


Reconstructing the nasal septum in rhinoplasty surgery
 0
0 
Abstract
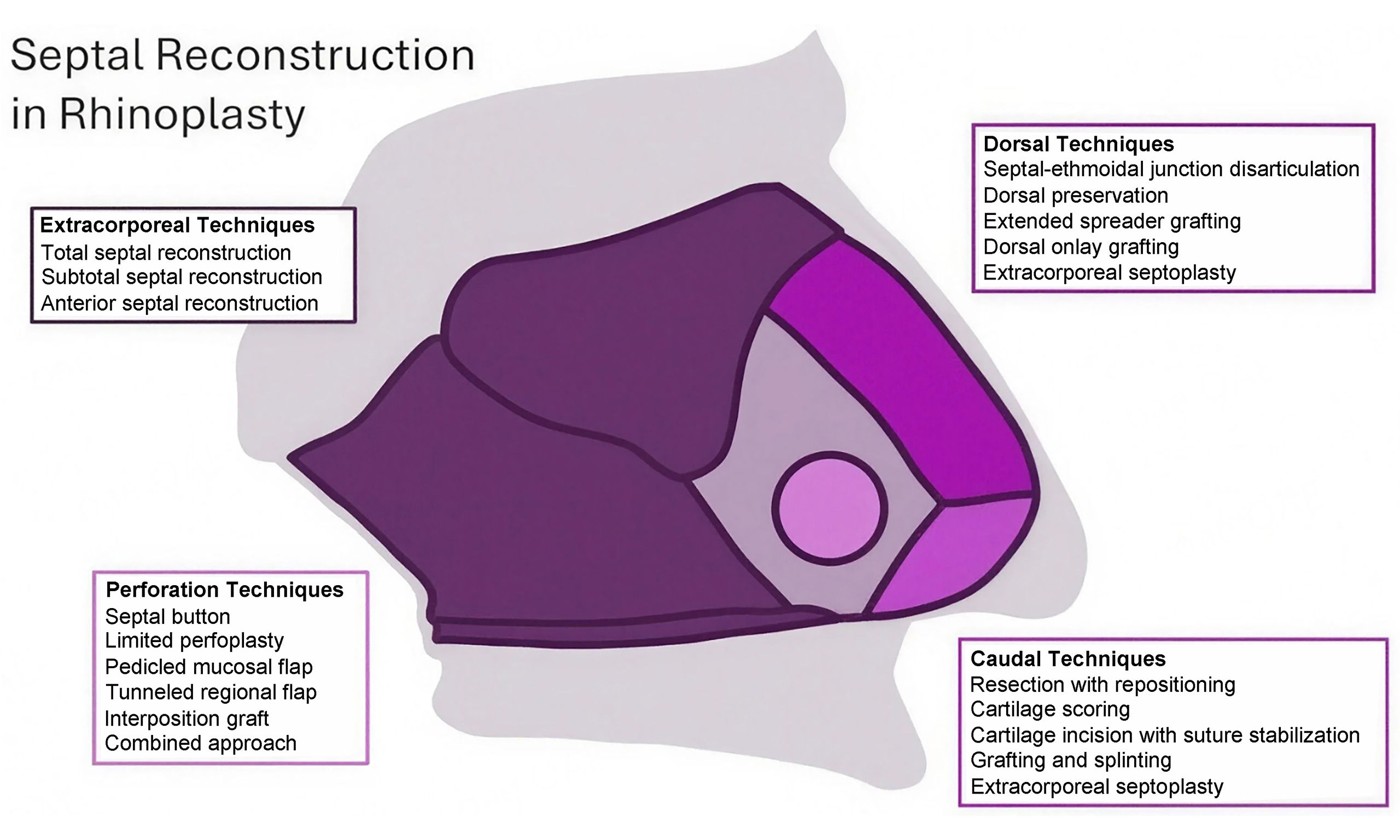
Nasal septum reconstruction is an essential component of a successful rhinoplasty for both nasal cosmesis and function. In this review, we provide both historical strategies and contemporary updates in nasal septum surgery. Conventional septoplasty involves removal of deformed septal cartilage, with care taken to maintain the integrity of the dorsal and caudal cartilaginous L-strut and avoid opposing mucoperichondrial flap perforations that can cause septal perforations after the healing period. When these conditions cannot be met, advanced septal reconstruction techniques may be required to address caudal septal deviation, dorsal septal deviation, and septal perforations, including extracorporeal structural reconstruction in particularly severe cases. Recent refinements of these more extensive techniques also include subtotal and anterior modifications to total septal reconstruction to better preserve the keystone area and dorsal preservation techniques to minimize disruption of aesthetically desirable aspects of the native nose. We conclude with an algorithmic pathway containing major considerations that highlight advantages of each technique described in this review to guide the rhinoplasty surgeon toward appropriate maneuvers to achieve the desired cosmetic and functional result in septal reconstruction.
Keywords
INTRODUCTION
A stable, midline nasal septum is a critical factor in nasal function and aesthetic appearance. Consequently, reconstruction of the nasal septum is an essential component of successful rhinoplasty. The earliest documented attempts at septoplasty date back to circa 3000 BC in ancient Egypt, where nasal fractures were addressed through nasal manipulation followed by the application of bilateral septal splints made of lint, swabs, and linen[1]. Since then, myriad new strategies have emerged using endoscopic, endonasal, and open rhinoplasty approaches for septal repair. This narrative review summarizes historical and recent innovations in techniques for the repair of the deformed nasal septum. Specifically, we discuss the principles of a standard septoplasty as well as strategies for managing complex septal deformities, including caudal septal deviation, dorsal septal deviation and collapse, extensive defects requiring total or subtotal septal reconstruction, and septal perforation. The objective of this article is to describe techniques appropriate for septal reconstruction in both primary and revision adult septorhinoplasty, including both endonasal and open techniques with a greater emphasis placed on the latter. Additionally, we include an algorithmic pathway with considerations that may prompt the rhinoplasty surgeon to include certain techniques in their reconstructive approach. To do so, we queried PubMed and Google Scholar in June 2025 for articles published from January 2010 to June 2025 relating to the search terms “septal reconstruction”, “caudal septal repair”, “dorsal septal repair”, “saddle nose repair”, and “septal perforation repair”, including any review articles and primary publications of case series, prospective studies, and retrospective studies describing techniques for septal reconstruction. We also expanded our literature search using cited articles prior to this time period that were referenced multiple times in the articles yielded by our initial search.
NASAL SEPTUM ANATOMY
The nasal septum is a midline nasal structure composed of a bony-cartilaginous framework surrounded by a mucoperichondrial soft-tissue envelope. Its caudal component is occupied by the quadrangular cartilage while the posterior aspect consists of the perpendicular plate of the ethmoid bone superiorly, the vomer posteriorly, and the maxillary crest inferiorly [Figure 1][2]. Its vascular supply includes branches of both the internal and external carotid arteries. The anterior and posterior ethmoidal arteries arise from the internal carotid artery, whereas the superior labial, greater palatine, and sphenopalatine arteries arise from the external carotid artery[2]. Through its attachment to the ethmoid bone, the superior-most aspect of the septum is anchored to the skull base, creating a potential risk for cerebrospinal fluid leak as a rare complication of septal reconstruction. The lateral attachments of the dorsal septum include the nasal bones in the upper bony vault, the upper lateral cartilages in the middle vault, and medial crura of the lower lateral cartilages at the nasal tip[2,3].
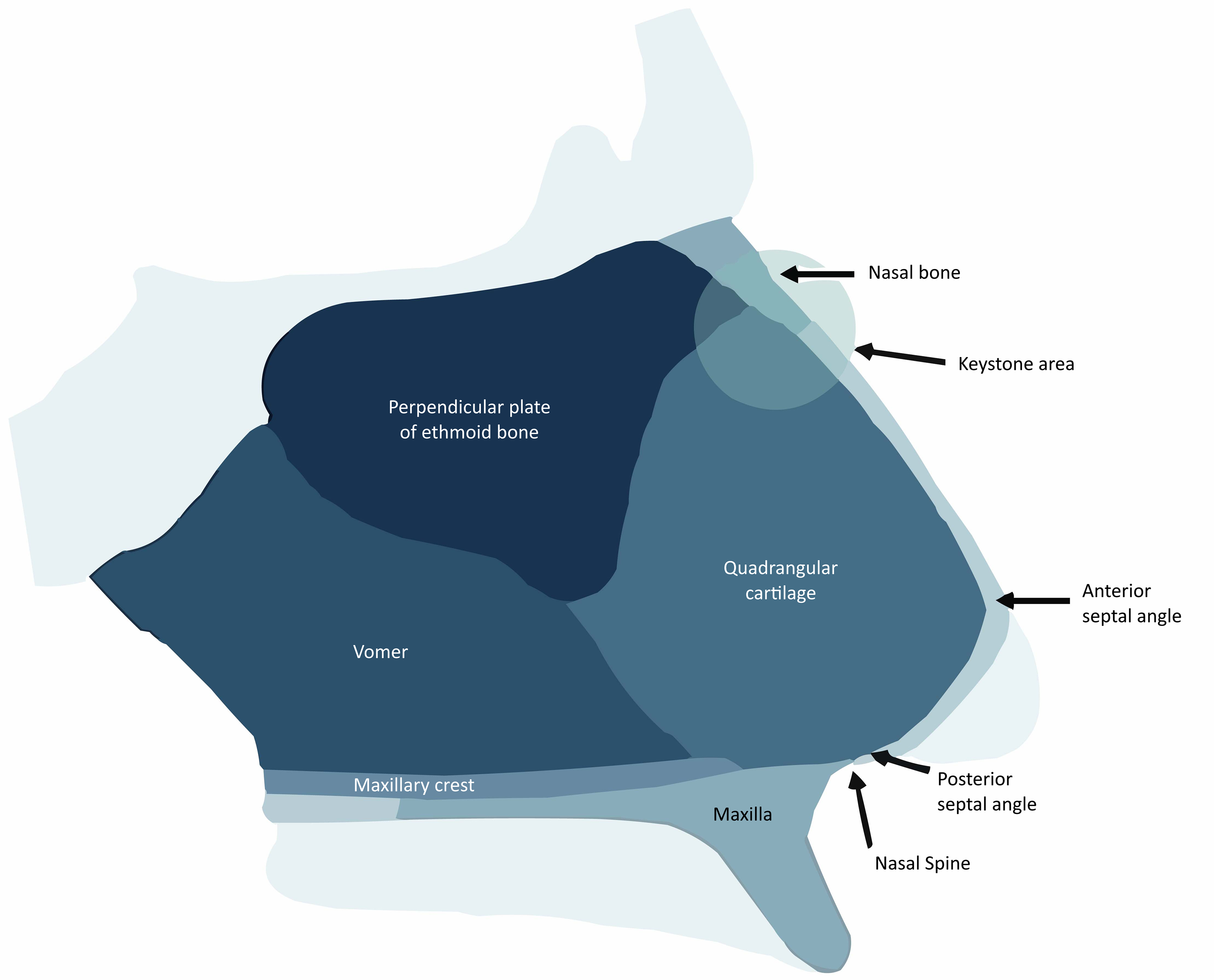
Figure 1. Nasal Septal Framework Anatomy. The nasal septum is composed of the quadrangular cartilage anteriorly, perpendicular plate superiorly, vomer posteriorly, and maxillary crest inferiorly. Reprinted with permission from Oliver & Humphrey. Facial Plast Surg. 2023;39:595-602. Copyright © 2023 Georg Thieme Verlag KG[2].
Key areas of anatomical importance during septal reconstruction include the keystone area and the septal L-strut[3]. The keystone area lies at the junction between the bony upper third and the cartilaginous lower two-thirds of the nasal framework. Preservation of this structure maintains the relative heights of the upper and middle nasal vaults to prevent deformation of the nasal dorsum following septorhinoplasty even in cases of subtotal septal reconstruction. Meanwhile, the septal L-strut is a two-limbed L-shaped structure comprised of the caudal- and dorsal-most aspects of the quadrangular cartilage [Figure 2][4]. Preservation of the L-strut during conventional septoplasty helps ensure adequate nasal tip support.

Figure 2. Septal L-Strut. The L-strut of the nasal septum is composed of the caudal and dorsal segments of the septal cartilage, highlighted in dark gray. Reprinted with permission from Apaydin. Facial Plast Surg. 2016;32:351-360. Copyright © 2016 Georg Thieme Verlag KG[4].
PATIENT COUNSELING
Prior to septal reconstruction and septorhinoplasty, surgeons should seek to understand their patients’ motivations for urgery and expectations for results. A dynamic discussion is required to ensure that patients understand their potential risks and benefits, an appropriate timeline for follow-up and recovery, and the possible need for further revisions in the future. Prior to surgery, patients should optimize medical comorbidities and refrain from use of intranasal vasoconstrictive medications and recreational drugs for at least several months to a year prior to surgery to maximize chances of good post-operative healing[5]. Patients should be counseled on risks of bleeding, septal hematoma, infection, persistent obstruction, intranasal adhesions, and poor wound healing. Additionally, sensory changes - including hyposmia and numbness or sensitivity of the upper teeth, palate, and lip - have been described to self-resolve within several months and should be discussed with the patient[6]. Patients should expect a routine follow-up period of 12-24 months to allow for final stabilization of their post-operative nasal tip and dorsal contour. Rates of revision surgery are variable in the literature and can depend on the severity of septal deformity and the patient’s satisfaction with their functional and aesthetic outcome from their overall septorhinoplasty, with recent studies citing an overall rhinoplasty revision rate of approximately 10%[7].
STANDARD SEPTOPLASTY
Conventional septoplasty can be performed via an endoscopic, endonasal, or open rhinoplasty approach. The open septorhinoplasty approach begins with opening of the nasal envelope via a transcolumellar incision, division of the interdomal ligament to separate the medial crura, and dissection through the midline soft tissue to expose the anterior septal angle. Next, dissection proceeds in a submucoperichondrial plane anteriorly and submucoperiosteal plane posteriorly at the bony septum until all deviated components of the cartilage are fully exposed, separating the upper lateral cartilages from the dorsal septum as needed. Any deviated components of the nasal framework are resected, then soft tissue flaps are reapproximated and secured with a quilting suture and/or bilateral nasal splints[2].
Irrespective of approach, general principles of a standard septoplasty include preservation of a 1.0-1.5 cm anterior and superior L-strut and avoidance of opposing perforations in the mucoperichondrial flaps while eliminating deflected and obstructing elements of the cartilaginous and bony nasal skeleton. However, in patients with severe septal deformities involving the caudal and/or dorsal septum or with existing septal perforations, restoration of nasal function and cosmesis may require more extensive resections and complex approaches to reconstruction, as detailed in the sections below.
CAUDAL SEPTAL RECONSTRUCTION
Caudal septal deviation represents the most common source of persistent deviation after conventional septoplasty[8]. In 1929, Metzenbaum pioneered the “swinging door” technique as the first published approach to displacement of the caudal septum[9]. Since then, five major categories of surgical techniques have been described in the literature: resection with repositioning, cartilage scoring, cartilage incision with suture stabilization, grafting and splinting, and extracorporeal reconstruction.
Resection with repositioning
Resection with repositioning represents the oldest approach to repairing the deviated caudal septum. Metzenbaum’s “swinging door” method involves dislocating the inferior attachment of the caudal septal strut at the anterior nasal spine, minimal resection of redundant septal cartilage, and reattachment to the nasal spine with creation of a small midline groove as needed to secure the midline position[9]. Pastorek and Becker further refined Metzenbaum’s technique to the “doorstop” approach, which instead transposes the cartilaginous strut over the spine with attachment in the contralateral paramedian position while deliberately maintaining a cartilage excess as a “doorstop”[9]. While this approach allows removal of excess cartilage height and repositioning of dislocated cartilage, over-resection can result in loss of tip height, which may be undesirable in cases of the under-projected or over-rotated nasal tip.
Cartilage scoring
Cartilage scoring addresses the challenge of multidirectional interlocked stresses within the septal cartilage, which contribute to its intrinsic warping tendencies[9]. By balancing these forces with releasing partial-thickness cuts on the concave surface, the deviated caudal septum can be straightened while minimizing its propensity to bow back into its native position. Such releasing cuts have been described in the literature using either cross-hatching patterns or parallel scoring[9]. While effective for improving the malleability of the caudal cartilage, scoring inevitably weakens the cartilage strut and may require ancillary strategies, including batten grafting, for adequate support. Additionally, it can be difficult to predict its final position after healing is complete. To further address these challenges, some surgeons also advocate for preservation of a thin 1-2 mm caudal strip without any partial thickness cuts or application of tissue adhesive along the cut surface to avoid excessive destabilization of the caudal strut[9,10].
Cartilage incision with suture stabilization
Cartilage incision with suture stabilization removes excess caudal cartilage height at the site of deflection by either excising or overlapping the cartilage at the inflection point, which is then joined in the straightened position using permanent sutures. These techniques can be combined with Mustardé-type sutures, which were initially described in otoplasty for contouring antihelical fold and are used to correct C-shaped cartilage deformities in septal reconstruction[10]. These straightening sutures are placed as horizontal mattress sutures that are initiated and knotted on the concave side of the cartilage deformity and cross the length of the C-shaped deflection to act as bowstrings. Similarly, Joo et al. describe a crossing suture technique that uses a single suture to combine the straightening action of Mustardé-type sutures with the joining suture[11]. To do so, they start with incision of the cartilage strut to form a superior and inferior segment, then apply a quilting suture to simultaneously straighten convex cartilage surfaces and join the superior and inferior segments. Alternatively, Seo et al. present the use of a traction suture, which anchors the concave cartilage surface at the point of greatest cartilage deflection to the ipsilateral nasal floor[12]. Because these techniques involve wedge resection of a segment of the caudal strut, they destabilize the nasal tip and rely exclusively on the strength of the joining suture to preserve tip height and columellar position.
Grafting and splinting
Grafting and splinting may be performed either alone or in conjunction with the above maneuvers to straighten the caudal septum. Specifically, septal batten grafts are inserted in a submucosal plane along the regions of cartilage deflection[9]. When necessary, septal straightening can be further promoted by using a unilateral graft or an asymmetric thickened graft on the concave side[10]. Grafting materials include autologous or cadaveric bone harvested from the perpendicular plate of the ethmoid bone as well as septal and costal cartilage. For example, the oblique septal crossbar graft obtained from either cartilage or perpendicular plate bone can be useful for stabilization of anterior septal angle reconstruction[13]. Other surgeons prefer alloplastic materials such as silicone, polydioxanone (PDS), expanded polytetrafluoroethylene (ePTFE), porous high-density polyethylene (PHDPE), and polycaprolactone[9,14]. Autologous and cadaveric materials can demonstrate some level of warping and resorption over time and require additional surgeon expertise and operative time to be shaped into appropriate grafts to suit each patient’s unique nasal requirements. Additionally, autologous grafting also carries the risk of donor site morbidity. However, while alloplastic materials can represent a readily available, pre-carved grafting material, a review of six systematic reviews conducted by Nandakumar et al. in 2022 described higher rates of infection, extrusion, and removal surgery for alloplastic materials as compared to autologous and cadaveric grafts[15]. When performed without simultaneous partial- or full-thickness incisions along the deflected caudal strut, grafts and splints allow cartilage straightening without destabilization. However, these grafts also increase the thickness of the septal framework and can lead to an unwanted side effect of nasal obstruction.
Complex caudal reconstruction
Extracorporeal septoplasty describes a technique involving subtotal resection of the septal cartilage, straightening or replacement of the L-strut, and reattachment of the septal framework in the keystone and caudal areas[3,9]. This technique is typically reserved for cases of severe, complex caudal deformity with or without concurrent high dorsal deflection and is further detailed in the sections below.
DORSAL SEPTAL RECONSTRUCTION
As with caudal septal deviation, deformities of the dorsal septum may require disruption of the L-strut to achieve adequate cosmetic and functional outcomes. These abnormalities include high dorsal septal deviation, which causes slanting, twisting, or other asymmetries of the nasal dorsum, as well as saddle nose deformity, characterized by collapse of the middle nasal vault due to insufficient septal cartilage resulting from substance use, trauma, infection, or autoimmune disease[16]. The dorsal septum can be reconstructed using four major strategies described in the literature: disarticulation of the septal-ethmoidal junction, spreader grafting, dorsal preservation techniques, and extracorporeal reconstruction. Additionally, repair of the saddle nose may require additional dorsal augmentation grafting to restore the desired dorsal contour.
Extended spreader grafting
Extended spreader grafts can be designed to span the length of the nasal dorsum to secure the dorsal septum into a straightened midline position[4]. Similar to spreader grafts used for repair of caudal septal deviation, they may be constructed using a variety of autologous, cadaveric, and synthetic materials described in the literature and designed to be thicker on the side of concavity in cases of C-shaped dorsal deviation. Shim spreader grafts, which are constructed from perpendicular plate bone, can allow for particularly robust rigid fixation of a midline dorsum[13]. These techniques can be used either alone or in combination with other techniques that weaken the intrinsic deforming forces of the dorsal septum or rotate the nasal tip medially[4]. For example, the dorsal segment may be scored along the side toward which the tip is deviated to encourage bowing toward midline. Alternatively, clocking sutures may be used to pull the nasal tip toward the contralateral spreader graft to medialize the tip. Deflections may also be resected or incised and re-sutured with spreaders used as stabilizing splints bilaterally[4,17]. While these grafts are effective for straightening a variety of complex deviation patterns, including linear, C-shaped, and S-shaped deviations, they also widen the nasal dorsum which may be aesthetically undesirable in some cases.
Dorsal preservation septorhinoplasty
Dorsal preservation techniques may be employed to address linear dorsal deviations or achieve dorsal nose augmentation in cases of saddle nose. Dorsal preservation surgery was first described by Cottle, Goodale, and Lothrop as “push-down” techniques, which aimed to lower dorsal humps by dislocating the inferior septum from the nasal floor, resecting excess cartilage, performing lateral osteotomies, and lowering the nasal complex en bloc[18]. A corresponding “push-up” technique was described by Toriumi to achieve saddle nose augmentation. This approach similarly involves release of the upper lateral cartilages and inferior septum, as well as osteotomy of the lateral nasal bones, but employs a subdorsal cantilever graft to elevate the middle nasal vault without disrupting the native nasal dorsum[19]. Dorsal preservation techniques can also be used to simply translocate the deviated septum without further cartilage resection or augmentation to shift the deviated nasal dorsum. Consequently, dorsal preservation can be considered in cases where the surgeon desires to maintain favorable aspects of the nasal contour at the midvault and keystone regions and avoid disruption of the soft tissue envelope over these regions. It may also be considered in situations in which the patient is satisfied with the overall tip appearance and desires only a limited augmentation or reduction of the midvault[20]. Meanwhile, structural techniques may be more appropriate when extensive changes including major tip revision maneuvers are warranted to achieve the desired aesthetic and functional outcome.
Septal-ethmoidal junction disarticulation
Disarticulation of the septal-ethmoidal junction allows mobilization of the entirety of the posterior nasal septum[4]. While this technique does not alter the shape of the dorsum, it allows straightening of linear septal deviations without displacement of the nasal tip.
Complex dorsal reconstruction
Finally, as in the case of caudal septal deviation, severe, complex, and/or revision cases of dorsal septal abnormalities may require complete reconstruction of the L-strut with extracorporeal septoplasty[3,4,16]. Saddle nose deformity often requires this approach due to the additional need to reconstruct multiple midvault and nasal tip components, which may be best addressed through replacement of the midline nasal framework.
Saddle nose deformity
In addition to septal repositioning, saddle nose repair often also involves dorsal onlay grafting to increase the height of the nasal dorsum. These grafts are placed between the reconstructed dorsal septum and the nasal soft tissue envelope and are achieved using either carved en-bloc rigid materials such as bone, cartilage, synthetic implants or composite constructs containing a diced rigid component surrounded by a pliable matrix of fascia or glue[17,21]. Four reconstruction paradigms are demonstrated in Figure 3[16]. En-bloc cartilage grafts are predominantly carved from septal, auricular, or costal cartilage, of which costal cartilage often provides the most robust source of grafting material but can be met with challenges of post-operative warping[21]. Cortical bone options include calvarial bone, costal bone, and iliac crest. In 2000, Erol described the “Turkish delight” graft comprised of diced cartilage wrapped in oxidized regenerated cellulose (Surgicel; Ethicon Inc., Piscataway, NJ, USA), then moistened with rifamycin and molded prior to insertion[22]. Although multiple subsequent studies have noted difficulties reproducing the results of their landmark study, multiple other variants of wrapped diced cartilage grafts have been described, particularly using thin fascia grafts such as temporoparietal fascia since it has been associated with lower rates of resorption than cellulose[21]. Additionally, in 2013, Tasman described the diced cartilage glue graft, which combines finely diced autologous cartilage soaked in ciprofloxacin solution with the thrombin component of fibrin glue in a cylindrical mold made from a cut syringe[23]. Before it sets, the composite graft is molded into the desired shape using the fibrinogen-containing component; it is then trimmed of any excess and placed into the nasal envelope.
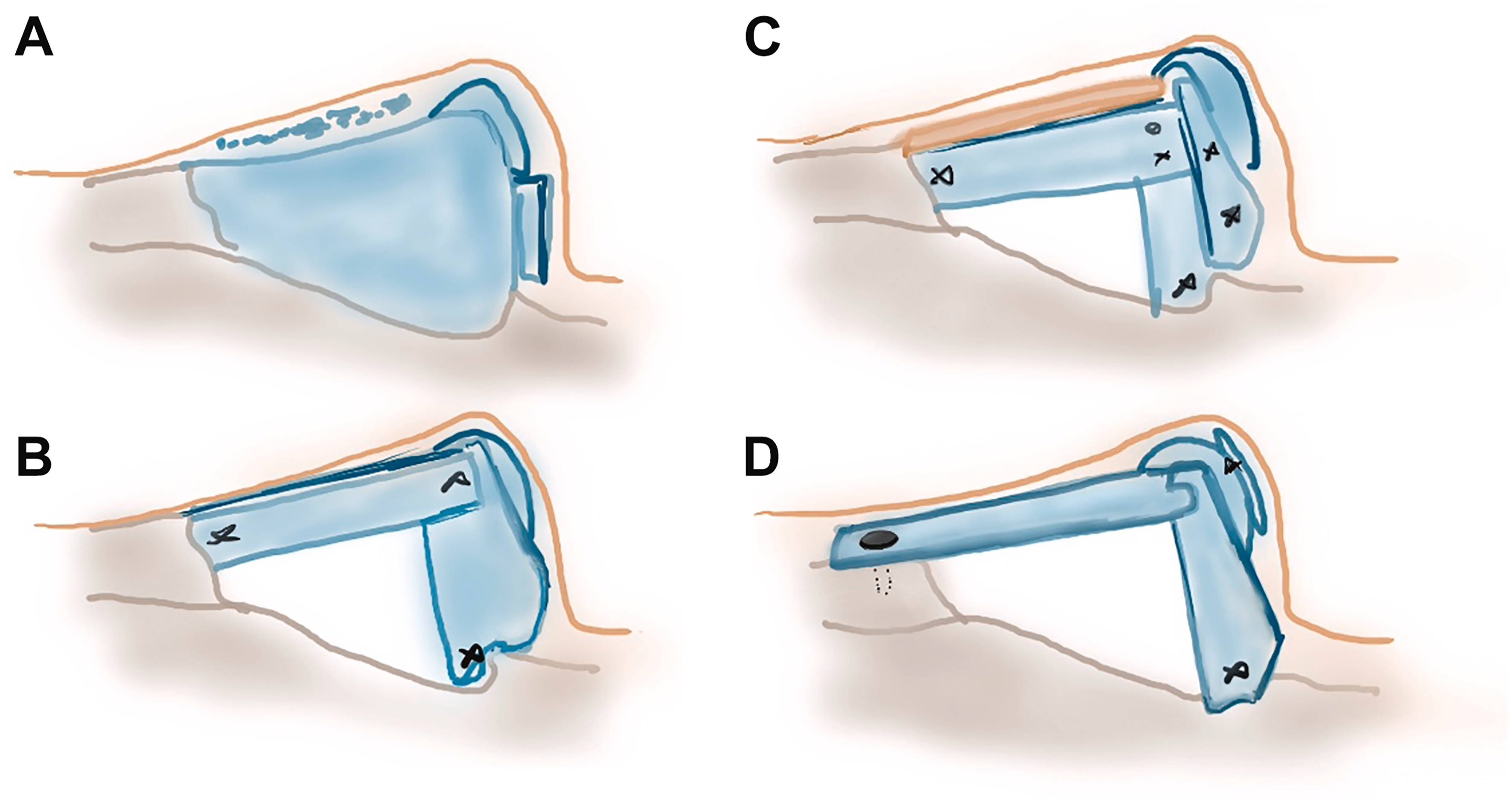
Figure 3. Dorsal Reconstruction for Saddle Nose Deformity. Strategies for management of saddle nose deformity include isolated augmentation without septal revision (A), L-strut reconstruction with caudal extension (B), L-strut reconstruction with dorsal augmentation (C), and complete nasal framework reconstruction with significant disruption of the keystone area (D). Reprinted with permission from Pham et al. Otolaryngologic Clinics of North America. 2025;58:325-41, with permission from Elsevier[16].
Reconstruction for granulomatosis with polyangiitis
Particularly severe cases of saddle nose deformity may be caused by granulomatosis with polyangiitis (GPA), an autoimmune condition characterized by inflammatory microvascular changes and granulomas that can compromise nasal framework perfusion and result in septal cartilage necrosis and collapse of the nasal and facial bones[24]. GPA-associated nasal deformity can be particularly resistant to long-term repair due to ongoing disease relapse and progression after nasal reconstruction. Within this population, Gantous and Garcia describe the use of strong bone or cartilage grafts, including columellar strut, septal extension, and septal replacement grafts that are thicker and larger than for the non-GPA nose with the addition of extended spreader, cantilever dorsal, or L-strut grafts secured with tongue-in-groove techniques in more severe cases of saddle nose deformity[24]. They also recommend intervening early when possible and scheduling surgery after patients are in sustained remission or on a stable low-dose immunosuppressive regimen for at least six months.
EXTRACORPOREAL SEPTOPLASTY
Extracorporeal septoplasty refers to various techniques in which septal reconstruction requires significant cartilage resection with replacement of the L-strut to adequately address nasal deviation or collapse. This technique was first described by King and Ashley in 1952, when they advocated for removal of the entire cartilaginous septum for extracorporeal straightening with subsequent replacement and reattachment at the columella[3]. Gubisch subsequently described a similar technique in 1995 with modifications of the suture technique to better secure the revised septum at the nasal tip[3]. However, this technique is historically associated with relatively high rates of dorsal irregularity due to unpredictable healing after complete cartilaginous resection, with Gubisch reporting a rate of 8%[3].
Consequently, many surgeons who currently perform extracorporeal septoplasty advocate for subtotal rather than total resection of the septal cartilage since retention of a cartilaginous strut at the keystone area can be instrumental in preventing secondary dorsal deformity. This technique of subtotal septal reconstruction was described by Toriumi in 2017[25]. His method starts with an open rhinoplasty approach followed by a subtotal septal cartilage resection with preservation of a 1.5 cm dorsal segment at the keystone area. After ensuring that the nasal spine is at midline, osteotomy is performed to enlarge the bony notch into which the inferior caudal cartilage seats, then the reconstructed L-strut is secured to the nasal spine caudally using PDS sutures and to the dorsal strut remnant using extended spreader grafts before reattachment of the upper and lower lateral cartilages.
Other surgeons have subsequently modified Toriumi’s technique. In 2022, Wang described his variant of the subtotal septal reconstruction, which preserves a 1.5-2.0 cm septal strut at the bony-cartilaginous junction as well as the anterior septal angle[3]. Additionally, his approach includes the routine reconstruction of the caudal septum using a columellar strut graft secured to the medial crura in a tongue-in-groove fashion. Meanwhile, Most described his “anterior septal reconstruction” method in 2023, which similarly involves a more conservative resection with a dorsal strut measuring at least 2 cm in length and 1.5 cm in height and variable preservation of the septal angle [Figure 4][26]. A new L-strut construct is then fashioned from a combination of the straightest segments of the resected septal cartilage and autologous costal cartilage if necessary. The construct is then secured to the dorsal strut and the anterior nasal spine with the use of a titanium miniplate when the nasal spine does not provide adequate structural support or is displaced. While these subtotal techniques minimize the risk of destabilizing the midvault by preserving a dorsal keystone strut, a total reconstruction may still be warranted in dorsal deformities that require extensive modification at the rhinion.
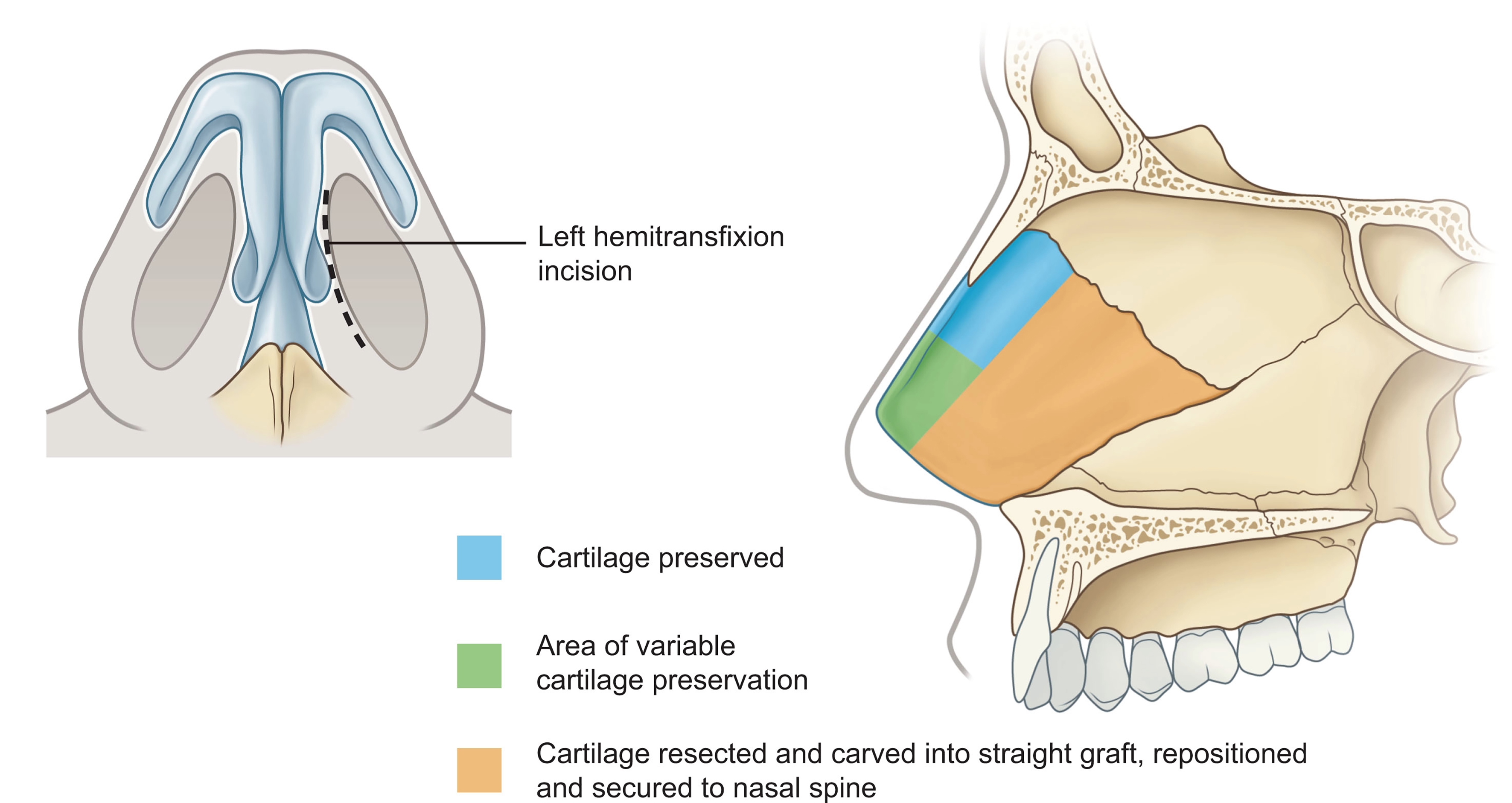
Figure 4. Anterior Septal Reconstruction. This technique involves resection of the entire orange section of the quadrangular cartilage and variable portions of the green section as needed to adequately address the septal deflections. The blue section is preserved to ensure keystone area stability. Reprinted with permission from Rudy & Most. Rhinoplasty. 2023, with permission from Elsevier[26].
SEPTAL PERFORATION REPAIR
Septal perforation may arise as a consequence of trauma, iatrogenic procedures, chronic inflammatory conditions, severe infection, or microvascular changes from substance use disorders or topical medications. Perforations range in size and location and may be either symptomatic or asymptomatic. “Unfavorable” or symptomatic perforations are usually found in the anterior septum and may be characterized by exposed bone or cartilage that acts as a nidus for crusting[27]. In patients who are poor surgical candidates for perforation repair, such perforations can be addressed with application of a septal button prosthesis to act as an obturator or a limited “perfoplasty,” which removes exposed cartilage to allow mucosalization over a more regular surface and reduce crusting. Surgical repair of septal perforations is most often restricted to those less than 2 cm, with success rates lower in those patients with chronic underlying etiologies or perforation size greater than 2 cm[27]. The reconstructive ladder for septal perforation repair includes nonoperative techniques such as septal button and surgical techniques, including perfoplasty, pedicled local mucosal flaps, tunned regional flaps, interposition grafts, and combined approaches.
Pedicled mucosal flaps
Pedicled mucosal flaps are typically used in the context of endoscopic or endonasal approaches to septal perforation repair. These flaps are based on named arteries and can be combined or extended to improve mucosal coverage or reach. The nasoseptal flap is based on the sphenopalatine artery using an intact portion of the posterosuperior septal mucosa and can be extended laterally along the lateral nasal wall or inferiorly along the nasal floor[27]. The anterior and posterior ethmoidal artery flaps are based on their respective named arteries along the dorsal septum and can be extended along the nasal floor or combined to provide a more robust vascular supply[27,28]. The greater palatine artery flap is an inferiorly based flap that includes the caudal septal mucosa and can be used either alone or opposite to a superiorly based contralateral flap to provide a two-layer repair over the septal defect[28]. Finally, the inferior turbinate flap is a posteriorly based flap that allows for two-stage repair of septal perforations involving a first stage for defect closure and a second stage to truncate the bridging mucosa[27].
Tunneled regional flaps
Tunneled regional flaps allow transfer of robust vascularized tissue without sacrifice of surrounding septal mucosa or multi-stage procedures. They can be utilized in the setting of endonasal or open septorhinoplasty. The facial artery musculomucosal (FAMM) flap is a superiorly based buccal mucosal and buccinator muscle flap based on the angular artery that can be tunneled along the nasal floor and lateral to the maxillary crest[27,29]. The gingivolabial sulcus flap is a medially based flap accessed via sublabial incision and tunneled just anterior to the floor of the nasal vestibule[27]. This flap can be raised bilaterally to allow for reconstruction using bilateral opposing flaps. The pericranial flap is an inferiorly based flap pedicled on the supratrochlear vessels that is tunneled along the nasal dorsum into the open rhinoplasty field[27,28]. While this flap allows a large area of donated tissue, it also requires access via coronal incision.
Interposition grafts
Interposition grafts have risen in popularity for robust closure during open rhinoplasty with varying combinations of autologous and alloplastic materials described in recent literature. Monolayer grafting materials include septal or conchal cartilage, temporalis fascia, fascia lata, pericranium, decellularized dermal matrix, and synthetic plates[27,30]. Hadford et al. first described a multi-layer approach using the trilayer temporalis fascia (TPF) graft in 2023, using a PDS plate larger than the size of the septal defect surrounded by a TPF envelope that is carefully placed between the mucoperichondrial septal flaps [Figure 5][31].
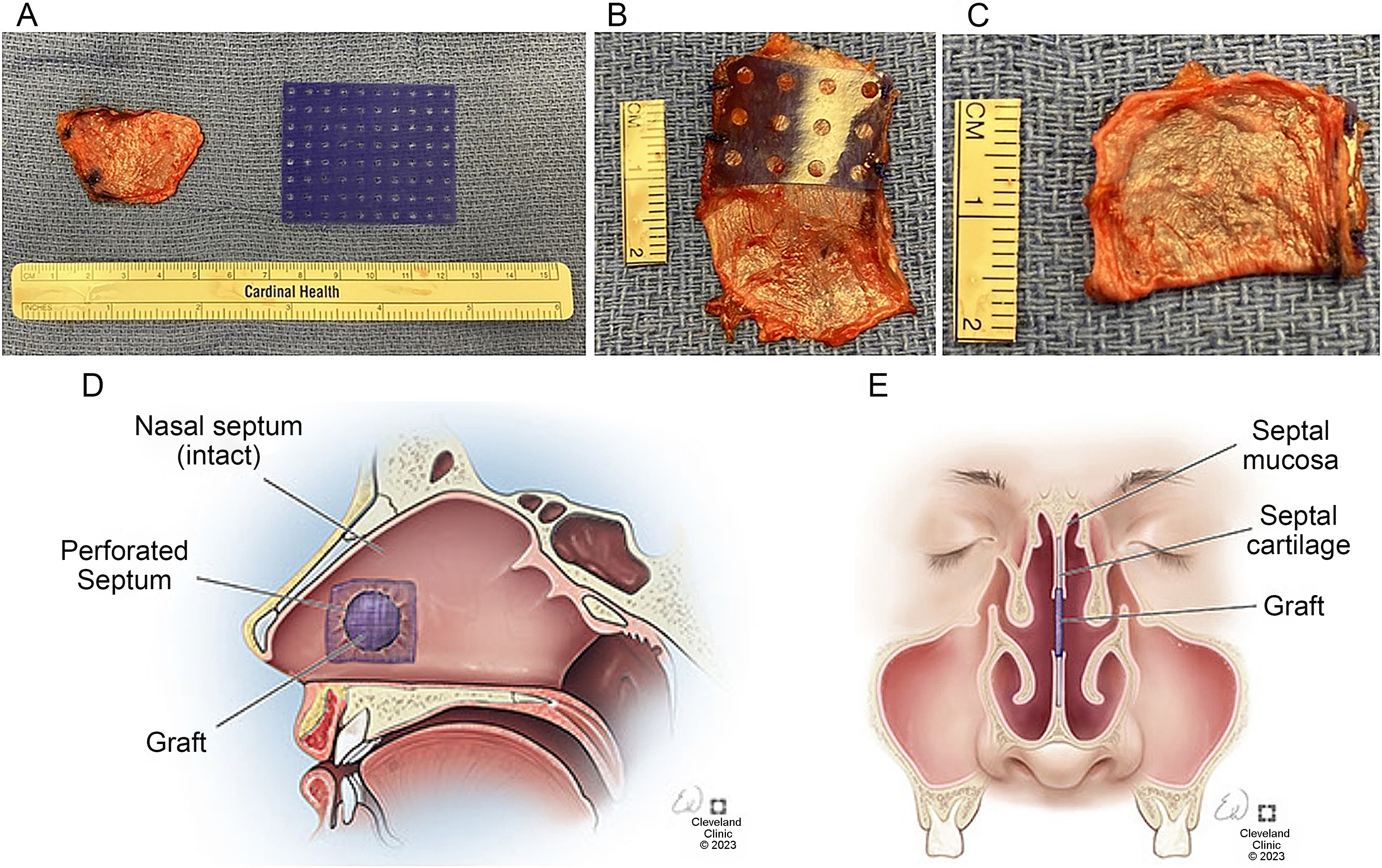
Figure 5. The Trilayer TPF Graft. The trilayer TPF graft is constructed from autologous TPF wrapped around a PDS plate, taking care to ensure that all edges of the plate are completely covered with fascia (A-C). The interposition graft is then placed between the two mucoperichondrial flaps in the area of the septal perforation with the graft size exceeding the size of the defect in both anteroposterior and vertical dimensions (D and E). Reprinted with permission from Hadford et al. American Journal of Otolaryngology. 2023;44:103883, with permission from Elsevier[31]. TPF: Trilayer temporalis fascia; PDS: polydioxanone.
Combined approaches
Finally, combined approaches that include both rotational flaps and interposition grafting may be used to further reinforce the area of repair. Kridel and Delaney describe a “four-quadrant” bipedicled mucosal advancement flap approach wherein bilateral nasal floor and lateral nasal wall rotational flaps are elevated to provide four mucosal grafts that enclose an acellular dermal matrix interposition graft[36].
Perforation closure rates
A recent meta-analysis compared rates of complete perforation closure at 3 months postoperatively between various published surgical techniques[37]. From the 64 studies included, the authors found no differences in closure rates between open vs. endonasal approaches, unilateral vs. bilateral pedicled mucosal, mucoperichondrial, or mucoperiosteal flaps, presence vs. absence of interposition grafts, and use vs. omission of intranasal splinting or packing after repair. While prior studies have shown that closure rates are lower for large perforations greater than 2 cm in greatest dimension, this meta-analysis found no significant difference in closure rates between small and large perforations, defined here by a cut-off diameter of 1.5 cm; however, the authors did note a non-statistically significant 2.25-fold greater odds of closure for small perforations in the endonasal approach subgroup, suggesting a potential benefit of selecting an open approach for large septal perforations.
CONCLUSION
Reconstruction of the nasal septum represents a challenging but essential component of septorhinoplasty. In many cases, conventional septoplasty is adequate for restoration of nasal cosmesis and function, for which it behooves the surgeon to follow the traditional wisdom of preserving the dorso-caudal L-strut. However, more recent innovations in septal reconstruction have sought to address the challenging cases in which the L-strut must be rebuilt to adequately repair the septal deformity [Table 1]. Along with a wealth of strategies for fine adjustments, including various scoring, suturing, grafting, and repositioning techniques, the extracorporeal septoplasty has been increasingly refined in recent years. Following a wider trend of preservation-focused strategies and de-escalation of historically radical procedures in both cosmetic and non-cosmetic surgery at large, the rhinoplasty literature has expanded to describe septal reconstructive techniques that preserve the native keystone region with subtotal and anterior resections[3]. Similarly, Toriumi and Kovacevic describe a preservation push-up technique for saddle nose deformity in the context of a resurgence of interest in preservation rhinoplasty techniques as a whole[19]. Nevertheless, the balance between the versatility and control of structural rhinoplasty and the appeal of maintaining native aesthetic features in preservation rhinoplasty remains a topic of ongoing controversy and conversation in septal reconstruction.
Septal reconstruction techniques
| Technique | Description | Benefits | Drawbacks |
| Conventional septoplasty[2] | Resection of deformed cartilage with preservation of L-strut | Maintains native L-strut | Usually incompletely addresses dorsal/caudal deformity |
| Caudal septum repair techniques | |||
| Resection with repositioning[9] | Dislocate caudal strut and reposition at midline | Maintains single intact segment as caudal strut | Excess resection drops tip height |
| Cartilage scoring[9] | Score on concave surface to encourage straightening | No repositioning | Weakens cartilage unpredictable |
| Cartilage incision with suture stabilization[10,11] | Incision at point of inflection then suture into straightened position | Can straighten sharp deflections | Relies solely on suture strength |
| Grafting and splinting[9] | Application of unilateral or bilateral strut grafts to straighten strut | Maintains native strut strength | Increases width Must overcome intrinsic forces |
| Dorsal septum repair techniques | |||
| Extended spreader grafting[4,9,12] | Application of unilateral or bilateral grafts along dorsal tunnels | Maintains native dorsal strength | Increases width Must overcome intrinsic forces |
| Dorsal preservation[17-19] | Combination of septal incisions and lateral osteotomies/ostectomy to reposition dorsum without fully opening soft tissue envelope | Keeps favorable dorsal features | Limited capacity for major changes Relies on suture strength |
| Septal-ethmoidal junction disarticulation[4] | Separation of cartilaginous and bony septum to mobilize entire posterior septum | Limited disruption of nasal dorsum | For linear dislocations only |
| Dorsal onlay grafting[15,20-22] | Augmentation graft placed along dorsal septum | Allows substantial augmentation | Resorption risk Risk of dorsal irregularities/warping over time |
| Extracorporeal septoplasty techniques | |||
| Total septal reconstruction[3,24] | Removal of entire midline septum, straightening, then replacement | Most versatile Can address severe deformities | Keystone area disruption risks midvault collapse |
| Subtotal/anterior septal reconstruction[24-25] | Replacement of entire septum except dorsal strut at keystone area | Maintains keystone area | Can be challenging to address severe rhinion deformity |
| Septal perforation repair techniques | |||
| Septal button[26] | Prosthetic device that covers area of perforation | Symptom relief in poor surgical candidates | Does not actually repair perforation |
| Limited perfoplasty[26] | Freshens edges and removes exposed cartilage to reduce crusting | ||
| Pedicled mucosal flap[26-27] | Local rotational mucosal flaps based on named arteries | Easily accessed endonasal or open | Donor site crusting |
| Tunneled regional flap[26-28] | Multi-layer regional flaps from oral cavity or pericranial area | Includes multiple tissue layers | Donor site morbidity |
| Interposition graft[26,29-34] | Single or multi-layer graft placed between bilateral soft tissue flaps | Robust scaffold for bilateral mucosalization | Donor site morbidity |
| Combined approach[35] | Combination of unilateral or bilateral rotational flaps with interposition grafting | Maximizes layers of repair | Increased surgical time and donor site morbidity |
Meanwhile, although reported success rates of septal perforation repair remain high in the literature and consistent across techniques, their persistent nature - particularly in cases with underlying chronic etiologies - has prompted surgeons to devise novel multilayered interposition graft materials to be used alone or in conjunction with locoregional flaps[31-35]. While no differences in success rates were detected across different strategies in a recent meta-analysis[37], further long-term studies may be needed to elucidate whether a benefit exists for composite grafts consisting of autologous soft tissue materials wrapped around a rigid plate-like structure as compared to monolayer grafts.
Existing approaches to both simple and complex nasal septal reconstruction are summarized in Figure 6, which also provides a basic algorithm of considerations that may direct the rhinoplasty surgeon toward certain techniques. Since many of the techniques described are drawn from case series and/or expert opinion articles summarizing single surgeon experiences, the final choice in reconstructive approach is ultimately at the discretion of the surgeon in the context of the individual patient’s anatomy. Further research is needed to better elucidate the comparative efficacy of different techniques that address similar types of septal deformities. Additionally, future research may leverage computational modeling and simulation technology to allow virtual surgical planning to craft precise, complex grafts in nasal reconstruction[38]. There also exist opportunities to incorporate emerging technologies in nasal septal cartilage tissue engineering and three-dimensional bioprinting to create fully customized, biocompatible implants[39].
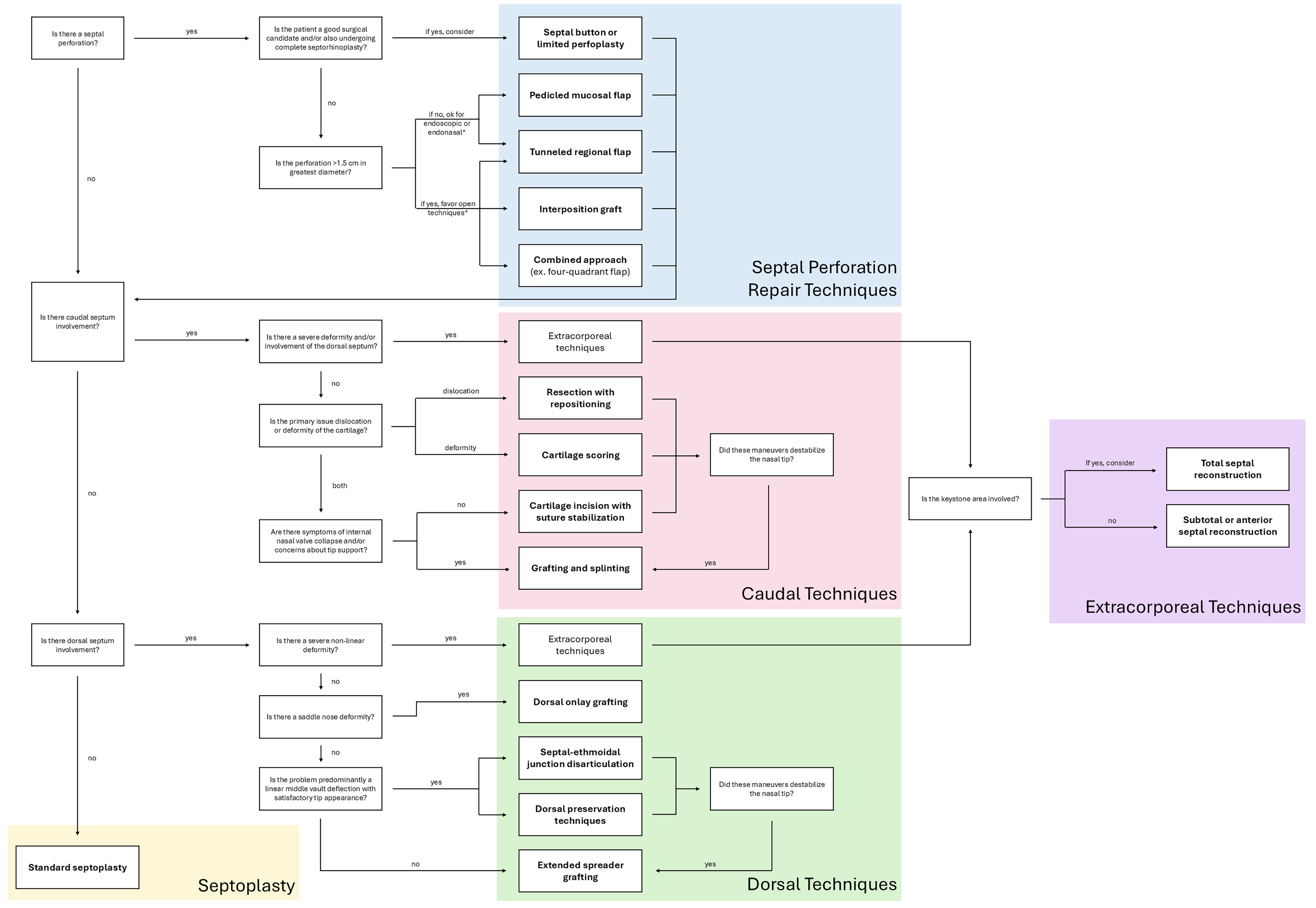
Figure 6. Septal Reconstruction Algorithm. Major considerations when selecting techniques for septal reconstruction in rhinoplasty include presence of septal perforation, involvement of caudal and/or dorsal septum, severity of deformity, baseline satisfaction with tip appearance, and stability of tip support, which are summarized in this figure. *Nearly all septal perforation techniques described can be performed via endoscopic, endonasal, or open techniques but are grouped based on the approach with which they are most often employed.
Amidst the growth of techniques within the septal reconstruction literature, strides have been taken to advance the field in both functional and structural outcomes. As we continue to advance our understanding of novel techniques in grafting and septal stabilization, we will be better equipped to manage complex nasal deformities with greater precision and predictability.
DECLARATIONS
Authors’ contributions
Literature review, manuscript drafting and revision: Feng AY
Manuscript planning, drafting and revision: Echanique KA
Availability of data and materials
Not applicable.
AI and AI-assisted tools statement
Not applicable.
Financial support and sponsorship
None.
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Lam T, Munns C, Fell M, Chong D. Septoplasty during primary cleft lip reconstruction: a historical perspective and scoping review. J Craniofac Surg. 2024;35:1985-9.
2. Oliver JR, Humphrey CD. Septal reconstruction: simple to complex. Facial Plast Surg. 2023;39:595-602.
3. Johnson CZ, Edelmayer L, Wang TD. Management of the deviated caudal septum. Curr Otorhinolaryngol Rep. 2022;10:162-6.
5. Ishii LE, Tollefson TT, Basura GJ, et al. Clinical practice guideline: improving nasal form and function after rhinoplasty. Otolaryngol Head Neck Surg. 2017;156:S1-30.
6. Watters C, Brar S, Yapa S. Septoplasty. Available from: https://www.ncbi.nlm.nih.gov/books/NBK567718/. [Last accessed on 22 Jan 2026].
7. Sibar S, Findikcioglu K, Pasinlioglu B. Revision rhinoplasty after open rhinoplasty: lessons from 252 cases and analysis of risk factors. Plast Reconstr Surg. 2021;148:747-57.
8. Lee DJ, Jo H, Kwon HN, Park JH, Kim SD, Cho KS. Causes and management of persistent septal deviation after septoplasty. Sci Rep. 2022;12:19574.
9. Kim S, Cho K. Management of caudal septal deviation: historic and new techniques. Curr Otorhinolaryngol Rep. 2021;9:409-14.
10. Alshehri WM, AlAwadh IH, Jomah MA, Aldosari BF. Caudal septal deviation: pertinent literature review. J Surg Res. 2021;4:742-8.
11. Joo YH, Cho HJ, Jeon YJ, Kim SW. Use of a crossing suture to correct caudal septal deviations. Int Forum Allergy Rhinol. 2019;9:939-43.
12. Seo HS, Na HS, Kim SD, Yi KI, Mun SJ, Cho KS. Septal cartilage traction suture technique for correction of caudal septal deviation. Laryngoscope. 2020;130:E758-63.
13. Aziz ZS, Brenner MJ, Putman HC 3rd. Oblique septal crossbar graft for anterior septal angle reconstruction. Arch Facial Plast Surg. 2010;12:422-6.
14. Jomah M, Smith O, Villemure-Poliquin N, Cunningham H. Use of alloplastic implants for correction of deviated nasal septum: systematic review and meta-analysis. Am J Otolaryngol. 2024;45:104240.
15. Nandakumar BS, Mukherjee P, Yung AE, Nirmalananda A, Ch’ng S. Grafts in septorhinoplasty: a systematic review and future directions. Aust J Otolaryngol. 2022;5:1-12.
16. Pham TT, Winkler AA, Gadkaree SK. Functional and cosmetic considerations in saddle nose deformity repair. Otolaryngol Clin North Am. 2025;58:325-41.
17. Guliyev M, Erbek SS. Partial septal overlap suture for correcting dorsal septal deviation in crooked nose. J Craniofac Surg. 2025;36:e543-5.
18. Lee J, Abdul-Hamed S, Kazei D, Toriumi D, Lin SJ. The first descriptions of dorsal preservation rhinoplasty in the 19th and early- to mid-20th centuries and relevance today. Ear Nose Throat J. 2021;100:713-9.
19. Toriumi DM, Kovacevic M. Correction of the saddle nose deformity using the “push up” technique. Facial Plast Surg. 2022;38:488-94.
20. Toriumi DM, Kridel RWH, Papel ID, Most SP, Patel PN. Dorsal preservation versus structural techniques and their application. Facial Plast Surg Clin North Am. 2024;32:603-24.
21. Wright JM, Halsey JN, Rottgers SA. Dorsal augmentation: a review of current graft options. Eplasty. 2023;23:e4.
22. El Abany A, Kandathil CK, Castillo N, Abdelhamid AS, Kimura K, Most SP. Outcomes of diced cartilage dorsal augmentation in dorsal aesthetic deformities. Facial Plast Surg Aesthet Med. 2024;26:160-5.
23. Tasman AJ, Diener PA, Litschel R. The diced cartilage glue graft for nasal augmentation. Morphometric evidence of longevity. JAMA Facial Plast Surg. 2013;15:86-94.
24. Gantous A, Fernández-Pellón Garcia RF. Nasal reconstruction in granulomatosis with polyangiitis: a two decade review. Facial Plast Surg Aesthet Med. 2023;25:61-7.
25. Asher SA, Kakodkar AS, Toriumi DM. Long-term outcomes of subtotal septal reconstruction in rhinoplasty. JAMA Facial Plast Surg. 2018;20:50-6.
26. Rudy SF, Most SP. Advanced septoplasty: correction of caudal septal deflection. In: Khan HA, Frame JD, Bagheri SC, Bohluli B, Editors. Rhinoplasty Elsevier; 2023. pp. 31-4.
27. Kimura KS, Ortiz AS, Stephan SJ. Repair of septal perforations. Facial Plast Surg. 2022;38:332-8.
28. Santamaría-Gadea A, Mariño-Sánchez F, Arana-Fernández B, Mullol J, Alobid I. Innovative surgical techniques for nasal septal perforations: management and treatment. Curr Allergy Asthma Rep. 2021;21:17.
29. Feldman J, Marcus B. Revisiting the labial-buccal sulcus flap for septal perforation closure: review at a single institution. JAMA Facial Plast Surg. 2017;19:241-3.
30. Levin M, Ziai H, Shapiro J, Roskies MG. Nasal septal perforation reconstruction with polydioxanone plate: a systematic review. Facial Plast Surg. 2022;38:428-33.
31. Hadford SP, Ciolek PJ, Genther DJ. Trilayer temporalis fascia interposition graft: a reliable technique for nasal septal perforation repair. Am J Otolaryngol. 2023;44:103883.
32. Hanci D, Gurpinar B, Sari H, Uyar Y. A novel technique in septal perforation: fascia lata and costal cartilage sandwich graft. Niger J Clin Pract. 2021;24:1531-4.
33. Hanci D, Onaran Öİ, Altun H, Uyar Y. Innovative repair method for septal perforation repair: the fascia lata and platelet-rich plasma fusion technique. Aesthetic Plast Surg. 2024;48:4095-8.
34. Hancı D, Çelik C, Altun H, Uyar Y. Fascia lata-fat island graft in septal perforation repair. Facial Plast Surg Aesthet Med. 2024;26:339-43.
35. Hanci D, Onaran Öİ, Altun H, Uyar Y. The tricellufuse technique for closing nasal septal perforations. Ear Nose Throat J. 2024;103:93S-8.
36. Kridel RWH, Delaney SW. Simultaneous septal perforation repair with septorhinoplasty: a 31-year experience. Facial Plast Surg. 2018;34:298-311.
37. Fermin JM, Bui R, McCoul E, et al. Surgical repair of nasal septal perforations: a systematic review and meta-analysis. Int Forum Allergy Rhinol. 2022;12:1104-19.
38. Shi B, Huang H. Computational technology for nasal cartilage-related clinical research and application. Int J Oral Sci. 2020;12:21.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Special Topic
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].