


fig2
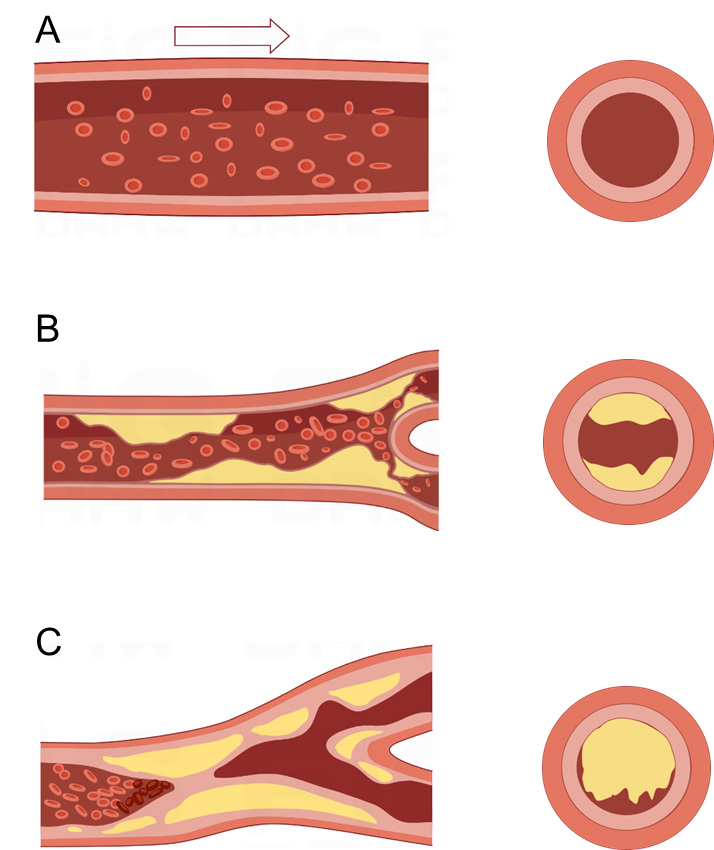
Figure 2. Diagram illustrating the progression of atherosclerosis and plaque rupture. (A) Normal artery: The arterial wall exhibits an intact endothelium and well-defined intima, media, and adventitia layers. There is no lipid accumulation or inflammatory cell infiltration, and vascular smooth muscle cells (VSMCs) maintain a contractile phenotype ensuring vessel integrity and function; (B) Early atherosclerosis: Endothelial injury and dysfunction lead to increased intimal permeability, allowing the deposition and oxidation of low-density lipoprotein particles in the subendothelial space. This results in recruitment of monocytes and their differentiation into macrophages, which take up oxidized LDL to form foam cells. The accumulation of foam cells and inflammatory cells initiates the formation of fatty streaks and early plaques within the intimal layer, thereby causing luminal narrowing. Note that plaques are localized within the intima/subendothelial space and do not protrude freely into the vessel lumen. VSMCs proliferate and migrate from the media to the intima, promoting fibrous cap formation; (C) Advanced plaque and rupture: The plaque enlarges, characterized by a large necrotic lipid core surrounded by a fibrous cap composed mainly of collagen and VSMCs. Inflammatory macrophages secrete matrix metalloproteinases (MMPs), which degrade extracellular matrix components within the fibrous cap, causing thinning and weakening of the cap. Mechanical forces and inflammatory stimuli promote plaque rupture or erosion, exposing thrombogenic material to circulating blood. This triggers platelet aggregation and thrombus formation, which can acutely occlude the arterial lumen, leading to ischemic events. The figure illustrates the process of fibrous cap thinning and subsequent fibrous cap rupture with thrombus formation. LDL: Low-density lipoprotein.





