | < 0.05 |
| Instructor satisfaction | 3.8 ± 0.65 | 4.5 ± 0.52 | < 0.05 |
| Total score | 3.55 ± 0.32 | 4.5 ± 0.26 | < 0.05 |
DISCUSSION
CBL promotes the integration of knowledge and the development of clinical reasoning through the use of authentic clinical scenarios and problem-oriented discussion[11,12]. Compared with traditional lecture-based teaching, CBL places greater emphasis on active learner participation and cognitive engagement and has been widely recognized as an effective approach for enhancing clinical analytical and decision-making skills[13,14]. In plastic and reconstructive surgery education, however, particularly in complex spatial anatomy and high-risk surgical regions, CBL alone may be insufficient due to the challenges of understanding intricate bone-soft tissue relationships[15]. Traditional two-dimensional imaging methods often fail to meet the spatial cognitive demands required in these high-risk anatomical areas.
Integrating 3D reconstruction into CBL can enhance trainees’ understanding of spatial relationships between bone and soft tissue, which is critical in complex anatomical regions such as the nasal base[16]. 3D reconstruction provides an intuitive, layered visualization of anatomical structures, enabling trainees to better understand the dynamic spatial interactions between soft tissues and the underlying skeletal framework. This combined approach may help overcome the limitations of traditional two-dimensional imaging, enhancing the understanding of bone-soft tissue relationships and facilitating safer procedural planning.
Although 3D reconstruction provides significant benefits, its broader implementation faces challenges, such as the need for technical support, additional instructional preparation, and specialized instructor expertise. The absence of a pretest also limited the ability to measure individual knowledge gains precisely. Future studies should address these constraints by incorporating pretest and posttest assessments and exploring the scalability of this teaching model across different anatomical regions.
The instructional intervention focused on a single standardized case of nasal base depression, which allowed for consistent exposure for all trainees within the limited session time. Although this approach reduced instructional variability and facilitated focused evaluation of 3D reconstruction within CBL, it may limit the generalizability of the findings to other nasal deformity patterns or more complex reconstructive scenarios. Future studies incorporating multiple case archetypes with varying anatomical complexity and spatial characteristics would enable a more comprehensive assessment of the scalability and applicability of this teaching model across a broader range of reconstructive training contexts.
The minimum detectable effect size (d ≈ 0.63) was smaller than the observed between-group differences, suggesting that insufficient statistical power was unlikely to explain the findings. The magnitude of the observed effect sizes may partly reflect the contrast between a structured 3D visualization approach and traditional didactic instruction within a focused anatomical domain. Although statistical significance was maintained after correction for multiple comparisons, the magnitude of the observed effect sizes should be interpreted with caution, particularly for subjective outcome measures, which may be prone to response bias and reduced variability. Nevertheless, replication across independent cohorts is warranted to confirm the stability of the observed differences.
Moderate internal consistency was observed across the assessment domains (α = 0.672), suggesting that diagnostic accuracy, treatment planning, and safety awareness, while related, are distinct aspects of clinical competence. Future research could enhance measurement precision by refining the scoring rubric and applying factor analysis approaches. Standardizing 3D model repositories and conducting multicenter studies would also enhance the generalizability of these findings.
The present findings further suggest that traditional lecture-based instruction may be insufficient for addressing complex spatial-anatomical relationships and high-risk procedural decision-making in plastic and reconstructive surgery education[17]. In a standardized nasal base depression case model, the integration of CBL with 3D reconstruction was associated with improved spatial-anatomical understanding, clinical decision-making performance, and safety awareness among trainees. These findings support the feasibility of this combined instructional strategy and provide preliminary evidence for its application in other complex areas of plastic surgery, such as breast reconstruction, facial defect repair, and craniofacial surgery, where 3D models can enhance spatial understanding and decision-making.
Several limitations must be considered when interpreting the results of this study. First, the study design did not include a pretest assessment, which may have contributed to potential knowledge biases between the control and experimental groups. A pre-post design would provide a more robust understanding of the educational impact. Second, the use of a single evaluator for performance-based assessments introduces the possibility of rater-related bias or expectancy effects. Third, the study relied on subjective outcome measures such as self-assessment and satisfaction scores, which are inherently prone to response bias and reduced variability. Finally, the study focused on a single anatomical region, limiting the generalizability of the findings to other areas of plastic surgery. Future studies should address these limitations by incorporating a pretest/posttest design, using multiple evaluators, and expanding the scope to other anatomical domains.
In conclusion, the integration of 3D reconstruction into CBL significantly enhanced trainees’ spatial anatomical understanding, diagnostic accuracy, and procedural planning in the context of nasal base depression. This combined instructional approach demonstrates strong feasibility and educational value for anatomically complex and high-risk regions.
DECLARATIONS
Acknowledgments
The authors would like to thank all the trainees who participated in this study for their cooperation and engagement. We also acknowledge the support of the teaching staff of the Department of Plastic and Reconstructive Surgery for their assistance in organizing and implementing the teaching sessions.
Authors’ contributions
Data acquisition, analysis, and interpretation: Zhou R
Literature review, manuscript drafting: Liu R
Manuscript planning, drafting: Wang C
Manuscript planning, drafting: Liang Y
Conceptualization, supervision: Wang D
All authors read and approved the final version.
Availability of data and materials
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
AI and AI-assisted tools statement
Not applicable.
Financial support and sponsorship
None.
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
This study was reviewed by the Ethics Committee of Shanghai Ninth People’s Hospital. In accordance with institutional policies, this study, which focused on an educational intervention and used fully anonymized data, was determined to be exempt from formal ethical approval. All the procedures were conducted in accordance with the relevant institutional guidelines and regulations. Written informed consent to participate was obtained from all participants prior to enrolment.
Consent for publication
Written informed consent for publication has been obtained for all patient images.
Copyright
© The Author(s) 2026.
Supplementary Materials
REFERENCES
1. Zhao R, Pan B, Li D, An Y. Application of paranasal augmentation rhinoplasty in asians with midfacial concavity. Ann Plast Surg. 2023;90:S147-52.
3. Xiang X, Wang X, Wang S. The treatment of alar base depression in rhinoplasty with diced autologous cartilage or mass cartilage: a systematic review. Aesthetic Plast Surg. 2024;48:3779-89.
4. Huang T, Zhou S, Wei Q, Ding C. Team-, case-, lecture- and evidence-based learning in medical postgraduates training. BMC Med Educ. 2024;24:675.
5. Jiang D, Huang D, Wan H, et al. Effect of integrated case-based and problem-based learning on clinical thinking skills of assistant general practitioner trainees: a randomized controlled trial. BMC Med Educ. 2025;25:62.
6. Zhou RP, Yu Y, Wang DR. Analysis of continuing medical education for advanced training physicians in plastic surgery at a Grade A tertiary hospital in Shanghai. J Tissue Eng Reconstr Surg. 2024;20:595-8. (in Chinese). Available from: https://www.qk.sjtu.edu.cn/jter/EN/lexeme/showArticleByLexeme.do?articleID=49102. [Last accessed on 19 May 2026].
7. Aguayo S, Benso B, Cantarutti C, Ortuño D, Véliz C. Case-based learning to teach scientific thinking to dental students. J Dent Educ. 2022;86:1734-6.
8. Zhang SL, Ren SJ, Zhu DM, et al. Which novel teaching strategy is most recommended in medical education? BMC Med Educ. 2024;24:1342.
9. Surek CC, Moorefield A. Deep plane anatomy for the facelift surgeon: a comprehensive three-dimensional journey. Facial Plast Surg Clin North Am. 2022;30:205-14.
10. Zhao W, He L, Deng W, Zhu J, Su A, Zhang Y. The effectiveness of the combined problem-based learning (PBL) and case-based learning (CBL) teaching method in the clinical practical teaching of thyroid disease. BMC Med Educ. 2020;20:381.
11. Burgess A, Matar E, Roberts C, et al. Scaffolding medical student knowledge and skills: team-based learning (TBL) and case-based learning (CBL). BMC Med Educ. 2021;21:238.
12. Zhao J, Gong X, Ding J, et al. Integration of case-based learning and three-dimensional printing for tetralogy of fallot instruction in clinical medical undergraduates: a randomized controlled trial. BMC Med Educ. 2024;24:571.
13. Yu Z, Zhao Z, Chen X, et al. Effects of standardised patients (SP) combined with case-based learning (CBL) in Chinese clinical education: a systematic review and meta-analysis. BMJ Open. 2025;15:e095705.
14. Cen XY, Hua Y, Niu S, Yu T. Application of case-based learning in medical student education: a meta-analysis. Eur Rev Med Pharmacol Sci. 2021;25:3173-81.
15. Brito ÍM, Avashia Y, Rohrich RJ. Evidence-based nasal analysis for rhinoplasty: the 10-7-5 method. Plast Reconstr Surg Glob Open. 2020;8:e2632.
16. Sulena S, Kapoor A, Kulkarni A, et al. Curriculum innovation: integrating case-based learning with seminar and journal club to enhance critical thinking skills in residency program. Neurol Educ. 2025;4:e200213.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].