


Association of urinary nitrate with blood pressure and cardiovascular outcomes in hypertensive population
 0
0 
Abstract
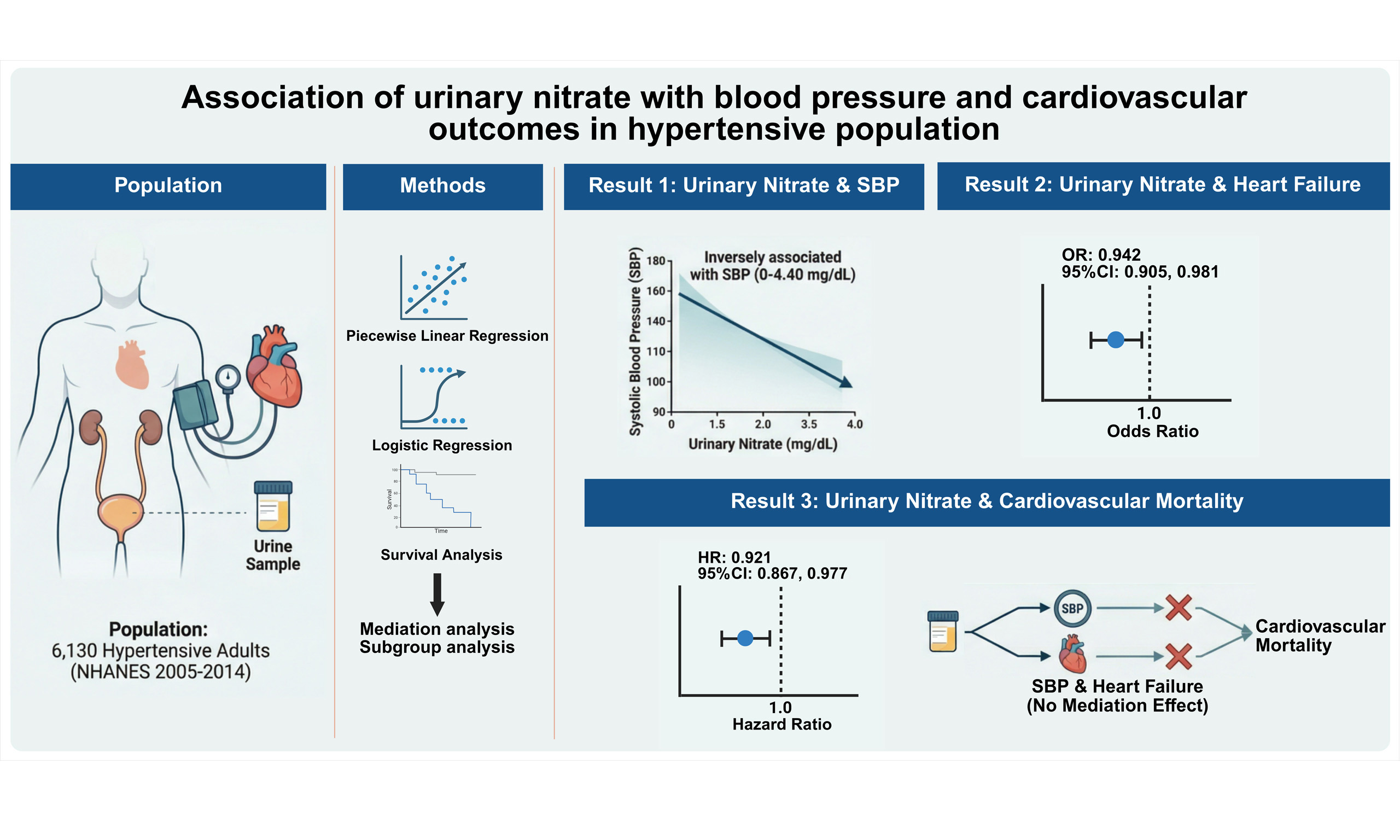
Aim: The protective effects of inorganic nitrate in hypertensive patients remain uncertain. Therefore, this study investigated the associations of urinary nitrate with blood pressure, the prevalence of cardiovascular disease (CVD), and cardiovascular mortality among the hypertensive population.
Methods: A total of 6,130 hypertensive adults from the 2005-2014 NHANES (The National Health and Nutrition Examination Survey) were included. Piecewise linear regression, logistic regression, and Cox proportional hazards regression models were performed to evaluate the associations of urinary nitrate with blood pressure, CVD prevalence, and cardiovascular mortality, respectively. Mediation and subgroup analyses were further conducted to explore the potential mechanisms and the consistency of the association between urinary nitrate and cardiovascular mortality.
Results: Within the range of 0-4.40 mg/dL, an inverse linear correlation between urinary nitrate and systolic blood pressure (SBP) was observed [β = -0.60; 95% confidence interval (95%CI): -0.99 to -0.21; P < 0.001]. Higher urinary nitrate levels were associated with a reduced prevalence of heart failure [odds ratio (OR): 0.942; 95%CI: 0.905 to 0.981; P = 0.004] and lower cardiovascular mortality [hazard ratio (HR): 0.921; 95%CI, 0.867 to 0.977; P = 0.006]. Mediation analyses indicated that neither SBP nor baseline heart failure mediated the association between urinary nitrate and cardiovascular mortality. Subgroup analyses showed that the inverse association between urinary nitrate and cardiovascular mortality was modified by the presence of coronary heart disease.
Conclusion: Among hypertensive individuals, higher urinary nitrate levels were associated with lower SBP, heart failure prevalence, and cardiovascular mortality. These findings suggest that urinary nitrate may serve as a potential biomarker for cardiovascular risk stratification.
Keywords
INTRODUCTION
Preventing cardiovascular disease (CVD) and reducing cardiovascular mortality are global research priorities. Between 2007 and 2017, total fatalities attributed to CVD increased by 21.1% worldwide. Specifically, the age-adjusted death rate for hypertension-related CVD rose from 18.3 to 23.0 per 100,000 during this period[1,2]. Hypertension remains the primary risk factor for CVD and multiple randomized controlled studies have unequivocally validated the efficacy of blood pressure (BP) reduction in averting CVD occurrences[3]. Therefore, identifying strategies to prevent elevated BP is essential to alleviate the burden of BP-related CVD.
Nitric oxide (NO) is critical for mediating vascular dilation, improving endothelial function, and maintaining vascular homeostasis[4]. Dietary inorganic nitrate serves as an exogenous source of NO. It is reduced by commensal bacteria in the oral cavity and gastrointestinal tract through various enzymatic and non-enzymatic reactions[4,5]. Extensive evidence highlights the benefits of nitrate intake for blood pressure regulation and the reduction of CVD risk[6-12]. Specifically, large-scale research has associated urinary nitrate with a lower prevalence of hypertension and stroke, as well as reduced cardiovascular mortality[13]. However, most studies have focused on healthy individuals or the general population. Whether these protective effects remain significant specifically in hypertensive individuals has yet to be established.
This study employed urinary nitrate as a biomarker of nitrate exposure to elucidate the associations of urinary nitrate with blood pressure, prevalence of CVD and cardiovascular mortality in the hypertensive population. A preliminary version of this study was previously published as a preprint[14].
MATERIAL AND METHODS
Study population
The National Health and Nutrition Examination Survey (NHANES) is an ongoing survey approved by the Institutional Review Boards of the National Center for Health Statistics and the Centers for Disease Control and Prevention. NHANES utilizes a complex survey methodology to provide a nationally representative sample of the U.S. civilian population. Linked with the National Death Index (NDI), the database enables prospective mortality follow-up[15]. Written informed consent was obtained from all participants under protocols #2005-06 (2005-2010) and #2011-17 (2011-2014). The initial population included 6,507 hypertensive adults (aged ≥ 20 years) from the 2005-2014 survey cycles, all of whom underwent urinary nitrate testing. After excluding participants with missing data on BP, comorbidities and follow-up, the final analytical sample comprised 6,130 individuals. Hypertension was defined as meeting at least one of the following criteria: self-reported physician diagnosis, use of ≥ 2 antihypertensive medications (including combination preparations), or a mean systolic blood pressure (SBP) ≥ 140 mmHg or mean diastolic blood pressure (DBP) ≥ 90 mmHg (based on the average of three measurements). This threshold is consistent with the Joint National Committee (JNC) 7 guidelines, thereby aligning the analysis with the clinical standards contemporary to the survey period. Mortality data were obtained through prospective follow-up by linking participant records to the NDI and official death certificates.
Measurement of urinary nitrate concentration
Urinary nitrate concentrations were measured in spot urine samples. Urine specimens were properly stored at -20 °C until shipment to the National Center for Environmental Health for testing. Nitrate levels were quantified by ion chromatography with tandem mass spectrometry (IC-MS/MS). Detailed protocols for specimen collection and processing are described in the NHANES Laboratory/Medical Technologists Procedures Manual[16].
Outcome
In this study, primary outcomes consisted of BP and cardiovascular mortality. Secondary outcomes were the prevalence of CVD, including angina pectoris, myocardial infarction (MI), coronary heart disease (CHD) and heart failure (HF). Mortality status was determined through linkage with the NDI for the 1999-2014 NHANES cohorts, providing follow-up data through December 31, 2015. Follow-up duration was defined as the interval from survey participation to either the date of death or December 31, 2015. The cause-specific death categories were based on the ICD-10 codes, with cardiovascular death codes including I00-I09, I11, I13, I20-I51 and I60-I69. For a more detailed description of the methodology, please refer to the online source[17].
Covariates
Demographic and physical examination data were collected, including sex, age, race (Mexican American, Other Hispanic, Non-Hispanic White, Non-Hispanic Black and Other Race), poverty income ratio (PIR), body mass index (BMI), SBP, and DBP. Smoking and drinking habits were categorized as current, former and never. Dietary factors, such as the intake of processed meat, sodium, and dark-green vegetables, were adjusted for as covariates. The major comorbidities included angina pectoris, MI, CHD, HF, stroke, diabetes and cancer. Diabetes was defined as meeting at least one of the following criteria: a self-reported diagnosis; glycated hemoglobin (HbA1c) ≥ 6.5%; fasting plasma glucose ≥ 7.0 mmol/L; random plasma glucose
Statistical analyses
The study population was stratified by urinary nitrate tertiles to describe baseline characteristics. Continuous variables are presented as weighted means (standard errors), while categorical variables are reported as unweighted counts (weighted percentages). Generalized additive models (GAMs) were employed to visualize the dose-response relationships between urinary nitrate and blood pressure. Linear association was analyzed using standard linear regression, whereas potential non-linearity was explored using two-piecewise linear regression. The optimal turning point was identified through a grid search to maximize the likelihood function. A log-likelihood ratio test was subsequently performed to compare the linear model with the piecewise model, with P < 0.05 indicating the presence of a threshold effect. Logistic regression and Cox proportional hazards models were utilized to evaluate the associations of urinary nitrate with CVD prevalence and cardiovascular mortality, respectively. Furthermore, subgroup and mediation analyses were conducted to explore potential interactions and mediating pathways. Mediation analysis was performed within a causal mediation framework to evaluate the mediating effects of mediators on the association between urinary nitrate and cardiovascular outcomes. The “mediation” package in R was employed. All analyses followed NHANES data analysis guidelines, incorporating sample weights. Given that urinary nitrate was measured in a specific laboratory sub-sample, the corresponding sub-sample weights were applied to ensure national representativeness. Missing values were addressed via multiple imputation. All statistical analyses were performed using R software (version 4.5.2; R Foundation for Statistical Computing, Vienna, Austria) and EmpowerStats (X&Y Solutions, Inc., Boston, MA). A two-sided P < 0.05 was considered statistically significant.
RESULTS
Descriptive analysis
A total of 6,130 participants were included in the final analysis [Figure 1]. The baseline characteristics are summarized in Table 1. The mean (standard deviation, SD) age was 56.85 (15.12) years, and 50.5% were men. Non-Hispanic Whites predominated, accounting for 71.3% of the population. The mean (SD) urinary nitrate concentration was 5.09 (4.34) mg/dL. Participants were stratified into tertiles based on urinary nitrate levels (T1, ≤ 2.82 mg/dL; T2, 2.82-5.52 mg/dL; T3, > 5.52 mg/dL). The T1 group had the lowest proportion of males. As urinary nitrate levels increased, upward trends were observed in the prevalence of alcohol consumption and tobacco use, alongside elevations in BMI and eGFR. Conversely, the mean age, SBP, and the proportion of participants with HF or stroke, as well as those using antihypertensive or lipid-lowering agents, decreased across the tertiles. The T3 group exhibited the lowest prevalence of stroke and cancer. No significant differences were observed in the proportions of CHD, MI, or diabetes among the three groups.
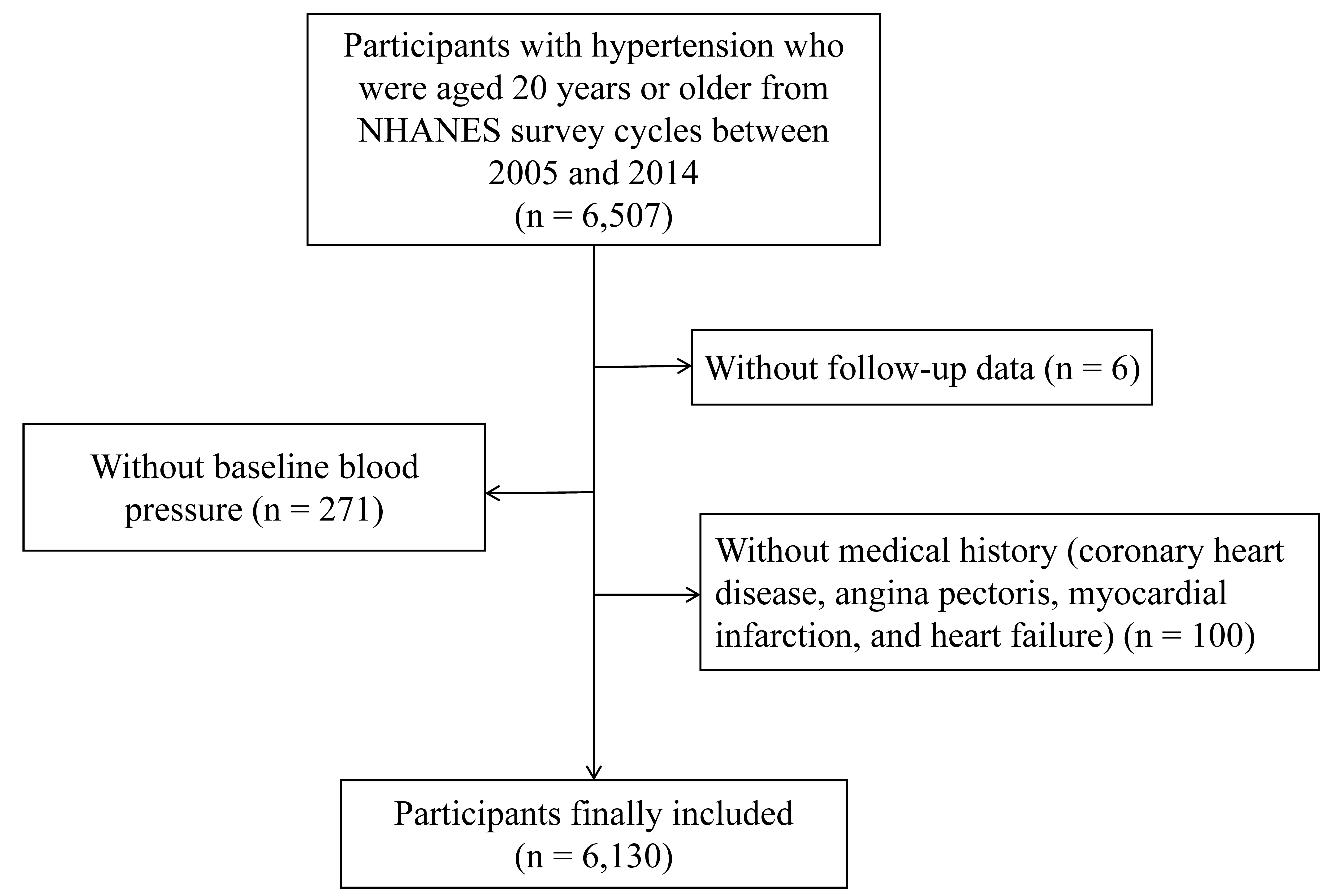
Figure 1. The flowchart of the study. NHANES: The national health and nutrition examination survey.
Weighted baseline characteristics of the study population
| Characteristic | Overall N = 6,130 | T1 (Lowest) N = 2,071 | T2 (Middle) N = 2,146 | T3 (Highest) N = 1,913 | P-value |
| Age, year | 56.85 (15.12) | 59.80 (15.11) | 57.36 (14.92) | 53.36 (14.63) | < 0.001 |
| Sex, n (%) | < 0.001 | ||||
| male | 3,119 (50.5%) | 882 (39.7%) | 1,166 (56.7%) | 1,071 (55.0%) | |
| Female | 3,011 (49.5%) | 1,189 (60.3%) | 980 (43.3%) | 842 (45.0%) | |
| Race, n (%) | 0.005 | ||||
| Mexican American | 784 (5.6%) | 259 (5.0%) | 291 (6.5%) | 234 (5.3%) | |
| Other Hispanic | 442 (3.8%) | 146 (3.4%) | 166 (4.5%) | 130 (3.6%) | |
| Non-Hispanic White | 2,979 (71.3%) | 1,042 (74.1%) | 1,009 (69.7%) | 928 (70.1%) | |
| Non-Hispanic Black | 1,594 (13.8%) | 522 (12.3%) | 588 (15.1%) | 484 (13.9%) | |
| Other | 331 (5.5%) | 102 (5.2%) | 92 (4.2%) | 137 (7.0%) | |
| BMI, kg/m2 | 30.63 (7.20) | 29.76 (6.69) | 30.82 (7.46) | 31.31 (7.33) | < 0.001 |
| PIR, n (%) | 0.062 | ||||
| ≤ 1.3 | 1,901 (21.8%) | 674 (22.5%) | 638 (21.4%) | 589 (21.4%) | |
| 1.3-3.5 | 2,409 (37.6%) | 846 (40.4%) | 841 (37.0%) | 722 (35.4%) | |
| ≥ 3.5 | 1,820 (40.7%) | 551 (37.1%) | 667 (41.7%) | 602 (43.2%) | |
| Smoking status, n (%) | < 0.001 | ||||
| Never | 3,017 (48.7%) | 1,099 (53.6%) | 1,054 (46.8%) | 864 (45.6%) | |
| Former | 1,935 (32.1%) | 688 (31.6%) | 700 (34.5%) | 547 (30.1%) | |
| Current | 1,178 (19.3%) | 284 (14.8%) | 392 (18.8%) | 502 (24.3%) | |
| Drinking status, n (%) | 0.001 | ||||
| Never | 933 (11.3%) | 371 (13.9%) | 334 (11.7%) | 228 (8.3%) | |
| Former | 1,044 (14.3%) | 356 (14.7%) | 374 (13.9%) | 314 (14.3%) | |
| Current | 4,153 (74.4%) | 1,344 (71.4%) | 1,438 (74.5%) | 1,371 (77.4%) | |
| SBP, mmHg | 133.03 (19.48) | 134.86 (21.19) | 132.99 (18.53) | 131.22 (18.44) | 0.005 |
| DBP, mmHg | 73.63 (13.47) | 72.10 (14.14) | 74.20 (13.15) | 74.59 (12.97) | < 0.001 |
| Angina pectoris, n (%) | 292 (4.3%) | 109 (4.6%) | 104 (4.9%) | 79 (3.5%) | 0.280 |
| CHD, n (%) | 455 (6.7%) | 164 (6.4%) | 167 (7.5%) | 124 (6.1%) | 0.490 |
| MI, n (%) | 469 (6.7%) | 184 (7.0%) | 155 (6.7%) | 130 (6.4%) | 0.900 |
| Stroke, n (%) | 436 (5.7%) | 181 (6.6%) | 147 (6.5%) | 108 (3.9%) | 0.011 |
| Diabetes, n (%) | 1,854 (25.2%) | 682 (25.1%) | 681 (27.1%) | 491 (23.4%) | 0.240 |
| HF, n (%) | 372 (4.9%) | 183 (6.4%) | 117 (5.3%) | 72 (3.0%) | 0.004 |
| Cancer, n (%) | 855 (15.0%) | 291 (14.9%) | 340 (17.7%) | 224 (12.3%) | 0.025 |
| HbA1c, % | 5.86 (1.04) | 5.87 (1.07) | 5.90 (1.10) | 5.81 (0.94) | 0.100 |
| Total cholesterol, mmol/L | 5.11 (1.13) | 5.17 (1.18) | 5.08 (1.08) | 5.08 (1.12) | 0.240 |
| eGFR, mL/min/1.73 m2 | 86.08 (21.41) | 81.06 (23.21) | 86.88 (20.85) | 90.32 (18.90) | < 0.001 |
| Urinary nitrate, mg/dL | 5.09 (4.34) | 1.72 (0.69) | 4.08 (0.77) | 9.51 (4.85) | < 0.001 |
| Processed meat intake, oz eq/day | 1.08 (1.93) | 0.99 (1.67) | 1.10 (1.89) | 1.14 (2.20) | 0.620 |
| Dark green vegetable intake, cup eq/day | 0.14 (0.42) | 0.11 (0.33) | 0.11 (0.41) | 0.20 (0.50) | < 0.001 |
| Dietary sodium intake (mg/day) | 3,427.80 (1,787.73) | 3,172.89 (1,629.49) | 3,499.75 (1,845.64) | 3,611.96 (1,851.27) | < 0.001 |
| Glucose-lowering medication, n (%) | 1,168 (16.1%) | 460 (16.8%) | 407 (16.2%) | 301 (15.2%) | 0.670 |
| Antihypertensive medication classes, n (%) | < 0.001 | ||||
| 0 | 2,117 (36.7%) | 581 (31.1%) | 725 (35.9%) | 811 (43.2%) | |
| 1 | 1,410 (23.3%) | 462 (24.5%) | 487 (23.1%) | 461 (22.3%) | |
| 2 | 1,455 (23.8%) | 531 (25.3%) | 528 (23.9%) | 396 (22.1%) | |
| ≥ 3 | 1,148 (16.2%) | 497 (19.1%) | 406 (17.1%) | 245 (12.5%) | |
| Lipid-lowering medication n (%) | 2,105 (34.3%) | 799 (37.9%) | 750 (33.3%) | 556 (31.7%) | 0.086 |
Urinary nitrate and blood pressure
As illustrated in Figure 2A, a nonlinear association between urinary nitrate and SBP was observed. After multivariable adjustment, a saturation effect was identified, with an optimal turning point of 4.40 mg/dL [95% confidence interval (95%CI), 3.68-5.25; log-likelihood ratio test P = 0.029]. Within the range of
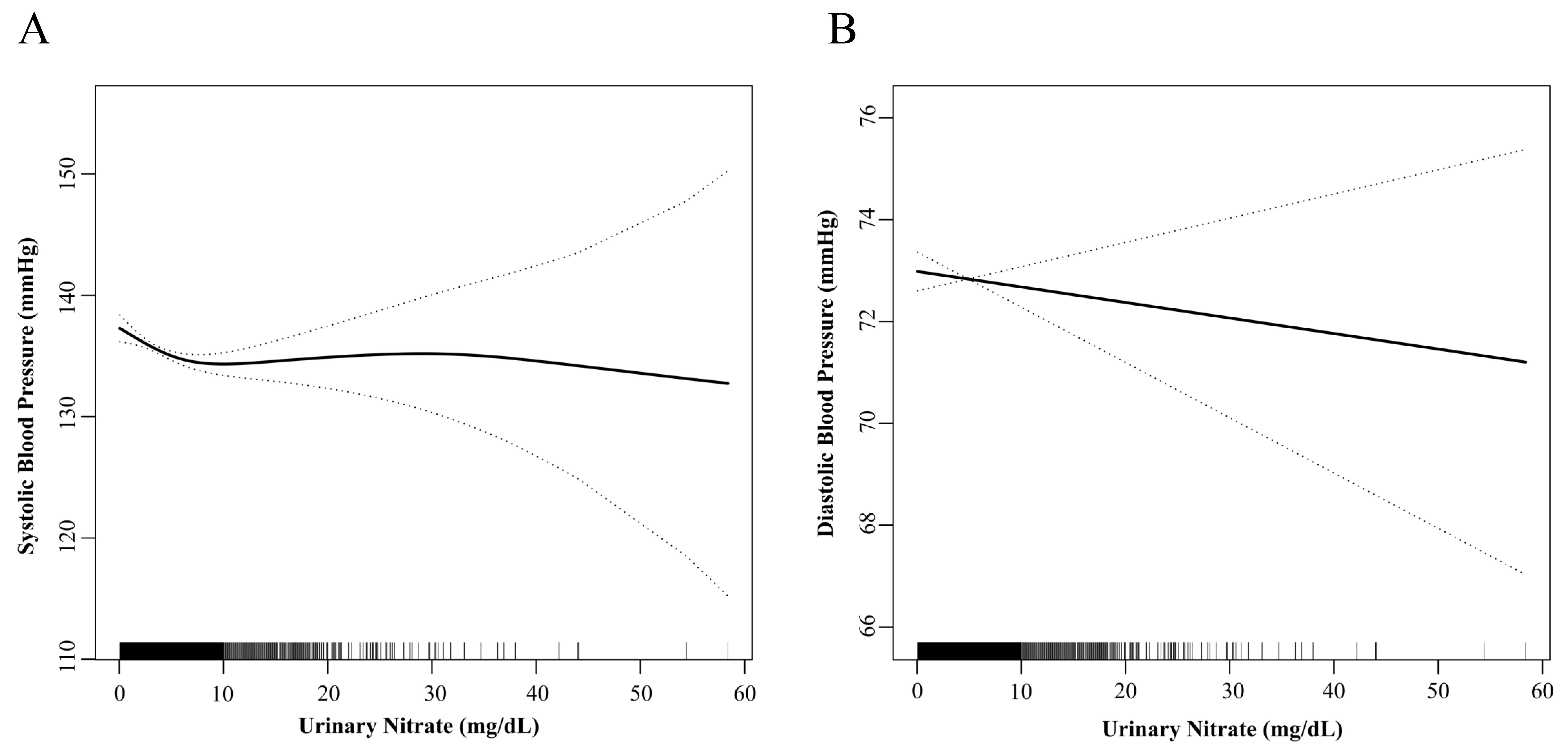
Figure 2. Relationship between urinary nitrate and blood pressure. (A) The relationship between urinary nitrate and systolic blood pressure; (B) the relationship between urinary nitrate and diastolic blood pressure.
Saturation effect between urinary nitrate and systolic blood pressure
| β (95%CI) | P-value | |
| Model 1: Fitting model by standard linear regression | -0.18 [(-0.28)-(-0.07)] | < 0.001 |
| Model 2: Fitting model by two-piecewise linear regression | ||
| Inflection point (mg/dL) | 4.40 (3.68-5.25) | |
| < 4.40 | -0.60 [(-0.99)-(-0.21)] | 0.003 |
| > 4.40 | -0.09 (-0.22-0.05) | 0.202 |
| P for log-likelihood ratio test | 0.029 | |
Association between urinary nitrate and diastolic blood pressure
| β (95%CI) | P-value | |
| Model 1: Fitting model by standard linear regression | -0.02 (-0.10-0.05) | 0.507 |
| Model 2: Fitting model by two-piecewise linear regression | ||
| Inflection point (mg/dL) | 1.33 (0.88-1.98) | |
| < 1.33 | 1.66 (-0.16-3.49) | 0.079 |
| > 1.33 | -0.04 (-0.12-0.03) | 0.266 |
| P for log-likelihood ratio test | 0.069 |
Urinary nitrate and the prevalence of cardiovascular diseases
As shown in Table 1, among the 6,130 participants, the prevalence of angina pectoris, MI, CHD, and HF was 4.3%, 6.7%, 6.7%, and 4.9%, respectively. Multivariable logistic regression analysis [Table 4] revealed that urinary nitrate levels were significantly and inversely associated with HF prevalence. The unadjusted, partially adjusted and fully adjusted odds ratios (ORs) with 95%CIs were 0.880 (95%CI, 0.846-0.916; P < 0.001), 0.902 (95%CI, 0.866-0.940; P < 0.001) and 0.942 (95%CI, 0.905-0.981; P = 0.004), respectively. A similar downward trend in the prevalence of angina pectoris was observed with increasing urinary nitrate, although it did not reach statistical significance (fully adjusted OR, 0.989; 95%CI, 0.939-1.041; P = 0.672). No significant associations were found between urinary nitrate and the prevalence of MI (OR, 1.017; 95%CI, 0.984-1.051; P = 0.315) or CHD (OR, 1.016; 95%CI, 0.982-1.051; P = 0.363).
Association of urinary nitrate with the prevalence of cardiovascular diseases
| Cases | OR (95%CI) | P-value | |
| Angina pectoris | 292 | ||
| Model 1 | 0.958 (0.910-1.007) | 0.096 | |
| Model 2 | 0.977 (0.930-1.027) | 0.362 | |
| Model 3 | 0.989 (0.939-1.041) | 0.672 | |
| Myocardial infarction | 469 | ||
| Model 1 | 0.981 (0.949-1.014) | 0.262 | |
| Model 2 | 1.002 (0.970-1.034) | 0.907 | |
| Model 3 | 1.017 (0.984-1.051) | 0.315 | |
| Coronary heart disease | 455 | ||
| Model 1 | 0.979 (0.943-1.017) | 0.282 | |
| Model 2 | 1.004 (0.970-1.040) | 0.812 | |
| Model 3 | 1.016 (0.982-1.051) | 0.363 | |
| Heart failure | 372 | ||
| Model 1 | 0.880 (0.846-0.916) | < 0.001 | |
| Model 2 | 0.902 (0.866-0.940) | < 0.001 | |
| Model 3 | 0.942 (0.905-0.981) | 0.004 |
Urinary nitrate and cardiovascular mortality
During a weighted median follow-up of 65.0 months (interquartile range: 37.0-97.0 months), 214 participants (weighted proportion: 2.0%) died from cardiovascular disease. The Kaplan-Meier curves [Figure 3] demonstrated that elevated urinary nitrate was significantly associated with superior cardiovascular-specific survival (Log-rank test, P < 0.001). Consistently, multivariable-adjusted Cox proportional hazards models showed that each unit increase in urinary nitrate was associated with a 7.9% reduction in cardiovascular mortality risk [hazard ratio (HR), 0.921; 95%CI, 0.867-0.977; P = 0.006; Table 5].
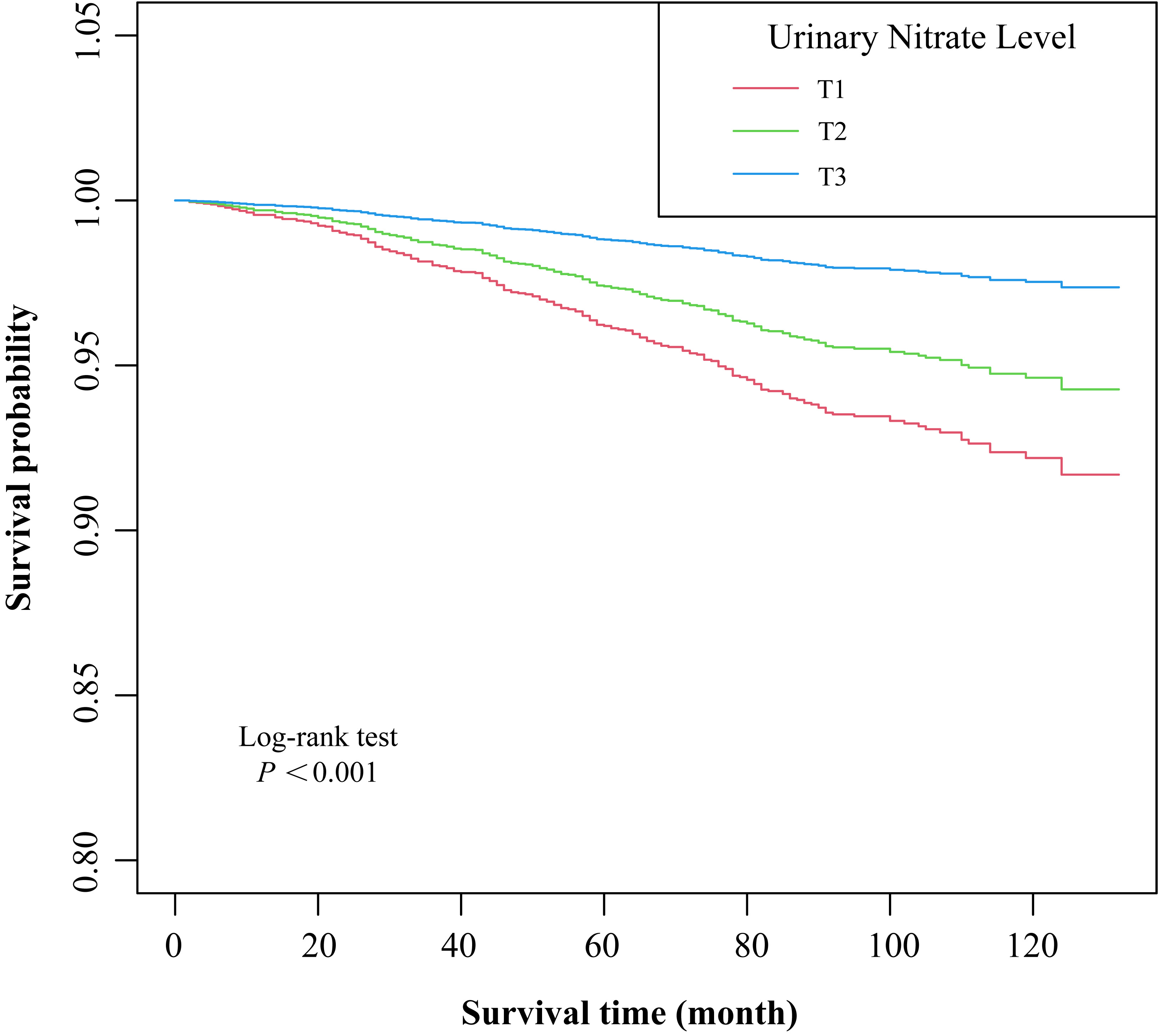
Figure 3. Survival curves for individuals with different urinary nitrate levels. T1, ≤ 2.82 mg/dL; T2, 2.82-5.52 mg/dL; T3, > 5.52 mg/dL.
Association of urinary nitrate with cardiovascular mortality
| Cases | HR (95%CI) | P-value | |
| Cardiovascular mortality | 214 | ||
| Model 1 | 0.854 (0.786 - 0.928) | < 0.001 | |
| Model 2 | 0.903 (0.837 - 0.974) | 0.008 | |
| Model 3 | 0.921 (0.867 - 0.977) | 0.006 |
Mediation analysis
Mediation analysis was performed to explore whether the association between urinary nitrate and cardiovascular mortality was mediated by HF or SBP. As shown in Table 6, the average causal mediation effect (ACME) for HF was 1.925 (95%CI, -14.947-20.318; P = 0.836), accounting for only 0.6% of the total effect. Similarly, the ACME for SBP was 2.582 (95%CI, -1.173-9.927; P = 0.244), with a mediated proportion of 1.1%. In contrast, the average direct effect (ADE) remained significant in both models (P < 0.05), suggesting that the favorable cardiovascular outcomes associated with higher urinary nitrate were independent of HF and SBP.
Mediation analysis of the association between urinary nitrate and cardiovascular mortality
| Variables and Effects | Estimate (95%CI) | P-value |
| Heart failure | ||
| ACME | 1.925 (-14.947-20.318) | 0.836 |
| ADE | 193.168 (33.108-454.799) | 0.014 |
| Total effect | 195.093 (33.142-456.891) | 0.016 |
| Prop. Mediated | 0.006 (-0.129-0.133) | 0.836 |
| Systolic blood pressure | ||
| ACME | 2.582 (-1.173-9.927) | 0.244 |
| ADE | 193.313 (34.164-488.182) | 0.020 |
| Total effect | 195.896 (38.595-492.504) | 0.020 |
| Prop. Mediated | 0.011 (-0.011-0.056) | 0.260 |
Subgroup analysis
Results of subgroup analyses for the association of urinary nitrate with cardiovascular mortality are shown in Figure 4. A significant interaction was observed for history of CHD [P-interaction < 0.001; false discovery rate (FDR)-adjusted P < 0.001]. The protective association was more pronounced in participants without CHD (HR, 0.849; 95%CI, 0.802-0.898), while no such association was observed in those with CHD (HR, 1.063; 95%CI, 0.991-1.140). Additionally, while a nominal interaction was noted for smoking status (P-interaction = 0.045), it did not retain statistical significance after FDR adjustment (P = 0.202). The inverse association remained largely consistent across most subgroups, including age, sex, BMI, history of diabetes or stroke, history of HF, and antihypertensive medication (all P-interaction > 0.05). It is important to note that some subgroups were characterized by small sample sizes and imbalanced distributions. These results should be interpreted with caution due to the potentially limited statistical power in these specific strata.
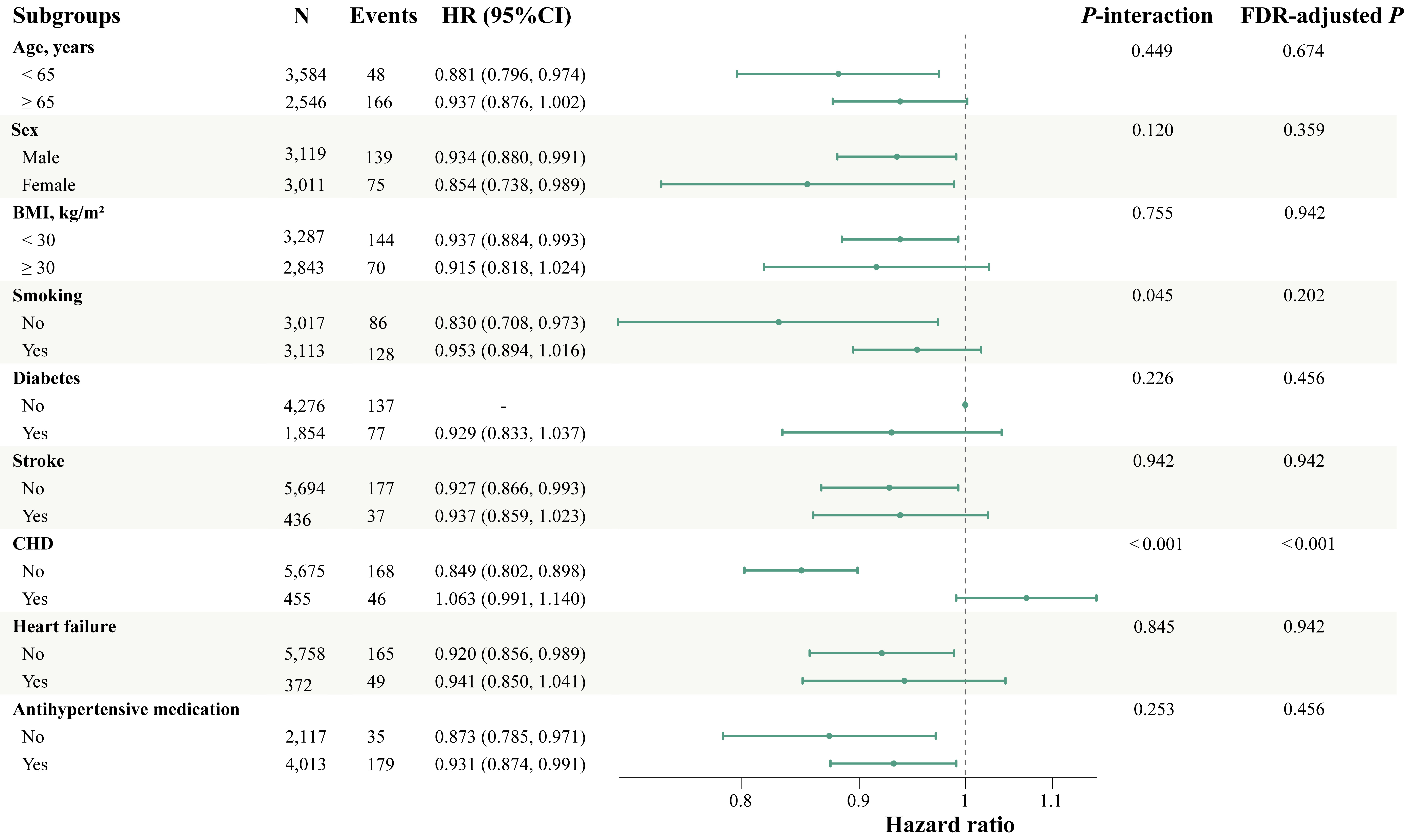
Figure 4. Subgroup analysis of the association between urinary nitrate and cardiovascular mortality. “-” indicates data not available. BMI: Body mass index; CHD: coronary heart disease; HR: hazard ratio; CI: confidence interval; FDR: false discovery rate.
DISCUSSION
This study investigated the association between urinary nitrate and blood pressure, along with its links to CVD prevalence and cardiovascular mortality. The findings revealed that higher urinary nitrate levels were inversely associated with baseline SBP in hypertensive participants, but this association reached a plateau above a certain nitrate concentration. Furthermore, higher urinary nitrate levels were associated with a reduced prevalence of HF and a lower risk of cardiovascular mortality. Notably, neither SBP nor HF significantly mediated this association, suggesting a potentially independent protective mechanism. Subgroup analyses confirmed the robustness of the inverse association between urinary nitrate and cardiovascular mortality across most subgroups. While these findings provide supportive evidence for the potential cardiovascular benefits of inorganic nitrates, it is essential to interpret them as observational associations. The reliance on a single-point measurement of urinary nitrate and the absence of time-varying exposure data further limit causal inference, necessitating caution when extrapolating these results to clinical practice.
In this study, we identified an inverse association between urinary nitrate and baseline SBP in hypertensive participants, characterized by a saturation effect at 4.40 mg/dL. This finding suggests that while moderate nitrate levels - likely reflecting dietary intake[18] - are linked to blood pressure reduction, the incremental benefit reaches a plateau at higher concentrations. This observation aligns with a previous meta-analysis of beetroot juice intervention, which consistently reports significant SBP reduction of 4.95 mmHg [95%CI, (-8.88)-(-1.01); P < 0.001] while DBP remains relatively stable[19]. Furthermore, evidence from another meta-analysis supports the capacity of inorganic nitrate to significantly lower both SBP and DBP[20].
The observed discrepancy, where urinary nitrate levels were inversely associated with SBP but not DBP, may stem from the distinct hemodynamic determinants of these parameters. SBP is particularly sensitive to large artery stiffness and pressure wave reflections, both of which are directly modulated by NO bioavailability[21,22]. As an exogenous NO donor, inorganic nitrate follows the nitrate-nitrite-NO pathway to activate soluble guanylate cyclase (sGC) and the downstream cyclic Guanosine Monophosphate (cGMP) signaling cascade[23]. This process enhances arterial compliance and promotes systemic vasodilation, thereby alleviating ventricular afterload. This hemodynamic shift is typically more pronounced in systolic than diastolic measurements[7,24]. These findings align with recent meta-analyses suggesting that inorganic nitrate supplementation yields reductions in SBP more consistently than in DBP, likely reflecting its predominant action on conduit artery function rather than peripheral resistance during the diastolic phase[25]. Furthermore, nitrate-derived NO bioactivity has been shown to inhibit renal nicotinamide adenine dinucleotide phosphate(NADPH) oxidase activity, thereby mitigating oxidative stress and relieving the increased renal vascular resistance caused by Angiotensin II[26,27].
The observed saturation effect may suggest a potential physiological ceiling to the antihypertensive ability of the nitrate-nitrite-NO, which is an intriguing finding that warrants careful interpretation. Although this observational study cannot establish causality, several hypothetical frameworks may be considered based on existing literature. One potential explanation involves the desensitization of the nitrate-nitrite-NO pathway. Specifically, experimental evidence suggests that chronic exposure to supra-physiological concentrations of NO might lead to a downregulation of both sGC protein expression and enzymatic activity, involving a shift from sGC to apo-sGC (NO-insensitive sGC)[23]. Furthermore, extremely high nitrate levels in this population may serve as a proxy for dietary patterns rich in processed or pickled meats. The high sodium content of such foods could independently elevate blood pressure, thereby antagonizing the vasodilatory benefits of inorganic nitrate. Notably, we observed that participants in the highest urinary nitrate quartile also exhibited the highest dietary sodium intake. While these mechanisms remain speculative, they provide a foundation for future experimental validation.
This study demonstrated that elevated urinary nitrate levels were associated with a lower prevalence of HF. Specifically, an increase of 1 mg/dL in urinary nitrate concentration was independently associated with a 5.8% reduction in the risk of HF. This finding is consistent with previous large-scale epidemiological evidence. For instance, the Danish Diet, Cancer, and Health Study reported that moderate increases in vegetable nitrate intake were associated with a 12%-26% lower risk of hospitalization for various cardiovascular conditions, including a 15% reduction in HF risk[7]. Similarly, another observational study showed that participants in the highest urinary nitrate quartile had a significantly lower prevalence of HF (OR, 0.375) compared with those in the lowest quartile[28]. However, no statistically significant associations were identified for MI, angina pectoris, or CHD. This discrepancy likely reflects the distinct pathological foundations of HF and ischemic heart diseases. The protective association observed for HF may be attributed to the inorganic nitrate-nitrite-NO pathway, which functions as an essential supplemental system for maintaining NO bioavailability, particularly when the endogenous L-arginine-nitric oxide synthase (NOS) pathway is impaired[23,29]. Mechanistically, nitrate-derived NO promotes hemodynamic improvement by reducing vascular stiffness and alleviating the afterload and wall stress in the left ventricle[30]. Additionally, nitrate may enhance myocardial compliance via the NO-sGC-cGMP signaling pathway - a critical factor in heart failure with preserved ejection fraction - and improve mitochondrial respiratory efficiency to provide “metabolic sparing” support in the energy-depleted failing heart[24,31]. However, physiological NO levels generated from inorganic nitrate may be insufficient to counteract fixed structural obstructions or advanced atherosclerotic plaques. The pro-oxidative environment in CHD, marked by high levels of reactive oxygen species (ROS), can rapidly scavenge NO to form toxic peroxynitrite, effectively nullifying its vascular benefits[32]. Consequently, the impact of inorganic nitrate on preventing acute ischemic events in patients with structural arterial narrowing appears to be limited.
The current study found that elevated urinary nitrate levels were associated with a significant reduction in cardiovascular mortality. Notably, neither SBP nor the prevalence of HF significantly mediated this protective association. Accordingly, we propose several alternative microvascular and cellular mechanisms. First, nitrate-derived NO acts as a pivotal regulator of endothelial function and microvascular health, functioning independently of systemic arterial pressure. Recent evidence suggests that enhancing the inorganic nitrate-nitrite-NO pathway can significantly restore endothelial NO bioavailability and improve microcirculatory perfusion, effectively mitigating the core pathophysiological processes of cardiovascular-kidney-metabolic (CKM) syndrome[33]. Furthermore, a systematic review demonstrated that habitual nitrate intake is inversely associated with overall cardiovascular mortality, with benefits attributable primarily to endothelial preservation rather than solely through systemic blood pressure reduction[8]. Second, nitrate enhances mitochondrial efficiency and suppresses oxidative stress. With advancing age and cardiometabolic stress, mitochondrial dysfunction leads to excessive generation of ROS, which scavenges endogenous NO. Inorganic nitrite supplementation has been shown to suppress mitochondrial oxidative stress and restore endothelial function without inducing significant hypotensive effects[34]. By preserving cellular energy homeostasis, nitrate metabolism may protect vital organs against ischemic injuries, thereby prolonging survival independent of systemic hemodynamics. Third, the pleiotropic effects of the nitrate-nitrite-NO pathway encompass potent anti-inflammatory and anti-thrombotic properties. NO governs blood flow and nutrient delivery at the cellular level while simultaneously mitigating immune dysfunction and low-grade inflammation[35,36]. These mechanisms collectively reduce the risk of subclinical microthrombi and systemic tissue damage, both of which are strong, independent predictors of all-cause mortality.
Subgroup analysis revealed a significant interaction between urinary nitrate levels and the history of CHD. While higher urinary nitrate was robustly associated with reduced cardiovascular mortality in participants without CHD, this protective association was absent in those with CHD. This divergence may be attributed to differences in endothelial functional status. In participants without CHD, intact enzymatic machinery allows nitrate-derived NO to maintain vascular tone and anti-inflammatory effects, providing a robust “primary prevention” benefit[7,23]. Conversely, in established CHD, severe endothelial dysfunction and enhanced oxidative stress promote the scavenging of NO by ROS to form toxic peroxynitrite, which may exacerbate vascular damage and counteract the physiological benefits of nitrate intake[37,38]. Furthermore, the irreversible structural remodeling and calcified plaques of advanced CHD may represent a “point of no return”, where functional modulation is insufficient to overcome fixed arterial narrowing[39,40]. Collectively, these findings underscore that inorganic nitrate acts as a potent modifier of vascular resilience primarily in early-stage prevention rather than as a secondary intervention for advanced ischemic disease.
In this study, urinary nitrate served as a practical and objective biomarker reflecting both exogenous dietary intake and endogenous nitric oxide metabolism[41-44]. Unlike dietary questionnaires, which are subject to recall bias, urinary nitrate provides a more direct assessment of total nitrate exposure in a large-scale population. Our findings demonstrate that this marker is independently associated with cardiovascular outcomes, suggesting its potential utility in risk stratification within the general hypertensive population. However, given the observational nature of NHANES, these results should be interpreted as indicative of a biological link rather than as evidence of a definitive causal effect.
Limitations
This study has several limitations that warrant consideration. First, the cross-sectional design of the NHANES database precludes the establishment of definitive causal relationships between urinary nitrate levels, blood pressure, and cardiovascular outcomes. While robust associations were observed, the lack of temporal sequencing between exposure and outcome leaves the possibility of reverse causality unresolved. Therefore, these findings should be further validated through large-scale prospective cohort studies.
Second, the reliance on a single spot urine sample to assess nitrate exposure represents an inherent limitation. Urinary nitrate concentrations are sensitive to recent dietary intake and exhibit significant diurnal fluctuations. Thus, a single measurement may not accurately reflect chronic exposure, potentially leading to non-differential misclassification of the exposure status. From a statistical perspective, such random measurement error typically attenuates effect estimates (bias toward the null). Therefore, the inverse associations between urinary nitrate and cardiovascular mortality observed in this study may be underestimated. Future research employing repeated measurements or 24 h urine collections would provide a more robust assessment.
Third, the ascertainment of CVD history relied primarily on self-reported questionnaires rather than independent clinical adjudication or comprehensive medical record reviews. This may introduce recall bias or social desirability bias, which could affect the accuracy of our prevalence estimates.
Fourth, although our mediation analysis suggested that urinary nitrate may influence cardiovascular mortality through pathways independent of blood pressure and heart failure, the underlying biological mechanisms require further elucidation. The “direct effect” observed in our models may be partially attributed to unmeasured physiological pathways or complex interactions between nitrates and other metabolic factors.
Fifth, several population-specific limitations must be acknowledged. The study utilized NHANES data, which is representative of the U.S. civilian population but may lack generalizability to other ethnic groups or global regions with distinct environmental and lifestyle exposure profiles.
Finally, the possibility of residual confounding cannot be entirely excluded. Our analysis lacked detailed information on the duration of hypertension. Although we adjusted for current blood pressure levels and antihypertensive medication use as proxies for severity, the absence of long-term blood pressure control data may lead to residual confounding. The duration of disease could independently influence cardiovascular prognosis, and it should be explored in future longitudinal studies with clinical cohorts. Additionally, physical activity was not included due to inconsistent survey methodologies across the 2005-2006 cycle and subsequent cycles. NHANES also lacks data on medication adherence, which may affect the management of hypertension and subsequent cardiovascular risk.
CONCLUSIONS
In this study, urinary nitrates within a certain range exhibit an inverse association with SBP in the hypertensive participants. Furthermore, elevated urinary nitrate levels are independently associated with a lower prevalence of heart failure and reduced cardiovascular mortality. However, the cardioprotective association appears most robust in primary prevention but is not evident in individuals with established CHD. Inorganic nitrates may be linked to lower cardiovascular mortality through mechanisms beyond lowering SBP and reducing the risk of heart failure. While these results suggest that inorganic nitrate could serve as a promising marker and intervention target for improving cardiovascular outcomes, the observational nature of the study and the reliance on single-point measurements necessitate caution. Future prospective longitudinal studies and randomized controlled trials are warranted to validate these associations and elucidate the underlying molecular pathways.
DECLARATIONS
Acknowledgments
The Graphical Abstract was created with BioRender (https://BioRender.com/f56qxjf). We thank all contributors and participants in NHANES.
Authors’ contributions
Made substantial contributions to conception and design of the study and performed data analysis and interpretation: Zhao W, Li D, Chen Y, Yin Y, Ling Z
Performed data acquisition and provided technical and material support: Zhang B, Wang Z, Xiong Q, Zhou H
Availability of data and materials
The datasets analyzed during the current study are available in the NHANES repository, https://www.cdc.gov/nchs/nhanes/index.html, and are available from the corresponding author upon reasonable request.
AI and AI-assisted tools statement
During the preparation of this manuscript, the AI tool Gemini (version 3.0, released 2025-12-17) was used solely for language editing. The tool did not influence the study design, data collection, analysis, interpretation, or the scientific content of the work. All authors take full responsibility for the accuracy, integrity, and final content of the manuscript.
Financial support and sponsorship
None.
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
The NHANES protocols were approved by the National Center for Health Statistics (NCHS) Ethics Review Board (ERB) (Protocol #2005-06 and #2011-17). All participants provided written informed consent. As this study was a secondary analysis of anonymous public-access data, it was exempt from further institutional review board (IRB) approval by the Second Affiliated Hospital of Chongqing Medical University.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Naghavi M, Ong KL, Aali A, et al. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403:2100-32.
2. Nambiar L, Lewinter MM, Vanburen PC, Dauerman HL. Decade-long temporal trends in U.S. Hypertension-related cardiovascular mortality. J Am Coll Cardiol. 2020;75:2644-6.
3. Fuchs FD, Whelton PK. High blood pressure and cardiovascular disease. Hypertension. 2020;75:285-92.
4. Carlström M, Weitzberg E, Lundberg JO. Nitric oxide signaling and regulation in the cardiovascular system: recent advances. Pharmacol Rev. 2024;76:1038-62.
5. Lundberg JO, Carlström M, Weitzberg E. Metabolic effects of dietary nitrate in health and disease. Cell Metab. 2018;28:9-22.
6. Li D, Nishi S, Jovanovski E, et al. Repeated administration of inorganic nitrate on blood pressure and arterial stiffness: a systematic review and meta-analysis of randomized controlled trials. J Hypertens. 2020;38:2122-40.
7. Bondonno CP, Dalgaard F, Blekkenhorst LC, et al. Vegetable nitrate intake, blood pressure and incident cardiovascular disease: danish diet, cancer, and health study. Eur J Epidemiol. 2021;36:813-25.
8. Tan L, Stagg L, Hanlon E, et al. Associations between vegetable nitrate intake and cardiovascular disease risk and mortality: a systematic review. Nutrients. 2024;16:1511.
9. Bondonno CP, Blekkenhorst LC, Prince RL, et al. Association of vegetable nitrate intake with carotid atherosclerosis and ischemic cerebrovascular disease in older women. Stroke. 2017;48:1724-9.
10. Jiang W, Zhang J, Yang R, et al. Association of urinary nitrate with diabetes complication and disease-specific mortality among adults with hyperglycemia. J Clin Endocrinol Metab. 2023;108:1318-29.
11. Casey DP, Bock JM. Inorganic nitrate supplementation attenuates conduit artery retrograde and oscillatory shear in older adults. Am J Physiol Heart Circ Physiol. 2021;320:H991-8.
12. Bondonno NP, Pokharel P, Bondonno CP, et al. Source-specific nitrate intake and all-cause mortality in the Danish diet, cancer, and health study. Eur J Epidemiol. 2024;39:925-42.
13. Mendy A. Association of urinary nitrate with lower prevalence of hypertension and stroke and with reduced risk of cardiovascular mortality. Circulation. 2018;137:2295-7.
14. Zhao W, Chen Y, Wang K, et al. Association of urinary nitrate with blood pressure, prevalence of cardiovascular diseases and cardiovascular mortality in hypertensive population. Research Square 2024.
15. National Center for Health Statistics. About the national health and nutrition examination survey. Available from: https://www.cdc.gov/nchs/nhanes/index.html [Last accessed on 25 May 2026].
16. The Centers for Disease Control and Prevention. Laboratory procedure manual. Available from: https://wwwn.cdc.gov/nchs/data/nhanes/public/2019/manuals/2020-MEC-Laboratory-Procedures-Manual-508.pdf [Last accessed on 25 May 2026].
17. National Center for Health Statistics. Office of analysis and epidemiology, public-use linked mortality file. Available from: https://www.cdc.gov/nchs/linked-data/mortality-files/index.html [Last accessed on 25 May 2026].
18. Capper TE, Siervo M, Clifford T, et al. Pharmacokinetic profile of incremental oral doses of dietary nitrate in young and older adults: a crossover randomized clinical trial. J Nutr. 2022;152:130-9.
19. Benjamim CJR, Porto AA, Valenti VE, et al. Nitrate derived from beetroot juice lowers blood pressure in patients with arterial hypertension: a systematic review and meta-analysis. Front Nutr. 2022;9:823039.
20. He Y, Liu J, Cai H, et al. Effect of inorganic nitrate supplementation on blood pressure in older adults: a systematic review and meta-analysis. Nitric Oxide. 2021;113-114:13-22.
21. Laurent S, Boutouyrie P. Arterial stiffness and hypertension in the elderly. Front Cardiovasc Med. 2020;7:544302.
22. Jones AM, Vanhatalo A, Seals DR, Rossman MJ, Piknova B, Jonvik KL. Dietary nitrate and nitric oxide metabolism: mouth, circulation, skeletal muscle, and exercise performance. Med Sci Sports Exerc. 2021;53:280-94.
24. Zamani P, Rawat D, Shiva-kumar P, et al. Effect of inorganic nitrate on exercise capacity in heart failure with preserved ejection fraction. Circulation. 2015;131:371-80.
25. Siervo M, Lara J, Ogbonmwan I, Mathers JC. Inorganic nitrate and beetroot juice supplementation reduces blood pressure in adults: a systematic review and meta-analysis. J Nutr. 2013;143:818-26.
26. Carlstrom M, Montenegro MF. Therapeutic value of stimulating the nitrate‐nitrite‐nitric oxide pathway to attenuate oxidative stress and restore nitric oxide bioavailability in cardiorenal disease. J Intern Med. 2018;285:2-18.
27. Gao X, Yang T, Liu M, et al. NADPH oxidase in the renal microvasculature is a primary target for blood pressure-lowering effects by inorganic nitrate and nitrite. Hypertension. 2015;65:161-70.
28. Wu Z, Tian T, Ma W, Gao W, Song N. Higher urinary nitrate was associated with lower prevalence of congestive heart failure: results from NHANES. BMC Cardiovasc Disord. 2020;20:498.
29. Gilchrist M, Shore AC, Benjamin N. Inorganic nitrate and nitrite and control of blood pressure. Cardiovasc Res. 2011;89:492-8.
30. Shimari M, Picozzi G, Boeder A, et al. Dietary nitrate prevents cardiac dysfunction in HFrEF by improving hemodynamics, ameliorating remodeling, and resolving inflammation. Acta Physiol. 2025;241:e70115.
31. Larsen FJ, Schiffer TA, Borniquel S, et al. Dietary inorganic nitrate improves mitochondrial efficiency in humans. Cell Metab. 2011;13:149-59.
32. Radi R. Oxygen radicals, nitric oxide, and peroxynitrite: redox pathways in molecular medicine. Proc. Natl. Acad. Sci. U.S.A. 2018;115:5839-48.
33. Liao GZ, He CH, Zhang YH, Zhang J. Addressing the “nitric oxide crisis” in cardiovascular-kidney-metabolic syndrome: therapeutic potential of the inorganic nitrate-nitrite-NO pathway. Obes Rev. 2025;27:e70021.
34. Rossman MJ, Gioscia-ryan RA, Santos-parker JR, et al. Inorganic nitrite supplementation improves endothelial function with aging: translational evidence for suppression of mitochondria-derived oxidative stress. Hypertension. 2021;77:1212-22.
35. Bryan NS, Ahmed S, Lefer DJ, Hord N, Von Schwarz ER. Dietary nitrate biochemistry and physiology. An update on clinical benefits and mechanisms of action. Nitric Oxide. 2023;132:1-7.
37. Fejes R, Pilat N, Lutnik M, et al. Effects of increased nitrate intake from beetroot juice on blood markers of oxidative stress and inflammation in older adults with hypertension. Free Radic Biol Med. 2024;222:519-30.
38. Sies H, Jones DP. Reactive oxygen species (ROS) as pleiotropic physiological signalling agents. Nat Rev Mol Cell Biol. 2020;21:363-83.
39. Lanzer P, Schurgers L, Twarda-clapa A, et al. Medial arterial calcification in ageing and disease: current evidence and knowledge gaps. Eur Heart J. 2025;46:4876-900.
40. Durham AL, Speer MY, Scatena M, Giachelli CM, Shanahan CM. Role of smooth muscle cells in vascular calcification: implications in atherosclerosis and arterial stiffness. Cardiovasc Res. 2018;114:590-600.
41. Carlström M. Nitric oxide signalling in kidney regulation and cardiometabolic health. Nat Rev Nephrol. 2021;17:575-90.
42. Berends JE, Van Den Berg LM, Guggeis MA, et al. Consumption of nitrate-rich beetroot juice with or without vitamin C supplementation increases the excretion of urinary nitrate, nitrite, and N-nitroso compounds in humans. Int J Mol Sci. 2019;20:2277.
43. Sundqvist ML, Lundberg JO, Weitzberg E, Carlström M. Renal handling of nitrate in women and men with elevated blood pressure. Acta Physiol. 2021;232:e13637.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].