


Immunotherapeutic advances for the treatment of osteosarcoma, driven by studies in pet dogs with spontaneous disease
 0
0 
Abstract
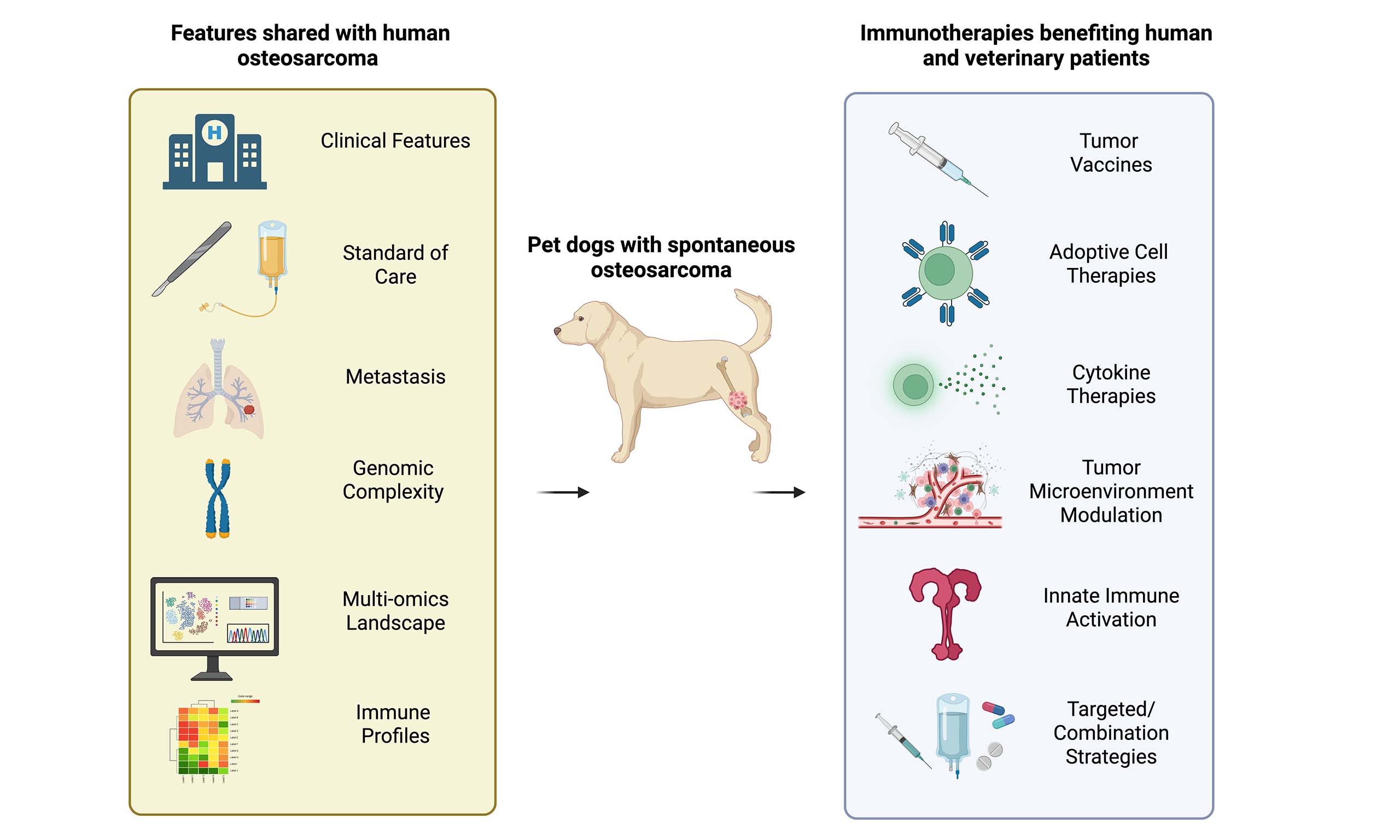
Osteosarcoma is an aggressive bone malignancy that affects approximately 15,000 older, large breed dogs and 800 adolescent and young adult (AYA) humans annually in the US. Pet dogs with osteosarcoma are recognized as a highly relevant, immune-competent patient population which shares clinical, genomic, transcriptomic and immunologic tumor profiles with human osteosarcoma patients. Standard of care has not changed in over five decades and in both species consists of radical surgery and chemotherapy, which in the AYA population causes significant morbidity. Metastases to the lungs occurs in both species and carries a guarded prognosis. There is a clear need for more effective and less toxic treatments. Clinical observations and the survival advantage seen with tumors that are infiltrated with cytotoxic immune cells suggest that the immune system can control osteosarcoma, providing a sound rationale for immunotherapies that boost anti-tumor immunity and generate memory responses, to prevent relapse. The high incidence of osteosarcoma in dogs facilitates collection of tumor tissue for research and performance of clinical trials to advance our understanding of the disease and develop novel therapies, relevant to both species. This review summarizes the exploratory studies that have been performed, often in small cohorts of dogs with osteosarcoma, using tumor vaccines, adoptive cellular therapies, checkpoint inhibitors, and tumor microenvironment modifying strategies. The review also includes the early efforts that are being made to identify correlative biomarkers of response that may inform human clinical trial design.
Keywords
INTRODUCTION
Osteosarcoma is the most common bone tumor seen in dogs and affects 10,000 to 15,000 dogs annually in the United States. In contrast, osteosarcoma in humans is rare and is diagnosed in approximately 800 children, adolescents and young adults in the United States annually. In dogs, the risk of developing osteosarcoma is breed-associated. Large breeds such as Scottish Deerhounds, Irish Wolfhounds, Rottweilers, Great Danes and Golden Retrievers, especially those with long legs and a longer skull conformation, are 30 to 100 times more commonly affected than crossbreeds[1,2]. Studies suggest that there are both heritable and environmental risk factors for canine osteosarcoma, with bone stress and loading implicated in tumorigenesis alongside genetics[1,2]. Standard of care treatment in dogs consists of amputation (less commonly limb sparing surgery) followed by adjuvant platinum-based chemotherapy[3]. An estimated 90% of canine patients have microscopic metastatic lesions at the time of diagnosis and 25% of patients will develop metastatic lesions during carboplatin chemotherapy[4]. Unfortunately, most dogs die from metastatic disease within a year of diagnosis. Although cytotoxic chemotherapy has been reported to prolong survival (median 134 days with amputation alone, median 200-480 days with amputation plus chemotherapy[5]), the benefit of adjuvant chemotherapy is currently being re-evaluated in an ongoing prospective study[6,7]. In cases where amputation is not pursued due to concurrent orthopedic disease, cost, or perceived quality of life issues, stereotactic radiation[8] or palliative radiation therapy can provide tumor control or pain relief for 3-5 months before most patients are euthanized due to progressive disease[9,10]. In contrast, treatment of pediatric osteosarcoma consists of intensive, neoadjuvant, multi-agent cytotoxic chemotherapy followed by surgical resection of the primary tumor and additional adjuvant chemotherapy[11]. While 70% of human patients with localized disease are cured with this approach, patients with metastatic disease at diagnosis or who eventually develop metastatic disease have a guarded prognosis[12].
The collective work of human and veterinary scientists has demonstrated remarkable similarities in the clinical presentation, biologic behavior, genetic complexity and immunologic landscape of osteosarcoma between human and canine patients, leading to the establishment of the dog as a spontaneous model for the human disease. The availability of this parallel canine patient population provides an opportunity to explore disease pathogenesis and therapeutic efficacy that is otherwise challenging in human patients given the low incidence of disease and substantial inter-patient variability that occurs in this species.
Human genome-wide association studies have identified only two susecuptibility loci for osteosarcoma, at 2p25.2 and 6p21.3 (which contains the tumor suppressor gene GRM4), suggesting that germline variants confer modest risk in a subset of human patients[13]. In contrast, canine GWAS have identified 33 osteosarcoma-associated loci across breeds, including a key regulatory variant near CDKN2A/B[14]. These findings led to a renewed interest in the role of CDKN2A in human osteosarcoma where deletions in the gene were associated with a negative prognosis[15]. At the somatic level, osteosarcoma in both humans and dogs is characterized by disruption of tumor suppressor pathways more than activating oncogenic mutations, and both human[15] and comparative canine[16,17] studies report recurrent involvement of TP53, RB1, and PTEN as well as MYC and SETD2. However, a defining feature of osteosarcoma in both species is marked genomic instability, with large structural rearrangements rather than a single dominant driver lesion[18]. This shared genomic complexity supports the value of canine models for pathway-directed therapeutic development, but also highlights the challenge of identifying universal genomic targets for therapy.
In humans and dogs with osteosarcoma, evidence suggests that the immune system plays a pivotal role in disease control, providing a sound rationale to investigate immunotherapeutic approaches. At the end of the 19th century, William B. Coley observed that concurrent erysipelas (Streptococcus spp.) infection in some patients with bone sarcomas was associated with spontaneous remissions and improved outcomes[19]. This led to the development of “Coley's toxins”, a combination of bacterial species, that was administered to bone sarcoma patients with anecdotal reports of successful treatment in some cases[19]. Similarly, although over 100 years later, studies have shown that dogs with osteosarcoma who experienced surgical site infections following limb-sparing surgery, had prolonged disease-free intervals compared to dogs without infection[20,21]. Although a subsequent canine study found no association[22], correlations between infection and prognosis have also been identified in human osteosarcoma patients[22,23]. The association between infections and improved prognosis generated the hypothesis that non-specific activation of the innate and adaptive immune systems can facilitate anti-tumor immune responses and improve outcomes in dogs with osteosarcoma[20,24].
Furthermore, a retrospective transcriptomic study performed using archived canine and publicly available human osteosarcoma datasets supports the idea that anti-tumor immune responses are involved in controlling osteosarcoma in both species[25]. The study identified molecular subtypes of osteosarcoma characterized by the presence or absence of immune cell infiltrates, and revealed that a small subset of patients had tumors that were infiltrated with cytotoxic T cells and natural killer (NK) cells (“immune-enriched” or “hot” tumors). These patients had a significant survival advantage over the larger subset of patients that had a tumor microenvironment devoid of immune cells (“immune desert” or “cold” tumors)[25]. Immune enrichment in the presence of significant, immunosuppressive extracellular matrix (ECM) elements was also associated with a poor prognosis, highlighting the negative immunosuppressive effects of tumor-associated stromal cells on anti-tumor immunity and clinical outcome. In a separate analysis, immunostaining of treatment naïve human and canine osteosarcoma also confirmed the association between a robust anti-tumor T cell infiltrate and a favorable prognosis[26]. Together, evidence from both species reinforces the hypotheses that (1) therapies focused on robustly stimulating tumor-specific cytotoxic T cells and NK cells can lead to tumor control, and (2) induction of immunological memory could help to prevent tomor recurrence.
A useful framework for organizing immunotherapies that promote anti-tumor T cell and NK cell responses is to consider those which support either (i) priming, (ii) infiltration or (iii) tumor cell killing by CD8+ T cells and NK cells, although immunotherapies often aim to achieve more than one of these actions
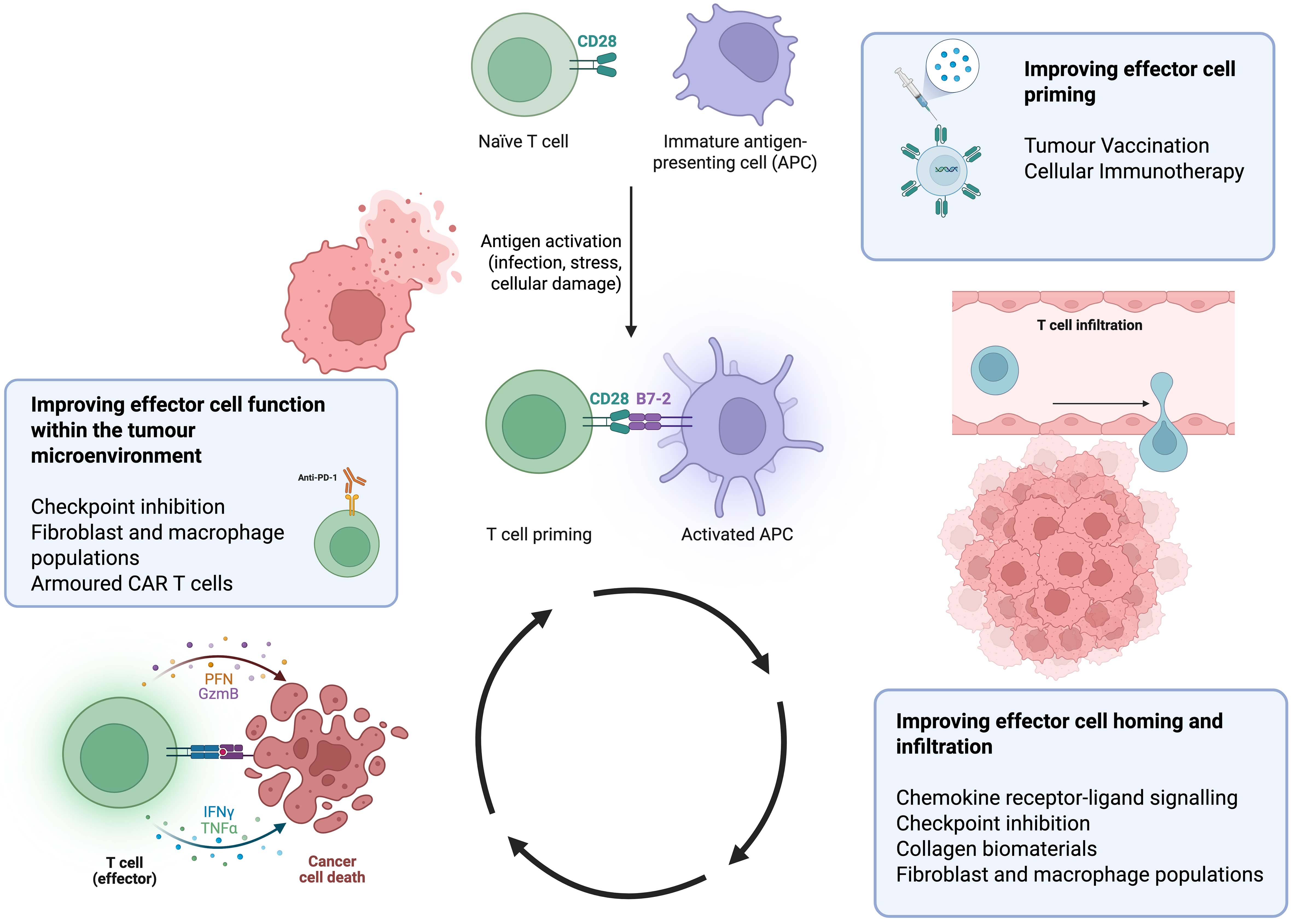
Figure 1. Key examples of immunotherapeutic strategies to enhance anti-tumor immunity in canine osteosarcoma with reference to the cancer immunity cycle of priming, infiltration and tumor-specific killing by effector cells Created in BioRender. Edmunds, G. (2026) https://BioRender.com/x9xb1cc.
In this narrative review, we consider current and developing immunotherapies that are being evaluated in clinical trials in pet dogs with osteosarcoma, analyses of canine clinical populations receiving investigational immunotherapies and the preclinical or mechanistic studies that provided the rationale for clinical evaluation. We particularly focus on current or ongoing studies, many of which are early in development, but are included to provide the reader with an account of the latest advances in immunotherapeutic strategies [Table 1]. Learnings from these studies in canine patients should help to inform how veterinarians manage osteosarcoma going forwards and also help to guide translational strategies for pediatric and adolescent and young adult (AYA) patients.
Summary of selected clinical immunotherapy studies in pet dogs with osteosarcoma since 2016
| Ref. | Study design | Status | Therapy/outcome measures |
| London 2025[6] | Prospective comparative cohort study | Recruiting | Compare outcomes in dogs treated with amputation alone versus amputation and chemotherapy |
| Leblanc et al., 2021[7] | Randomized, two-arm, multicenter, superiority trial | Published | Compare DFI and OS in dogs treated with amputation and carboplatin chemotherapy ± oral sirolimus |
| London et al., 2015[4] | Randomized, prospective clinical trial | Published | Following amputation and carboplatin, assess the benefit of piroxicam/ cyclophosphamide with or without toceranib on DFI and OS |
| Flesner et al., 2020[5] | Single‐site, single‐arm, open‐label prospective trial | Published | Assess safety, tolerability, DFI and OS with autologous cancer cell vaccination, ex vivo expanded T cells and subcutaneous IL-2 |
| Mason et al., 2016[9] | 3 + 3 phase I clinical trial | Published | Safety of HER2-Targeting Listeria and its ability to generate HER2/neu-specific immunity following amputation and carboplatin chemotherapy |
| Kraitchman 2025[36] Doucet et al., 2024[37] | Not yet disclosed | Enrolling | Efficacy of intratumoral STING agonist and carboplatin chemotherapy prior to amputation on DFI, OS and metastasis-free survival |
| Fan 2025[39] | Randomised prospective clinical trial | Finished recruiting | Safety and efficacy of K9-ACV, an autologous tumor cell vaccine combined with the checkpoint inhibitor CD200AR-L, compared to standard-of-care chemotherapy following amputation |
| Marconato et al., 2022[40] | Multi-center, single-arm, prospective trial with historical controls | Published | Dermal administrations of peptide-based anticancer vaccine following amputation and carboplatin. Safety and efficacy (OS, metastasis-free survival, T cell and humoral immune responses) endpoints. |
| Milner 2025[54] | Not yet disclosed | Recruiting | Effect on overall survival of ganglioside targeted vaccine and chemotherapy following radiation or amputation |
| Canter et al., 2017[79] | Tolerability study | Published | Palliative radiotherapy and intralesional NK cell therapy with IL-2. Safety, metastasis-free survival, NK cell persistence in PBMC and tumor |
| Rebhun et al., 2022[81] | 3 + 3 phase I clinical trial | Published | Inhaled rhIL-15 in dogs with gross pulmonary metastases. Safety, ORR, OS and PFS, pharmacokinetic and immune correlative analyses. |
| Mason 2025[84] | Phase I clinical trial | Recruiting | Safety, tolerability, persistence and identification of maximum tolerated dose of B7-H3 CAR-iNKT cells in dogs before or after amputation. Metastasis-free survival, PFS, OS as secondary endpoints. |
| Regan et al., 2022[93] | Prospective dose escalation study | Published | Safety, tolerability, pharmacokinetics, lesion size, immune correlates in dogs with metastatic osteosarcoma treated with amputation followed by losartan and toceranib |
| London et al., 2022[102] | Prospective clinical trial | Enrolling | Adjuvant losartan, toceranib and ladarixin used pre-and post-amputation. Effects on PFS, OS, lung metastases, circulating cytokine concentrations, and gene expression profiles in PBMC |
| Regan 2025[108] | Randomised prospective clinical trial | Enrolling | Safety and anti-cancer activity of fibroblast activation protein (FAP) targeted CAR T cells ± losartan and toceranib in dogs with sarcoma |
| Milner et al., 2025[115] | Not yet disclosed | Enrolling | Determine safety, efficacy and immune correlates of response to adjuvant RNA vaccination and anti-PD1 blockade used alongside radiotherapy in dogs with osteosarcoma |
Tumor vaccines
The overarching goal of a tumor vaccine is to provide tumor antigens together with an adjuvant or “danger signal” that activates professional antigen presenting cells (APCs) and promotes tumor-specific T cell priming and activation[29,30]. APC activation requires the engagement of pattern recognition receptors on their surface by pathogen or danger-associated molecular patterns derived from pathogens, dying cells, and adjuvants[31]. Adjuvants that activate and mature APCs are important components of the vaccination strategy, since APCs that encounter antigen in the absence of danger can become tolerogenic. A significant barrier to generating vaccines to treat osteosarcoma or prevent recurrence is the lack of identified target antigens. In addition, the genetic heterogeneity of osteosarcoma likely necessitates a polyclonal T cell response for tumor control and elimination. Early vaccine strategies addressed these challenges by using autologous or allogeneic tumor cells to supply multiple tumor associated antigens without requiring knowledge of antigen identity. Similar approaches using whole tumor cell lysates together with adjuvants to promote polyclonal T cell responses are still being actively investigated today.
One of the earliest reported immunotherapy studies in dogs with osteosarcoma evaluated Bacillus Calmette-Guérin (BCG), a potent but non-specific immune stimulus, alone (n = 3) or mixed with irradiated, autologous tumor cells (n = 4) and administered intravenously to 4 dogs following amputation[32]. Patients receiving BCG or BCG plus autologous tumor cells were reported to have longer survival times compared to those treated with amputation alone. Subsequent studies evaluating BCG with or without autologous tumor cells after amputation also reported improved survival[33]. Studies in healthy dogs revealed that BCG administration increased NK cell cytotoxicity and increased pulmonary macrophage activation. These findings suggested mechanisms by which micrometastatic disease may be controlled, and helped lay the groundwork for later studies evaluating NK cell therapies and biological response modifiers, including liposomal muramyl tripeptide phosphatidyl ethanolamine (L-MTP-PE; mifamurtide) (see below).
More recently, guided by an increased understanding of the role that the stimulator of interferon genes (STING) pathway plays in anti-tumor immune responses, STING agonists were evaluated in dogs with osteosarcoma. STING agonists drive type I interferon and pro-inflammatory cytokine production and play an important role in tertiary lymphoid structure development[34,35]. Early studies in dogs with osteosarcoma showed that intratumoral administration of a STING agonist is feasible, tolerable and safe, and led to a 2-fold increase in the number of infiltrating CD3+ T cells in the region of the injection[36,37]. Upregulation of Th1 gene profiles was also identified by RNA sequencing at the injection site. Consistent with immune activation, STING administration was accompanied by increased expression of immunoregulatory molecules such as PD-1 and TIM3, supporting combination studies using checkpoint inhibition. Indeed, STING agonists are now being combined with inducers of immunogenic cell death (e.g., cryotherapy) which release tumor associated antigens from osteosarcoma lesions to generate an in vivo vaccine. The results of this in situ vaccination approach on the prevention of metastases in dogs with osteosarcoma are eagerly awaited[36].
Tumor lysate vaccines are now being combined with potent adjuvants such as Cytosine-phosphate-Guanine oligodeoxynucleotide (CpG) or checkpoint inhibitors including CD200 activation receptor ligand (CD200AR-L) to enhance anti-tumor T cell responses and promote epitope spreading. Prospective evaluation of CD200AR-L in combination with autologous tumor lysate in dogs with glioma showed superior progression-free survival when compared with a historical cohort treated with tumor lysate alone[38]. This approach is now being evaluated in the adjuvant setting following amputation in dogs with osteosarcoma[39]. Autologous and allogeneic canine osteosarcoma vaccines have also been prepared from osteosarcoma cells incubated with Salmonella enterica which causes them to release immunogenic peptides. Intradermal administration of these peptides to dogs once a month, for a total of 6 months following amputation and chemotherapy, resulted in improved metastasis-free survival and tumor-specific overall survival when compared to a historical control group that underwent amputation and chemotherapy alone[40].
The development of vaccines that incorporate specific tumor associated antigens for osteosarcoma has been challenging, given the lack of validated targets that are universally expressed. Several antigens have emerged as potential candidates including the epidermal growth factor receptor, HER2/neu[9,41], B7-H3[42,43], Transferrin Receptor-1[44], urokinase plasminogen activator[45] and the disialyl gangliosides GD2/GD3[46,47]. Preclinical identification of such antigens has led to the development of two vaccines targeting HER2/neu and one targeting GD2/GD3 synthase, which have been evaluated in dogs with osteosarcoma.
The chimeric HER2expressing Listeria vaccine (Lm-LLO-HER2) consists of a highly attenuated strain of Listeria monocytogenes (Lm), genetically engineered to express a chimeric HER2 antigen fused to a pore-forming lysin, listeriolysin O[48]. Following intravenous administration, the organism is phagocytosed by APCs and Listeriolysin O mediates escape of listeria components including the chimeric HER2 protein from the phagolysosome into the cytoplasm, enabling antigen presentation through both MHCI and MHCII pathways. This results in priming of HER2-specific CD8+ T cells and CD4+ T cells. Listeria also has potent innate immune stimulatory properties which further enhance T cell priming. Immunization with Lm-LLO-HER2 produced strong cytotoxic CD8+ T cell responses and eliminated HER2+ tumors in mice[48,49]. In a pilot canine study of 18 dogs, administration after amputation and carboplatin was associated with HER2-specific T cell responses and prolonged disease-free interval and overall survival relative to historical controls[9]. In a larger multi-institutional study with 118 intent-to-treat dogs, the survival advantage following vaccination was not observed[50]. However, across both groups, a number of dogs emerged as “elite” survivors, defined as dogs who experienced an overall survival time exceeding two or three times the expected median. Interestingly, elite survivorship was correlated with the augmentation of cytotoxic immune responses following vaccination[50]. Amongst elite survivors, differential gene expression analysis of peripheral blood mononuclear cells (PBMCs) harvested before treatment, identified baseline enrichment of pathways associated with dendritic cell cross presentation, cytotoxic T cell responses and T cells compared with short-term survivors. These findings led to the hypothesis that “immune fitness” or the baseline immunological capability of a patient to respond to immune stimulus might predict clinical response to Lm-LLO-HER2 immunotherapy. Canine trials provide an interesting opportunity to identify immune signatures that might predict successful responses to immunotherapy and enable stratification of immunologically fit patients to immunotherapy treatment groups. A lyophilized Lm-LLO-HER2 vaccine was subsequently developed for commercialization, however, the altered formulation contributed to adverse events and identification of the attenuated Lm within the tumors of several patients resulted in discontinuation of this biological form of the vaccine[51]. Interestingly, Lm is known to home to hypoxic regions and this property has now also been exploited to deliver radionuclides directly into tumors[52]. The initial data with the original frozen form of Lm-LLO-HER2 has supported a pediatric trial in patients with relapsed, resected osteosarcoma which is now fully enrolled, and the final readout of the trial is pending (NCT04974008; COG AOST1221). Based on the canine data, immune fitness biomarkers are being explored in this cohort to determine their value in predicting clinical outcomes.
The second HER2 targeting vaccine approach being explored in canine cancer patients consists of an 18 amino-acid HER2 peptide delivered with the adjuvant, montanide[53]. 93 patients were enrolled on the study, of which 43 had HER2+ appendicular osteosarcoma. Dogs received the vaccine subcutaneously within 3 weeks of their last carboplatin treatment. Vaccination elicited IgG responses against the vaccinal peptide and 65% of patients survived 12 months, with a median survival time of 478 days. The vaccine was generally well tolerated although sterile abscesses at the injection site were reported in up to 30% of all patients immunized. Assessment of baseline immune fitness as a potential correlative biomarker of response has yet to be performed.
A third antigen specific vaccine strategy targeting GD3 is currently being evaluated in dogs with osteosarcoma. In this study, the GD3 vaccine is administered following amputation or radiation therapy and in combination with chemotherapy, every 3 weeks for 6 vaccines. Results of this trial, which include immunological endpoints, are pending[54].
It is important to note that unlike the autologous or allogeneic tumor vaccine approaches that provide multiple tumor associated antigens to generate a polyclonal T cell response, the vaccines described above are engineered to target a single tumor antigen and, as such, their success could rely on the inclusion of powerful adjuvants that boost endogenous immune responses and promote epitope spreading to induce additional polyclonal T cell responses against other tumor antigens besides those included in the vaccine. These responses are essential to combat tumor antigen heterogeneity and circumvent antigen escape mechanisms.
Collectively, the above vaccine strategies have shown encouraging early activity, albeit in small cohorts of canine osteosarcoma patients. Future priorities include rational combinations of vaccines with other therapies including those that induce immunogenic cell death and inhibit checkpoint molecules, and the identification of biomarkers that will enable patient stratification in larger, placebo controlled, clinical trials.
Adoptive cellular immunotherapies for the veterinary clinic
The ultimate goal of immunotherapies is to generate tumor-specific cytotoxic T cells that can specifically recognize, home to and kill malignant cells anywhere in the body[27,28]. An alternative approach to vaccination to achieve this goal is adoptive cellular therapy (ACT). ACT involves the ex vivo isolation, expansion, activation, and/or genetic modification of immune cells to recognize tumor antigens, prior to reinfusion into the patient.
T cell-based immunotherapies
Tumor infiltrating lymphocyte (TIL) therapy works on the hypothesis that T cells within the tumor are specific for a multitude of different tumor associated antigens (reviewed in[55]). TILs isolated from solid tumors and expanded ex vivo, retain their tumor-specific functionality post expansion and mediate potent anti-tumor immunity upon adoptive transfer back into the patient. Insights from transcriptomic profiling of canine CD8+ TILs showed them to be different from circulating CD8+ T cells, having increased expression of 241 genes associated with cytotoxicity and immune activation[56]. However, exhaustion markers such as LAG3, TIM1 and 41-BB were also expressed, along with factors that tune activation signaling (NFKBIA, DUSP4, RGS2 and RGS4), those that enforce tolerance (NR4A3) and others that regulate proliferation[56]. Ex vivo rapid expansion protocols performed in the presence of high concentrations of IL-2 help to reinvigorate TILs, and further expansion in vivo after re-infusion is aided by the concurrent administration of IL-2 to patients[57]. In 2024, the first TIL therapy was approved by the FDA for the treatment of advanced unresectable or metastatic melanoma based on promising results in 73 human patients[58]. This has now led to the exploration of TILs to treat canine cancers. One group recently demonstrated that TILs can be expanded from dissociated canine osteosarcoma samples to achieve clinically relevant cell numbers after a customized rapid expansion protocol ex vivo[59]. Functional assays demonstrated that the majority of these expanded TIL products exhibited reactivity against autologous tumor cells, suggesting that TIL therapy may hold therapeutic promise for dogs with osteosarcoma. To address concerns over TILs exhibiting low TCR affinity for the self-antigens expressed on tumors, chimeric antigen receptor (CAR) technology has been explored to re-direct TILs. One group used a second generation, HER2 targeted, CAR-TIL approach in dogs with squamous cell carcinoma and melanoma which, when administered alongside tumor resection, a tyrosine kinase inhibitor and IL-2, led to transient reduction in tumor size in some cases and one year of tumor free survival in others[60]. Additional engineering strategies to promote the activity of re-infused TILs in the tumor microenvironment are currently being investigated in human TILs[61].
An alternative approach to provide large numbers of autologous tumor-specific T cells for adoptive transfer is to combine autologous tumor vaccination to prime T cells in vivo, with subsequent T cell harvest, ex vivo expansion and adoptive transfer back into the patient. In vivo priming with autologous tumor cells aims to increase the number of tumor-specific T cells in the patient before apheresis, thereby increasing the number in the ex vivo expanded infusion product[5,62]. Autologous tumor vaccination prior to ACT was evaluated in two cohorts of pet dogs with osteosarcoma who underwent amputation without chemotherapy, and clinical outcomes were compared to dogs treated with standard of care amputation and carboplatin. In the first prospective pilot single arm cohort study, 10 dogs received tumor vaccination followed by apheresis and ACT, together with low‐dose systemic IL‐2 to support in vivo expansion of adoptively transferred T cells[5]. This approach produced a median survival time of 415 days, which was comparable to that of dogs receiving standard of care amputation and carboplatin chemotherapy. Although one patient experienced severe immune-related adverse events, the therapy was otherwise well tolerated. In preliminary conference-reported data from a second small (n = 14) study of autologous tumor vaccination and ACT given after a single dose of carboplatin, a one year survival rate of 71% compared favorably to 21% achieved in a matched comparator cohort receiving standard of care carboplatin without vaccination and/or ACT[63]. This ACT/vaccine approach (ELIAS Cancer Immunotherapy) recently received full approval from the USDA Center for Veterinary Biologics for dogs with osteosarcoma. Future prospective studies are warranted to explore predictive biomarkers of immune response that may allow for stratification of patients most likely to respond to therapy.
Although vaccination prior to T cell harvest aims to enhance the potency of cellular products by increasing the frequency of tumor-specific T cells, it relies on effective in vivo T cell priming. However, defects in antigen presentation together with an imbalance in the specificity and affinity of the endogenous T cell repertoire relative to tumor antigens expressed could render vaccines ineffective at priming T cells in some cancer patients[64]. Furthermore, down regulation of MHC molecules on the surface of tumor cells enables them to avoid detection by endogenous and adoptively transferred tumor-specific T cells. To circumvent the requirement for in vivo T cell priming and to overcome MHC down-regulation, autologous T cells can be engineered to express a CAR that enables the T cell to recognize cell surface expressed antigens[65]. CARs are composed of the VH and VL domains of an antibody linked to a T cell co-stimulatory domain and an activating CD3 chain [Figure 2]. When expressed on the T cell surface, the CAR construct allows T cells to detect a membrane bound target antigen, without the need for MHC, activate upon CAR engagement and undergo antigen-specific proliferation, cytokine production and target cell killing. While CAR-T cell therapy has been remarkably successful in hematological malignancies in human patients, it has underperformed in the treatment of solid tumors, including osteosarcoma. Reported reasons for this include failure of trafficking into the tumor, the immunosuppressive tumor microenvironment, and target antigen downregulation and/or heterogeneity within solid tumors. These barriers to effective CAR-T cell therapy are being addressed through engineering strategies to improve trafficking, resist the hostile tumor microenvironment and circumvent epitope loss, for example through expression of bivalent CARs. Furthermore, CARs employing different antigen recognition and/or signaling domains that influence the phenotype of the CAR-T product with effects on function and persistence, are now being evaluated[66,67].
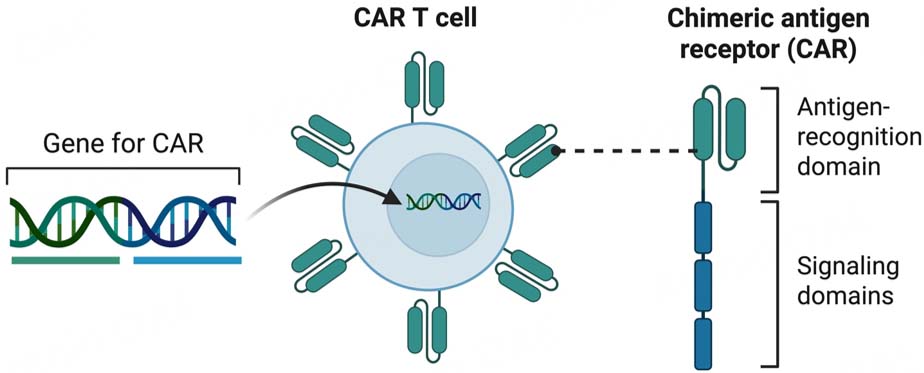
Figure 2. Chimeric Antigen Receptor (CAR) T Cells T cells are harvested from the patient, activated in vitro and then transduced with a lenti- or retro-virus containing DNA that encodes the CAR construct. The construct integrates into the T cells’ DNA, and is subsequently transcribed, translated and expressed on the surface of the T cell. CARs consist of an extracellular antigen recognition domain often made up of a single chain variable fragment (scFv) comprised of the variable heavy and variable light domains of an antibody. The antigen-recognition portion is linked to a hinge and transmembrane domain followed by a co-stimulatory domain (such as CD28 or 4-1BB), and an intracellular signaling domain which is usually the CD3 chain. Upon antigen engagement, CAR signaling domains are phosphorylated and lead to downstream signaling and effector T cell activation, with similar effects to the endogenous T cell receptor. The CAR T cells recognize antigen in an MHC-independent manner and as the CAR construct is integrated into the cellular DNA, daughter cells will also express the CAR. Created in BioRender. Edmunds, G. (2026) https://BioRender.com/atc495e.
Second generation CAR-T cells that target HER2 or B7-H3 have been developed for the treatment of human sarcomas[68,69] and canine osteosarcoma[43,70]. While HER2 targeting CAR-T cells show robust effector function against HER2+ osteosarcoma cell lines in vitro, they failed to show efficacy in pediatric osteosarcoma patients and have not yet been evaluated in the canine clinic. In contrast, B7-H3 targeted CAR-T (and chimeric antigen receptor invariant natural killer T (CAR-iNKT)) cells are currently being evaluated in both human (CAR-T) and canine (CAR-T and CAR-iNKT) osteosarcoma patients. B7-H3 is a checkpoint receptor that is highly expressed in many tumor types including osteosarcoma, where it correlates with a negative prognosis[71]. B7-H3 targeting CAR-T cell approaches have demonstrated anti-tumor activity in vitro and in xenograft models of canine osteosarcoma[42]. Safety and efficacy data is currently being obtained from a canine clinical trial of B7-H3 targeted CAR T cells and CAR-iNKT cells in metastatic and non-metastatic osteosarcoma, and parallel B7-H3 targeting CAR T cell trials in pediatric osteosarcoma are ongoing.
Tumors can downregulate or eliminate targeted antigens/epitopes when placed under selection pressure by natural immune responses or in response to targeted immunotherapy - a phenomenon known as antigen escape. In hematological malignancies, loss of the CAR-targeted epitopes is a well-documented challenge which can lead to CAR-T failure[66,72]. Advanced engineering to generate bi-specific CARs, that target two antigens, or the use of universal CARs that target multiple antigens at once through innovative designs, are now being explored to address issues of antigen escape[73]. Such advances are starting to be explored in canine osteosarcoma but have yet to be tested in the clinic.
Alternative immune cell subsets employed in canine cellular immunotherapy
While autologous T cells are the most commonly used immune subset in cellular immunotherapy, intrinsic T cell dysfunction, associated with advanced disease or prior chemotherapeutics, can limit the effectiveness of T cell therapy. This, together with the high cost and labor-intensive process of generating autologous T cell products, limits their global use in human and canine patients. Together, these challenges have fueled the drive to advance allogeneic cellular immunotherapies, whereby multiple immune cell products can be generated from a single healthy donor and cryopreserved for on-demand use [Figure 3]. Key barriers to adoptive cell transfer with allogeneic T cells include graft versus host disease (GVHD) mediated by MHC mismatch between donor and recipient, and immunological rejection of allogeneic cells by the recipient[74]. While some of these barriers are being addressed by genetic editing of T cell components including disruption of the TCR and MHC molecules, the effects of multiple edits on T cell function are not fully understood. This has led to the exploration of alternative cytotoxic immune cell types including NK and iNKT cells that can be safely transferred into MHC mismatched hosts, without causing GVHD[75].
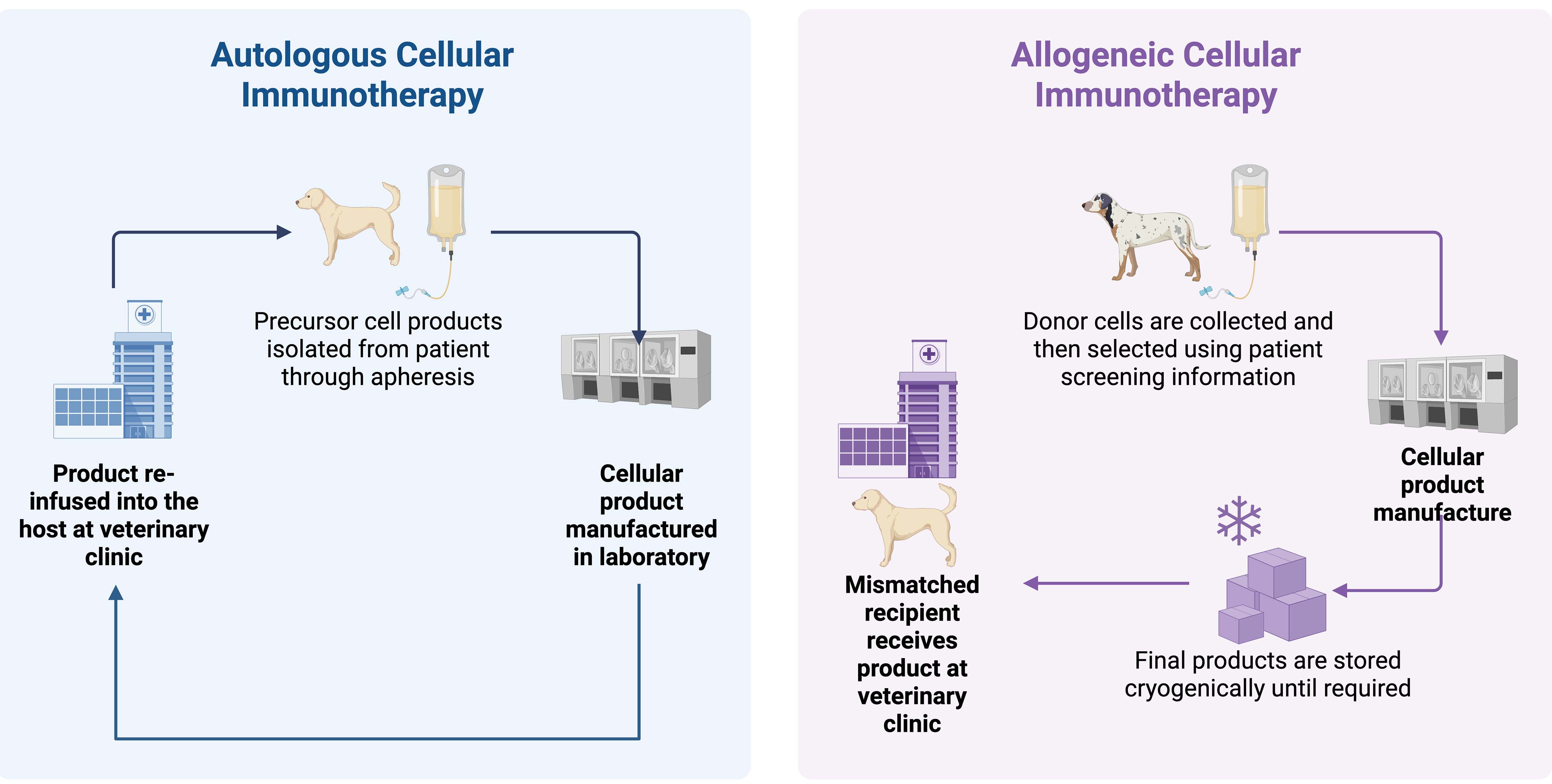
Figure 3. Autologous versus allogeneic cellular immunotherapy for canine patients. Autologous products are generated by isolating patient leukocytes through apheresis, expanding and editing the desired subset in the laboratory and reinfusing the edited cells back into the same patient. Allogeneic products are generated from the peripheral blood of a healthy donor and cryopreserved such that they can be available ‘off the shelf’ and administered to unmatched recipients as needed. Created in BioRender. Edmunds, G. (2026) https://BioRender.com/06j6sgf.
NK cells are innate lymphoid cells which play a critical role in the anti-tumor immune response. NK cell activation depends upon the balance of activating and inhibitory signals received through a multitude of surface receptors such as killer immunoglobulin receptors, which are stimulatory to NK cells, and interactions with self MHC molecules, which inhibit NK cell activation[76]. Malignant cells often down-regulate MHC and are therefore vulnerable to NK cell attack. The use of autologous and allogeneic NK cells either alone or in combination with radiation and/or cytokine support has been actively explored in dogs with osteosarcoma[77,78].
The rationale for combining adoptively transferred NK cells with radiation therapy was supported by in vitro studies suggesting that radiation increases the cytotoxicity of NK cells and enhances their homing to tumors[79]. In a prospective pilot single-arm cohort study, autologous NK cells were administered intra-tumorally to dogs with appendicular osteosarcoma that had undergone palliative radiation. Treatment was generally well tolerated although 3/10 patients developed injection site infections requiring surgical debridement in 2 dogs. Patients experienced a significant increase in CD5+ GranzymeB+ cells in peripheral blood, and one patient had resolution of a suspected metastatic pulmonary nodule, a finding which may be consistent with systemic immune activity. Metastasis-free survival and progression-free survival compared favorably to historical controls[79]. A follow up study by the same group revealed greater increases in CD3 and CD8 gene expression in the peripheral blood of long-term survivors compared with short term survivors amongst NK cell-treated canine patients[80]. These findings provide preliminary evidence that NK cell therapy, in combination with radiation therapy, may potentiate anti-tumor immune responses. The study also suggested that higher serum IL-6 levels at baseline might predict shorter metastasis-free and overall survival, revealing a conflicting role for serum and intratumoral IL-6 as a potential biomarker of prognosis in canine patients[80].
IL-15 is a critical cytokine promoting NK cell activation and expansion and has been delivered via inhalation to enhance local NK cell activity in dogs with pulmonary metastatic osteosarcoma[81]. In a small feasibility study, treatment with inhaled recombinant human IL-15 alone was well tolerated and associated with increases in pro-inflammatory cytokines and some evidence of clinical response. To increase the effectiveness of this approach, inhaled IL-15 was supplied in combination with adoptive autologous NK cell transfer. This approach was found to be feasible, safe and well tolerated, with one out of the five dogs treated developing stable disease[81]. To gain further insights into NK cell biology and therapeutic capabilities, canine NK cells have been extensively characterized using single-cell RNA sequencing which revealed tissue-specific canine NK cell signatures and comparability of canine NK cells to human NK cells[82]. These studies in pet dogs have begun to provide the baseline data required to identify molecular signatures or biomarkers of NK cell fitness that could be valuable in donor selection, ensuring the best chance of success for allogeneic NK cell therapies in the future.
Pet dogs with metastatic osteosarcoma are also being employed to advance the development of adoptive cell therapy (ACT) using a rare subset of T cells known as iNKT cells. iNKT cells comprise less than 1% of peripheral T cells and express an invariant T cell receptor specific for glycolipid antigens presented in the context of the monomorphic non-classical MHCI molecule[74]. Similar to NK cells, allogeneic iNKT cells can be adoptively transferred without causing GVHD and produce cytokines which potentiate cytotoxic anti-tumor immune responses while regulating excessive or toxic immune related adverse events[75,83]. Non-terminal studies in 2 healthy research dogs demonstrated that adoptive transfer of ex-vivo expanded allogeneic, MHC mismatched iNKT cells was feasible, safe and resulted in the persistence of donor iNKT cells within recipients for over 3 months[75]. In this preclinical study, single cell RNA sequencing of ex vivo expanded canine iNKT cells identified significant inter-donor differences in iNKT cell phenotype (e.g., central memory versus effector memory), cytotoxicity and replicative capacity, and these differences were validated using in vitro assays. Therefore, the study provided important information regarding donor variability and the effect of donor selection on allogeneic iNKT products. Engineered allogeneic CAR-iNKT cells are now being evaluated in dogs with metastatic osteosarcoma and as neoadjuvant therapy in primary appendicular osteosarcoma, in NCI supported clinical trials[84]. Serial integrated immunologic analyses of canine patients receiving allogeneic CAR-iNKT cells is ongoing and should help to clarify any immune modulatory and anti-tumor effects of CAR-iNKT cells in this setting.
Improving the recruitment and infiltration of anti-tumor immune cells into osteosarcoma lesions
A transcriptomic analysis which compared 190 canine primary osteosarcoma lesions with 8 canine metastatic lesions and 405 samples from 8 human osteosarcoma datasets revealed that primary tumors can be categorized into three subtypes depending on their immune content (i) “immune enriched”, (ii) “immune desert”, and (iii) “immune enriched with dense ECM”[25]. The most common subtype in this study, immune desert, lacked any significant immune infiltrate, including T and NK cells, and is considered to be immunologically “cold”. Conversely, a small subset of canine and human osteosarcomas contained T and NK cells and are considered immunologically “hot” or “immune-enriched”, a phenotype which was associated with prolonged disease-free intervals and overall survival[25]. These findings support those of contemporaneous[85] and earlier[86] studies which identified transcriptomic signatures associated with inflammation and immune activation that correlate with improved outcome in canine and human osteosarcoma cohorts. While the factors that determine whether osteosarcoma lesions are immunologically hot or cold remain under investigation, failure of T cell homing and penetration into the tumor, owing to inadequate chemoattractant signaling and/or physical and functional barriers appear to contribute to immune exclusion[85,87,88].
To improve the homing of CAR-T cells to tumors, CAR constructs have been engineered to express chemokine receptors such as CXCR2 for the treatment of hepatocellular carcinoma in people[89]. Canine osteosarcoma cells were shown to secrete the CXCR2 ligand CXCL8, and canine B7-H3 CAR-T cells expressing human CXCR2 migrated towards canine CXCL8 in transwell assays[42]. Interestingly, in this study, B7-H3/CXCR2 CAR-T cells showed enhanced functionality over standard B7-H3 CAR-T cells in vitro, producing more IFN-γ and IL-2 and showed improved persistence and anti-tumor function in vivo in mouse xenograft models. The CXCR2 engineered CAR-T cells had a distinct transcriptomic profile with increased expression of genes related to T cell activation, while genes related to functions such as G-protein coupled receptor signaling and lipid metabolism were downregulated. While this preclinical study did not specifically evaluate the effects of CXCR2 expression on CAR-T homing to tumors in vivo, it revealed unexpected effects of increased CAR-T persistence and activity, and provides an interesting avenue of exploration for next generation CAR-T cell design.
In humans, combining RNA sequencing data with spatial biology approaches and screening of a library of FDA approved compounds have shown that manipulation of the CXCR4 axis may improve immune infiltration in osteosarcoma[88]. In addition, single cell RNA sequencing of canine osteosarcoma identified a CXCL13/IL21 expressing CD4+ T follicular helper population that has previously been associated with favorable anti-tumor responses in other species[85]. Collectively, these data indicate that manipulating chemokine signaling may represent an avenue for further exploration in osteosarcoma, and the availability of a growing body of canine omics data may allow improvements in the efficacy of CAR-T cells in solid tumors in the veterinary and human clinic.
Targeting the tumor microenvironment
Another physical and functional barrier to effective anti-tumor T cell responses in osteosarcoma is the tumor microenvironment. The tumor microenvironment is composed of a potent mixture of immunosuppressive cell populations including subsets of cancer associated fibroblasts (CAFs), tumor-associated
Both human and canine data suggest that monocytes develop into macrophages which are implicated in conditioning the tumor microenvironment and metastatic niche in osteosarcoma[26,88,93]. Historically, macrophages were divided into M0 (“resting”), M1 (“anti-tumor”) and M2 (“pro-tumor”) populations, but their phenotype is now known to be much more fluid and nuanced[94]. The complexity and diversity of macrophage subsets in osteosarcoma is extensive, and this may explain in part the conflicting reports of the roles they play in anti-tumor immunity across different studies.
Targeting myeloid subsets that are beneficial to anti-tumor immunity
Multiple studies in human osteosarcoma have shown that macrophage infiltrates and M2 phenotypes positively correlate with outcome[95,96]. In the previously referenced retrospective transcriptomic study[85], CIBERSORT was used to deconvolute immune populations in canine osteosarcoma tissue, and the authors unexpectedly found that M2 subsets were enriched in the favorable outcome group whereas M0 macrophages were associated with a poor prognosis[85]. Furthermore, a retrospective pathology study of 24 canine osteosarcomas used immunostaining to show that the % area of CD204+ (M2 like) macrophage staining within the primary tumor positively correlated with CD3+ T cell and FOXP3+ infiltrates, and with disease-free interval but not with overall survival time[26]. Thus, in both human and canine osteosarcoma, and in contrast to other tumor types, specific subsets of tumor associated macrophages (TAMs) appear to be beneficial, and this has formed the basis of employing macrophage-activating agents therapeutically. One such agent is liposomal muramyl tripeptide phosphatidyl ethanolamine (L-MTP-PE), which in a prospective randomized double-blind placebo-controlled clinical trial was found to extend survival when administered to dogs with appendicular osteosarcoma following amputation and cisplatin chemotherapy[97]. A similar benefit was identified in non-metastatic pediatric osteosarcoma patients, treated with mifamurtide (Mepact), a muramyl-dipeptide derivative, following definitive surgery and in combination with maintenance chemotherapy[98]. Mifamurtide is now approved by the European Medicines Agency for treatment of high-grade, resectable, non-metastatic osteosarcoma in pediatric and young adult cohorts[99]. Although the initial studies showing survival benefit using mifamurtide were performed in dogs, it is not FDA approved for veterinary use.
Targeting myeloid subsets that are detrimental to anti-tumor immunity
Conversely, several canine and human studies also support a tumor-promoting role of macrophages in osteosaroma. Transcriptomic studies have shown that CCL2 (also known as monocyte chemoattractant protein-1, MCP-1), a protein that plays a central role in monocyte recruitment to areas of tissue damage and inflammation, is highly expressed in primary and metastatic canine osteosarcoma lesions[25]. In murine and human preclinical models, CCL2 was associated with intra-tumoral enrichment of CCR2+ myeloid cells, angiotensin-II driven upregulation of TGF-β signaling, macrophage recruitment and collagen deposition/fibrosis, contributing to the pre-metastatic niche[100]. Drug library screening identified the angiotensin II receptor blocker, losartan, as an inhibitor of CCL2 that might block or retard development of an immunosuppressive metastatic niche. This hypothesis led to mouse studies and canine clinical trials in which treatment with high doses of losartan was associated with partial responses in 4/16 dogs and stable disease in 4/16 dogs[93]. At the highest dose of losartan, 95% and 66% increases in median progression-free survival and overall survival respectively were observed. Losartan treatment was also associated with reduced circulating monocytes in a subset of dogs in this study, who experienced prolonged progression-free survival compared to those with no changes in monocytes in response to therapy[93]. Losartan treatment did not affect serum TGF-β concentrations, suggesting that its primary mode of action was inhibition of monocyte recruitment to osteosarcoma lesions. The combination of losartan and toceranib is now widely employed in the treatment of dogs with metastatic osteosarcoma by veterinary oncologists. These promising results in pet dogs led to an ongoing study of losartan and sunitinib in human patients with metastatic osteosarcoma, exemplifying that findings from canine studies are being used to inform clinical trials in human osteosarcoma patients[101]. Canine studies have now been extended to include the CXCR1 and CXCR2 inhibitor ladarixin, in combination with losartan and toceranib. Preliminary reports indicate that this regimen has produced objective responses and clinical benefit in some dogs with pulmonary osteosarcoma metastases, although the final results are pending[102]. Early gene expression profiling data generated from the PBMC of dogs treated in the triple combination therapy trial, has so far shown therapy-induced alterations in genes and pathways with obvious relevance to anti-tumor immunity e.g., downmodulation of the checkpoint inhibitor cytotoxic T-lymphocyte associated protein 4 (CTLA-4), and upregulation of CCL19 (a chemokine ligand involved in lymphocyte recruitment)[102]. Given the promising results in the initial trial, losartan/toceranib/ladarixin is now being evaluated in the adjuvant setting in dogs post-amputation, in the absence of systemic chemotherapy.
Since myeloid cells are heterogeneous, identifying specific subsets and establishing their role in tumor progression and metastasis is a key focus of current research[103]. Collaborations between veterinary and human research groups, including analyses of clinical cohorts across humans[94] and dogs[102], may inform therapies that eliminate immunoregulatory macrophage subsets whilst preserving those that support anti-tumor immune responses.
Cancer associated fibroblasts
CAFs are also thought to play a fundamental role in stromal conditioning and immunosuppression in canine osteosarcoma. In one study, canine CAFs isolated from the tumors of dogs with malignant epithelial tumors, were analyzed using immunostaining and ELISA and were shown to produce CXCL12[104]. CAF derived TGF-β augmented this effect, acting in an autocrine manner to upregulate CXCL12 secretion. CXCL12 is a cytokine which may encourage CXCR4-expressing T cells to sequester in the peritumoral stroma rather than infiltrating the tumor, and CAF derived TGF also functioned in an endocrine fashion to increase CXCR4 expression by T cells[104]. Overall, this canine study provided evidence in support of the CAF-mediated CXCL12-CXCR4 axis contributing to immune exclusion in solid tumors. Spatial transcriptomic analysis has also shown that the CXCR4 axis is important in the peritumoral region of human osteosarcoma metastases[88]. Further analysis of CAFs in canine osteosarcoma could support a renewed drive to target fibroblasts for therapeutic gain.
In order to target CAFs, markers of immunosuppressive CAF subsets must be defined. Amongst human cohorts, fibroblast activating protein (FAP) is expressed by CAFs and has been targeted with radionucleotide therapy and CAR-T cells, leading to CAF depletion and control of tumor growth in clinical trials of multiple cancers, including osteosarcoma[105]. However, markers of immunosuppressive CAFs have previously been lacking in dogs. Canine-specific omics and immunostaining analyses have now allowed canine CAF subsets to be better characterized, and populations expressing SFRP2 and PRSS23 at the gene level[106], and FAP at the protein level[107] have been shown to be associated with a negative prognosis in pet dogs. Subsequently, cross-reactive anti-FAP antibodies have been identified, paving the way for FAP-targeted antibodies and CAR-T cells to enter the canine clinic. Current canine trials are employing FAP-directed CAR-T cells in combination with telmisartan and toceranib, to collectively address the immunosuppressive TME. The clinical outcome data of these studies together with immune correlates of response to therapy are eagerly awaited[108].
Checkpoint inhibition and combination therapies
Checkpoint inhibitors, which block the interaction between inhibitory ligands (expressed in the tumor microenvironment and draining lymph node), and their receptors on activated immune cells, are now entering the veterinary clinic. Monoclonal antibodies which inhibit canine programmed cell death protein 1 (PD-1), programmed cell death ligand 1 (PD-L1) and CTLA-4 have now been generated and are being evaluated in pilot clinical trials both as monotherapy and combination therapies in dogs with various tumors[109-112]. Osteosarcoma expresses PD-L1 at high levels, and immunohistochemistry showed that metastatic OS lesions expressed higher levels of PD-L1 and Herpes Virus Entry Mediator (HVEM, CD270) compared with primary lesions. Expression of these checkpoint ligands correlated with reduced infiltration of CD8+ T cells[113] and a novel canine anti-PD-L1 antibody has shown some activity against osteosarcoma in canine xenograft models[114]. Dogs are also paving the way to evaluate the combination of RNA-based vaccines with checkpoint immunotherapy, and the first canine clinical trial combining anti-PD1 monoclonal antibodies with a RNA-based vaccine for osteosarcoma is enrolling at present, generating safety and efficacy data which could inform translation of such combinations into the human and veterinary oncology clinic[115].
CONCLUSIONS
In the last two decades, a comparative body of evidence has established that pet dogs with spontaneous osteosarcoma are valuable “models” for the pediatric disease. This has lead to increased investment in research aiming to understand canine osteosarcoma’s pathogenesis, identify target antigens, evaluate the effects of immunotherapeutics and identify correlative biomarkers that predict therapeutic response and outcome. As an increasing number of assays and molecular tools have become available for use in dogs, investigations have provided important information that has increased our understanding of the tumor’s immune composition, the physical and functional barriers that protect it from immunologic attack and potential immunotherapeutic targets. Based on these findings, rationally designed immunotherapeutics and combination strategies to treat osteosarcoma and prevent metastases are being evaluated in the adjuvant and neoadjuvant setting. Despite some differences in host genetic susceptibility, standard of care treatment, trial design and regulation, findings from preclinical and clinical studies in dogs have successfully informed the design of therapeutic strategies for pediatric, adolescent and young adult human patients. Furthermore, population level findings from multiple canine clinical studies suggest that a subset of "elite" responders to immunotherapies exist, who experience unusually prolonged survival times across different cancer histologies. Preliminary data from immune assays performed in these studies has led to the hypothesis that a patient’s baseline immune fitness and capability of responding to immunotherapies might distinguish elite from poor responders[50]. Future studies will address this hypothesis and may allow for stratification of patients to immunotherapy trials based on their immune profile pre-treatment.
Durable anti-tumor responses are likely to depend not only on early cytotoxic responses but also on the persistence of effective anti-tumor immunity afforded through the formation of immunological memory. This area has been understudied in osteosarcoma, and it could be explored in detail amongst the cohorts of canine patients that are currently receiving experimental treatments, in order to advance the field. In this narrative review, we have focused on canine clinical trials, or analyses of canine clinical populations being treated with immunotherapy. However, canine populations are also providing insights into other aspects of osteosarcoma including epidemiology, Genome Wide Association Studies (GWAS), targeted molecular therapies, hormone receptor expression, oncolytic viruses, ferritinophagy, and the exploitation of the gut microbiome for prognosis and treatment. Overall, the large body of canine data being generated is predicted to increase our understanding of the biology and immunobiology of osteosarcoma and inform improvements in our treatment and management of the disease in both humans and dogs over the next decade.
DECLARATIONS
Acknowledgments
Graphical Abstract created in BioRender, Edmunds GL (2026) https://BioRender.com/el6yu4s.
Authors' contributions
Drafted the manuscript: Edmunds GL
Provided conceptual guidance, wrote additional sections, critically revised the manuscript for intellectual content, and supervised the work: Mason NJ
Both authors reviewed and approved the final manuscript.
Availability of data and materials
Not applicable.
AI and AI-assisted tools statement
During the preparation of this manuscript, the AI-assisted language tool including ChatGPT version 4.0 was used solely for language editing and readability improvement. These tools did not influence the study design, data collection, analysis, interpretation, or the scientific content of the work. All authors take full responsibility for the accuracy, integrity, and final content of the manuscript.
Financial support and sponsorship
None.
Conflicts of interest
Mason NJ reports being a co-founder of Vetigenics, Edmunds GL declared that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Edmunds GL, Smalley MJ, Beck S, et al. Dog breeds and body conformations with predisposition to osteosarcoma in the UK: a case-control study. Canine Genet Epidemiol. 2021;8:2.
2. O’neill DG, Edmunds GL, Urquhart-Gilmore J, et al. Dog breeds and conformations predisposed to osteosarcoma in the UK: a VetCompass study. Canine Med Genet. 2023;10:8.
3. Selmic L, Burton J, Thamm D, Withrow S, Lana S. Comparison of carboplatin and doxorubicin-based chemotherapy protocols in 470 dogs after amputation for treatment of appendicular osteosarcoma. J Vet Intern Med. 2014;28:554-63.
4. London CA, Gardner HL, Mathie T, et al. Impact of toceranib/piroxicam/cyclophosphamide maintenance therapy on outcome of dogs with appendicular osteosarcoma following amputation and carboplatin chemotherapy: a multi-institutional study. PLoS ONE. 2015;10:e0124889.
5. Flesner BK, Wood GW, Gayheart-Walsten P, et al. Autologous cancer cell vaccination, adoptive T-cell transfer, and interleukin-2 administration results in long-term survival for companion dogs with osteosarcoma. J Vet Intern Med. 2020;34:2056-67.
6. London C. Characterization of naturally occurring osteosarcoma in dogs. 2025. Available from: https://veterinaryclinicaltrials.org/study/VCT24005829 [Last accessed on 6 Jun 2026].
7. Leblanc AK, Mazcko CN, Cherukuri A, et al. Adjuvant sirolimus does not improve outcome in pet dogs receiving standard-of-care therapy for appendicular osteosarcoma: a prospective, randomized trial of 324 dogs. Clin Cancer Res. 2021;27:3005-16.
9. Mason NJ, Gnanandarajah JS, Engiles JB, et al. Immunotherapy with a HER2-targeting Listeria induces HER2-specific immunity and demonstrates potential therapeutic effects in a phase I trial in canine osteosarcoma. Clin Cancer Res. 2016;22:4380-90.
10. Mason NJ. Comparative immunology and immunotherapy of canine osteosarcoma. Adv Exp Med Biol. 2020;1258:199-221.
11. Smeland S, Bielack SS, Whelan J, et al. Survival and prognosis with osteosarcoma: outcomes in more than 2000 patients in the EURAMOS-1 (European and American Osteosarcoma Study) cohort. Eur J Cancer. 2019;109:36-50.
12. Aljubran A, Griffin A, Pintilie M, Blackstein M. Osteosarcoma in adolescents and adults: survival analysis with and without lung metastases. Ann Oncol. 2009;20:1136-41.
13. Savage SA, Mirabello L, Wang Z, et al. Genome-wide association study identifies two susceptibility loci for osteosarcoma. Nat Genet. 2013;45:799-803.
14. Karlsson EK, Sigurdsson S, Ivansson E, et al. Genome-wide analyses implicate 33 loci in heritable dog osteosarcoma, including regulatory variants near CDKN2A/B. Genome Biol. 2013;14:R132.
15. Jiang Y, Wang J, Sun M, et al. Multi-omics analysis identifies osteosarcoma subtypes with distinct prognosis indicating stratified treatment. Nat Commun. 2022;13:7207.
16. Simpson S, Rizvanov AA, Jeyapalan JN, De Brot S, Rutland CS. Canine osteosarcoma in comparative oncology: molecular mechanisms through to treatment discovery. Front Vet Sci. 2022;9:965391.
17. Sakthikumar S, Elvers I, Kim J, et al. SETD2 is recurrently mutated in whole-exome sequenced canine osteosarcoma. Cancer Res. 2018;78:3421-31.
18. Espejo JVI, De Noon S, Trevers K, et al. Ongoing chromothripsis underpins osteosarcoma genome complexity and clonal evolution. Cell. 2025;188:352-70.e22.
19. McCarthy EF. The toxins of William B. Coley and the treatment of bone and soft-tissue sarcomas. Iowa Orthop J. 2006;26:154-8.
20. Lascelles BDX, Dernell WS, Correa MT, et al. Improved survival associated with postoperative wound infection in dogs treated with limb-salvage surgery for osteosarcoma. Ann Surg Oncol. 2005;12:1073-83.
21. Liptak JM, Dernell WS, Ehrhart N, Lafferty MH, Monteith GJ, Withrow SJ. Cortical allograft and endoprosthesis for limb-sparing surgery in dogs with distal radial osteosarcoma: a prospective clinical comparison of two different limb-sparing techniques. Vet Surg. 2006;35:518-33.
22. Hans EC, Pinard C, Van Nimwegen SA, et al. Effect of surgical site infection on survival after limb amputation in the curative-intent treatment of canine appendicular osteosarcoma: a Veterinary Society of Surgical Oncology retrospective study. Vet Surg. 2018;47:E88-96.
23. Jeys LM, Grimer RJ, Carter SR, Tillman RM, Abudu A. Post operative infection and increased survival in osteosarcoma patients: are they associated? Ann Surg Oncol. 2007;14:2887-95.
24. Wustefeld-Janssens BG, Séguin B, Ehrhart NP, Worley DR. Analysis of outcome in dogs that undergo secondary amputation as an end-point for managing complications related to limb salvage surgery for treatment of appendicular osteosarcoma. Vet Comp Oncol. 2019;18:84-91.
25. Patkar S, Mannheimer J, Harmon SA, et al. Large-scale comparative analysis of canine and human osteosarcomas uncovers conserved clinically relevant tumor microenvironment subtypes. Clin Cancer Res. 2024;30:5630-42.
26. Withers SS, Skorupski KA, York D, et al. Association of macrophage and lymphocyte infiltration with outcome in canine osteosarcoma. Vet Comp Oncol. 2018;17:49-60.
27. Chen DS, Mellman I. Oncology meets immunology: the cancer-immunity cycle. Immunity. 2013;39:1-10.
28. Galon J, Bruni D. Approaches to treat immune hot, altered and cold tumours with combination immunotherapies. Nat Rev Drug Discovery. 2019;18:197-218.
29. Corrales L, Matson V, Flood B, Spranger S, Gajewski TF. Innate immune signaling and regulation in cancer immunotherapy. Cell Res. 2016;27:96-108.
30. Joffre OP, Segura E, Savina A, Amigorena S. Cross-presentation by dendritic cells. Nat Rev Immunol. 2012;12:557-69.
31. Miwa S, Shirai T, Yamamoto N, et al. Current and emerging targets in immunotherapy for osteosarcoma. J Oncol. 2019;2019:1-8.
32. Owen L, Bostock D. Effects of intravenous BCG in normal dogs and in dogs with spontaneous osteosarcoma. Eur J Cancer. 1974;10:775-80.
33. Owen LN, Bostock DE, Lavelle RB. Studies on chemotherapy and immunotherapy in canine lymphosarcoma and osteosarcoma. Bibl Haematol. 1975;43:522-3.
34. Amouzegar A, Chelvanambi M, Filderman J, Storkus W, Luke J. STING agonists as cancer therapeutics. Cancers. 2021;13:2695.
35. Li B, Zhang C, Xu X, Shen Q, Luo S, Hu J. Manipulating the cGAS-STING axis: advancing innovative strategies for osteosarcoma therapeutics. Front Immunol. 2025;16:1539396.
36. Kraitchman DL. Canine osteosarcoma clinical trial. 2025. Available from: https://veterinaryclinicaltrials.org/study/VCT20005123 [Last accessed on 6 Jun 2026].
37. Doucet M, Glavaris SA, Phillips M, Kulp E. Abstract B054: Intratumoral injection with stimulator of interferon genes (STING) agonist increases T- and B-cell infiltrates in canine osteosarcoma. American Association of Cancer Research, Advances in Pediatric Cancer Research; 2024.
38. Olin MR, Ampudia-Mesias E, Pennell CA, et al. Treatment combining CD200 immune checkpoint inhibitor and tumor-lysate vaccination after surgery for pet dogs with high-grade glioma. Cancers. 2019;11:137.
39. Fan T. Autologous cancer vaccine with checkpoint inhibitor for treatment of canine osteosarcoma. 2025. Available from: https://veterinaryclinicaltrials.org/study/VCT25005864 [Last accessed on 6 Jun 2026].
40. Marconato L, Melacarne A, Aralla M, et al. A target animal effectiveness study on adjuvant peptide-based vaccination in dogs with non-metastatic appendicular osteosarcoma undergoing amputation and chemotherapy. Cancers. 2022;14:1347.
41. Flint AF, U'ren L, Legare ME, Withrow SJ, Dernell W, Hanneman WH. Overexpression of the erbB-2 proto-oncogene in canine osteosarcoma cell lines and tumors. Vet Pathol. 2004;41:291-6.
42. Cao JW, Lake J, Impastato R, et al. Targeting osteosarcoma with canine B7-H3 CAR T cells and impact of CXCR2 Co-expression on functional activity. Cancer Immunol Immunother. 2024;73:77.
43. Zhang S, Black RG, Kohli K, et al. B7-H3 specific CAR T cells for the naturally occurring, spontaneous canine sarcoma model. Mol Cancer Ther. 2022;21:999-1009.
44. De Vico G, Martano M, Maiolino P, Carella F, Leonardi L. Expression of transferrin receptor-1 (TFR-1) in canine osteosarcomas. Vet Med Sci. 2020;6:272-6.
45. Matsuyama A, Wood GA, Speare R, Schott CR, Mutsaers AJ. Prognostic significance of the urokinase plasminogen activator system in tissue and serum of dogs with appendicular osteosarcoma. PLoS ONE. 2022;17:e0273811.
46. Milner RJ, Chimura N, Bowles KD, Salute M. Abstract A29: Differential expression of the gangliosides GD3 and GD2 in canine and human osteosarcoma cell lines: an immunotherapy target. Cancer Immunol Res. 2015;3:A29.
47. Fu Y, Yu J, Liatsou I, et al. Anti-GD2 antibody for radiopharmaceutical imaging of osteosarcoma. Eur J Nucl Med Mol Imaging. 2022;49:4382-93.
48. Shahabi V, Seavey MM, Maciag PC, Rivera S, Wallecha A. Development of a live and highly attenuated Listeria monocytogenes-based vaccine for the treatment of Her2/neu-overexpressing cancers in human. Cancer Gene Ther. 2010;18:53-62.
49. Seavey MM, Pan Z, Maciag PC, et al. A novel human her-2/neu chimeric molecule expressed by Listeria monocytogenes can elicit potent HLA-A2 restricted CD8-positive T cell responses and impact the growth and spread of her-2/neu-positive breast tumors. Clin Cancer Res. 2009;15:924-32.
50. Mason NJ, Selmic L, Ruple A, et al. Immunological responses and clinical outcomes in dogs with osteosarcoma receiving standard therapy and a Listeria vaccine expressing HER2. Mol Ther. 2025;33:1674-86.
51. Musser ML, Berger EP, Tripp CD, Clifford CA, Bergman PJ, Johannes CM. Safety evaluation of the canine osteosarcoma vaccine, live Listeria vector. Vet Comp Oncol. 2020;19:92-8.
52. Quispe-Tintaya W, Chandra D, Jahangir A, et al. Nontoxic radioactive isteriaat is a highly effective therapy against metastatic pancreatic cancer. Proc Natl Acad Sci USA. 2013;110:8668-73.
53. Doyle HA, Gee RJ, Masters TD, et al. Vaccine-induced ErbB (EGFR/HER2)-specific immunity in spontaneous canine cancer. Transl Oncol. 2021;14:101205.
54. Milner R. Vaccine study for dogs with appendicular osteosarcoma. 2025. Available from: https://veterinaryclinicaltrials.org/study/VCT24005824 [Last accessed on 6 Jun 2026].
55. Shaik R, Royyala SA, Inapanuri B, Durgam A, Khan H, Unnisa A. Tumor infiltration therapy: from FDA approval to next-generation approaches. Clin Exp Med. 2025;25:254.
56. Ammons DT, Harris RA, Chow L, Dow S. Characterization of canine tumor-infiltrating leukocyte transcriptomic signatures reveals conserved expression patterns with human osteosarcoma. Cancer Immunol Immunother. 2025;74:105.
57. Dudley ME, Wunderlich J, Nishimura MI, et al. Adoptive transfer of cloned melanoma-reactive T lymphocytes for the treatment of patients with metastatic melanoma. J Immunother. 2001;24:363-73.
58. Chesney J, Lewis KD, Kluger H, et al. Efficacy and safety of lifileucel, a one-time autologous tumor-infiltrating lymphocyte (TIL) cell therapy, in patients with advanced melanoma after progression on immune checkpoint inhibitors and targeted therapies: pooled analysis of consecutive cohorts of the C-144-01 study. J Immunother Cancer. 2022;10:e005755.
59. Foos KM, Pandey V, Jennings MW, Powell DJ, Mason NJ. Generation of functional canine TIL products for solid tumors. Front Immunol. 2026;17:1810955.
60. Forsberg EMV, Riise R, Saellström S, et al. Treatment with anti-HER2 chimeric antigen receptor tumor-infiltrating lymphocytes (CAR-TILs) is safe and associated with antitumor efficacy in mice and companion dogs. Cancers. 2023;15:648.
61. Sarnaik AA, Hamid O, Khushalani NI, et al. Lifileucel, a tumor-infiltrating lymphocyte therapy, in metastatic melanoma. J Clin Oncol. 2021;39:2656-66.
62. Dias JNR, André AS, Aguiar SI, Gil S, Tavares L, Aires-da-Silva F. Immunotherapeutic strategies for canine lymphoma: changing the odds against non-hodgkin lymphoma. Front Vet Sci. 2021;8:621758.
63. Reyes NaB J, Wahaus T, Wright Z, et al. Adoptive cell therapy with chemotherapy improves canine osteosarcoma outcomes compared to standard of care chemotherapy. ACVIM Forum; 2025; Louisville, Kentucky. Available from: https://academic.oup.com/jvim/article/39/6/jvim70258/8474771#552954844 [Last accessed on 10 Jul 2026].
64. Huber F, Bassani-Sternberg M. Defects in antigen processing and presentation: mechanisms, immune evasion and implications for cancer vaccine development. Nat Rev Immunol. 2025;26:23-34.
65. Hong M, Clubb JD, Chen YY. Engineering CAR-T cells for next-generation cancer therapy. Cancer Cell. 2020;38:473-88.
66. Zugasti I, Espinosa-Aroca L, Fidyt K, et al. CAR-T cell therapy for cancer: current challenges and future directions. Sig Transduct Target Ther. 2025;10:210.
67. Kawalekar OU, O’connor RS, Fraietta JA, et al. Distinct signaling of coreceptors regulates specific metabolism pathways and impacts memory development in CAR T cells. Immunity. 2016;44:380-90.
68. Hegde M, Navai S, Derenzo C, et al. Autologous HER2-specific CAR T cells after lymphodepletion for advanced sarcoma: a phase 1 trial. Nat Cancer. 2024;5:880-94.
69. Epperly R, Gottschalk S, Derenzo C. CAR T cells redirected to B7-H3 for pediatric solid tumors: current status and future perspectives. EJC Paediatr Oncol. 2024;3:100160.
70. Mata M, Vera JF, Gerken C, et al. Toward immunotherapy with redirected T cells in a large animal model: ex vivo activation, expansion, and genetic modification of canine T cells. J Immunother. 2014;37:407-15.
71. Wang L, Zhang Q, Chen W, et al. B7-H3 is overexpressed in patients suffering osteosarcoma and associated with tumor aggressiveness and metastasis. PLoS ONE. 2013;8:e70689.
72. Sotillo E, Barrett DM, Black KL, et al. Convergence of acquired mutations and alternative splicing of CD19 enables resistance to CART-19 immunotherapy. Cancer Discovery. 2015;5:1282-95.
73. Garcia-Robledo JE, Cabrera-Salcedo S, Brandauer AM, et al. Engineering the next generation of CAR T- cells: precision modifications, logic gates and universal strategies to overcome exhaustion and tumor resistance. Front Oncol. 2026;15:1698442.
74. Liu Y, Wang G, Chai D, Dang Y, Zheng J, Li H. iNKT: a new avenue for CAR-based cancer immunotherapy. Transl Oncol. 2022;17:101342.
75. Rotolo A, Whelan EC, Atherton MJ, et al. Unedited allogeneic iNKT cells show extended persistence in MHC-mismatched canine recipients. Cell Rep Med. 2023;4:101241.
76. Mujal AM, Delconte RB, Sun JC. Natural killer cells: from innate to adaptive features. Annu Rev Immunol. 2021;39:417-47.
77. Razmara AM, Gingrich AA, Toedebusch CM, et al. Improved characterization and translation of NK cells for canine immunotherapy. Front Vet Sci. 2024;11:1336158.
78. Razmara AM, Farley LE, Harris RM, et al. Preclinical evaluation and first-in-dog clinical trials of PBMC-expanded natural killer cells for adoptive immunotherapy in dogs with cancer. J Immunother Cancer. 2024;12:e007963.
79. Canter RJ, Grossenbacher SK, Foltz JA, et al. Radiotherapy enhances natural killer cell cytotoxicity and localization in pre-clinical canine sarcomas and first-in-dog clinical trial. J Immunother Cancer. 2017;5:98.
80. Judge SJ, Yanagisawa M, Sturgill IR, et al. Blood and tissue biomarker analysis in dogs with osteosarcoma treated with palliative radiation and intra-tumoral autologous natural killer cell transfer. PLoS ONE. 2020;15:e0224775.
81. Rebhun RB, York D, Cruz SM, et al. Inhaled recombinant human IL-15 in dogs with naturally occurring pulmonary metastases from osteosarcoma or melanoma: a phase 1 study of clinical activity and correlates of response. J Immunother Cancer. 2022;10:e004493.
82. Razmara AM, Lammers M, Judge SJ, et al. Single cell atlas of canine natural killer cells identifies distinct circulating and tissue resident gene profiles. Front Immunol. 2025;16:1571085.
83. Delfanti G, Cortesi F, Perini A, et al. TCR-engineered iNKT cells induce robust antitumor response by dual targeting cancer and suppressive myeloid cells. Sci Immunol. 2022;7:eabn6563.
84. Mason N. Cell therapy for metastatic osteosarcoma. Available from: https://veterinaryclinicaltrials.org/study/VCT24005853 [Last accessed on 6 Jun 2026].
85. Mannheimer JD, Tawa G, Gerhold D, et al. Transcriptional profiling of canine osteosarcoma identifies prognostic gene expression signatures with translational value for humans. Commun Biol. 2023;6:856.
86. Scott MC, Temiz NA, Sarver AE, et al. Comparative transcriptome analysis quantifies immune cell transcript levels, metastatic progression, and survival in osteosarcoma. Cancer Res. 2018;78:326-37.
87. Beck JA, Garg A, Church S, Mazcko C, Leblanc AK. Spatial transcriptomics advances the use of canine patients in cancer research: analysis of osteosarcoma-bearing pet dogs enrolled in a clinical trial. Clin Cancer Res. 2025;31:2957-62.
88. Eigenbrood J, Wong N, Mallory P, et al. Spatial profiling identifies regionally distinct microenvironments and targetable immunosuppressive mechanisms in pediatric osteosarcoma pulmonary metastases. Cancer Res. 2025;85:2320-37.
89. Liu G, Rui W, Zheng H, et al. CXCR2-modified CAR-T cells have enhanced trafficking ability that improves treatment of hepatocellular carcinoma. Eur J Immunol. 2020;50:712-24.
90. Langsten KL, Kim JH, Sarver AL, Dewhirst M, Modiano JF. Comparative approach to the temporo-spatial organization of the tumor microenvironment. Front Oncol. 2019;9:1185.
92. Qiu G, Tang Y, Zuo J, Wu H, Wan Y. Deciphering spatially confined immune evasion niches in osteosarcoma with 3-D spatial transcriptomics: a literature review. Front Oncol. 2025;15:1640645.
93. Regan DP, Chow L, Das S, et al. Losartan blocks osteosarcoma-elicited monocyte recruitment, and combined with the kinase inhibitor toceranib, exerts significant clinical benefit in canine metastatic osteosarcoma. Clin Cancer Res. 2022;28:662-76.
94. Levy A, Morel D, Texier M, et al. Monocyte-lineage tumor infiltration predicts immunoradiotherapy response in advanced pretreated soft-tissue sarcoma: phase 2 trial results. Sig Transduct Target Ther. 2025;10:103.
95. Buddingh EP, Kuijjer ML, Duim RA, et al. Tumor-infiltrating macrophages are associated with metastasis suppression in high-grade osteosarcoma: a rationale for treatment with macrophage activating agents. Clin Cancer Res. 2011;17:2110-9.
96. Gomez-Brouchet A, Illac C, Gilhodes J, et al. CD163-positive tumor-associated macrophages and CD8-positive cytotoxic lymphocytes are powerful diagnostic markers for the therapeutic stratification of osteosarcoma patients: an immunohistochemical analysis of the biopsies fromthe French OS2006 phase 3 trial. OncoImmunology. 2017;6:e1331193.
97. Kurzman ID, MacEwen EG, Rosenthal RC, et al. Adjuvant therapy for osteosarcoma in dogs: results of randomized clinical trials using combined liposome-encapsulated muramyl tripeptide and cisplatin. Clin Cancer Res. 1995;1:1595-601.
98. Meyers PA, Schwartz CL, Krailo M, et al. Osteosarcoma: a randomized, prospective trial of the addition of ifosfamide and/or muramyl tripeptide to cisplatin, doxorubicin, and high-dose methotrexate. J Clin Oncol. 2005;23:2004-11.
99. Palmerini E, Meazza C, Tamburini A, et al. Is there a role for mifamurtide in nonmetastatic high-grade osteosarcoma? Results From the Italian Sarcoma Group (ISG/OS-2) and Spanish Sarcoma Group (GEIS-33) trials. J Clin Oncol. 2025;43:3113-22.
100. Kondo H, Tazawa H, Fujiwara T, et al. Osteosarcoma cell-derived CCL2 facilitates lung metastasis via accumulation of tumor-associated macrophages. Cancer Immunol Immunother. 2025;74:193.
101. Losartan + Sunitinib in treatment of osteosarcoma; 2019. Available from: https://clinicaltrials.gov/study/NCT03900793 [Last accessed on 6 Jun 2026].
102. London C, Regan D, Chow L, et al. 840 triple-drug oral immunotherapy targeting myeloid cells for treatment of metastatic osteosarcoma evaluated in spontaneous canine model. J ImmunoTher Cancer. 2022;10.
103. Pittet MJ, Michielin O, Migliorini D. Clinical relevance of tumour-associated macrophages. Nat Rev Clin Oncol. 2022;19:402-21.
104. Kudo A, Kamo S, Yamauchi A, et al. Exploring the effect of canine cancer-associated fibroblasts on T cell dynamics through the CXCL12/CXCR4 axis modulated by TGF-β1. Sci Rep. 2025;15:31050.
105. Bracigliano A, Clemente O, Peddio A, et al. FAP-α in soft tissue and bone sarcomas: a new potential diagnostic and therapeutic biomarker in the era of precision medicine. Crit Rev Oncol Hematol. 2025;215:104852.
106. Ammons DT, Hopkins LS, Cronise KE, Kurihara J, Regan DP, Dow S. Single-cell RNA sequencing reveals the cellular and molecular heterogeneity of treatment-naïve primary osteosarcoma in dogs. Commun Biol. 2024;7:496.
107. Beer P, Pauli C, Haberecker M, et al. Cross-species evaluation of fibroblast activation protein alpha as potential imaging target for soft tissue sarcoma: a comparative immunohistochemical study in humans, dogs, and cats. Front Oncol. 2023;13:1210004.
108. Regan D. Clinical testing of canine T cells engineered to target osteosarcoma and soft tissue sarcoma in combination with oral immunotherapy. Flint Animal Cancer Center: Colorado State University; 2025. Available from: https://studypages.com/s/clinical-testing-of-canine-t-cells-engineered-to-target-osteosarcoma-and-soft-tissue-sarcoma-in-combination-with-oral-immunotherapy-737440/ [Last accessed on 6 Jun 2026].
109. Yoshimoto S, Chester N, Xiong A, et al. Development and pharmacokinetic assessment of a fully canine anti-PD-1 monoclonal antibody for comparative translational research in dogs with spontaneous tumors. mAbs. 2023;15:2287250.
110. Mason NJ, Chester N, Xiong A, et al. Development of a fully canine anti-canine CTLA4 monoclonal antibody for comparative translational research in dogs with spontaneous tumors. mAbs. 2021;13:2004638.
111. Maekawa N, Konnai S, Watari K, et al. Development of caninized anti-CTLA-4 antibody as salvage combination therapy for anti-PD-L1 refractory tumors in dogs. Front Immunol. 2025;16:1570717.
112. Maekawa N, Konnai S, Nishimura M, et al. PD-L1 immunohistochemistry for canine cancers and clinical benefit of anti-PD-L1 antibody in dogs with pulmonary metastatic oral malignant melanoma. NPJ Precis Onc. 2021;5:10.
113. Cascio MJ, Whitley EM, Sahay B, et al. Canine osteosarcoma checkpoint expression correlates with metastasis and T-cell infiltrate. Vet Immunol Immunopathol. 2021;232:110169.
114. Song M, Cho J, Park H, et al. Discovery and functional characterization of canine PD-L1-targeted antibodies for evaluating antitumor efficacy in a canine osteosarcoma xenograft model. Sci Rep. 2025;15:7574.
115. Milner R, Sayour E, Ligon J. Canine RNA-nanoparticle vaccine combined with anti-PD1 drug against osteosarcoma for canine patients (currently enrolling). University of Florida College of Veterinary Medicine; 2025. Available from: https://research.vetmed.ufl.edu/research-programs/clinical-trials/small-animal/mrna-vaccine-study-for-dogs-with-appendicular-osteosarcoma-currently-enrolling/?utm_source=chatgpt.com [Last accessed on 6 Jun 2026].
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Special Topic
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].