
fig1
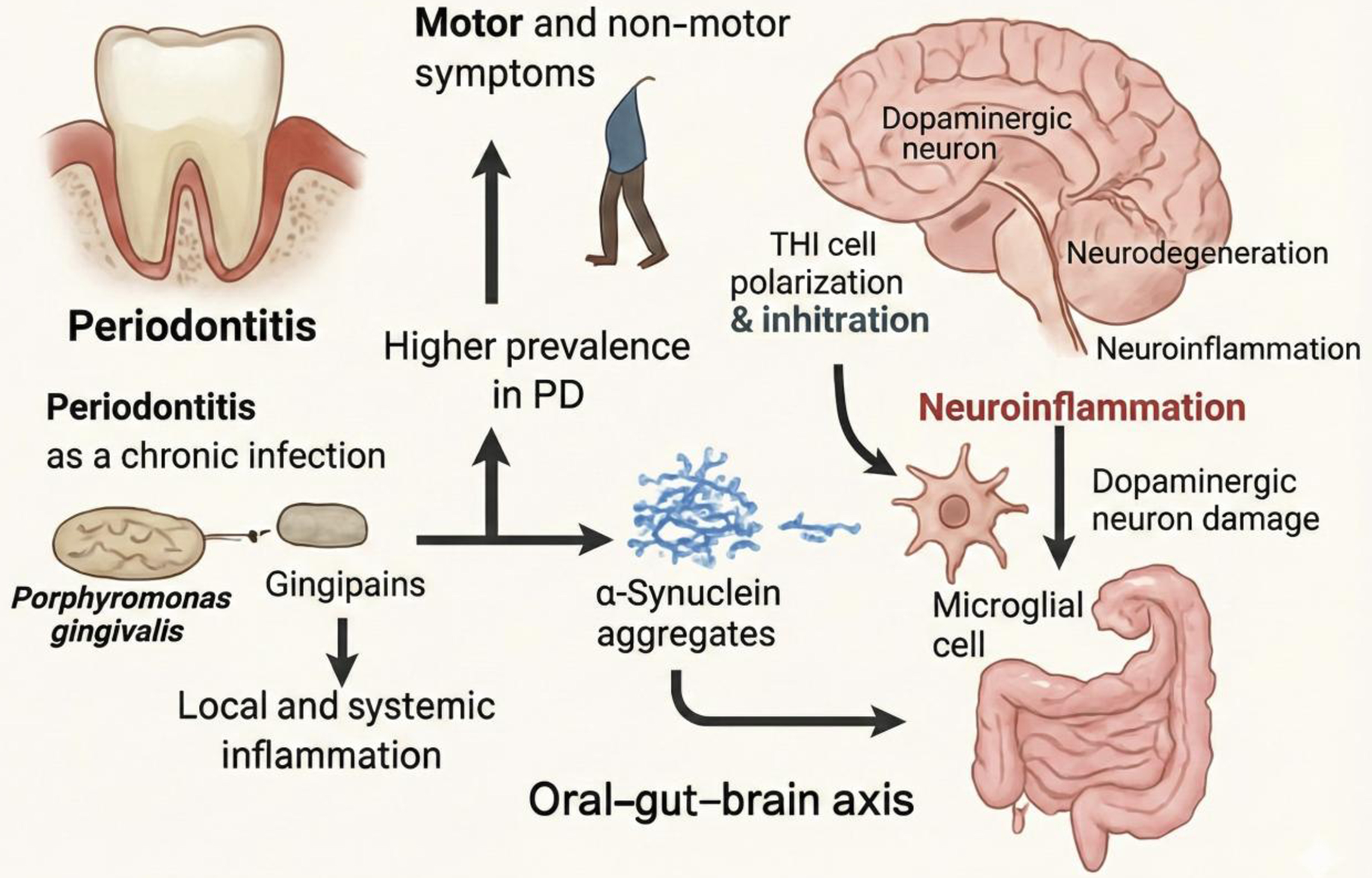
Figure 1. Bidirectional links between periodontitis and PD. PD-related motor and non-motor symptoms may impair daily oral self-care, thereby increasing the prevalence and severity of periodontitis. In the figure, the incomplete human silhouette represents gait impairment and reduced motor function in PD, including bradykinesia, postural instability, and mobility limitation, which can indirectly compromise oral hygiene practices. Periodontitis may, in turn, contribute to PD progression through chronic infection, local and systemic inflammation, microbial dysbiosis, and the oral-gut-brain axis. Key periodontal pathogens, particularly Porphyromonas gingivalis, and its Rgp/Kgp may promote pathological α-synuclein processing and aggregation. Peripheral immune skewing, such as Th1 polarization and infiltration, together with inflammatory mediators, can amplify microglial activation and neuroinflammation, ultimately contributing to dopaminergic neuronal damage. PD: Parkinson’s disease; Th1: T helper type 1; Rgp/Kgp: gingipains.





