
Progress on the interaction between periodontitis and Parkinson’s disease pathogenesis
 0
0 Abstract
There is a complex and potentially bidirectional association between Parkinson’s disease (PD) and periodontitis. Epidemiological studies consistently show that periodontal disease and other oral-health problems are more common in patients with PD, whereas the hypothesis that periodontitis increases PD susceptibility remains biologically plausible but not yet conclusively established. Mechanistically, PD-related motor and non-motor symptoms can impair oral self-care and worsen periodontal status; conversely, chronic periodontal infection may contribute to neurodegenerative stress through oral dysbiosis, the oral-gut-brain axis, microglial activation, Th1-skewed immune responses, oxidative stress, ferroptosis-related injury, and pathogen-associated effects on α-synuclein biology. Importantly, part of the observed association may also reflect shared modifiers, particularly vitamin D status and diet, which may influence both periodontal inflammation and PD-related vulnerability. Further clarification of these pathways may support more integrated oral-health management within comprehensive PD care.
Keywords
INTRODUCTION
Parkinson’s disease (PD) is the second most common neurodegenerative disorder worldwide and predominantly affects older adults[1-3]. It is characterized by the progressive degeneration of dopaminergic neurons in the substantia nigra pars compacta, leading to striatal dopamine deficiency and the cardinal motor manifestations of resting tremor, rigidity, bradykinesia, and postural instability[1-3]. In addition to motor symptoms, PD is frequently accompanied by non-motor manifestations, including cognitive impairment, mood disorders, sleep disturbance, autonomic dysfunction, and sleep-related symptoms, all of which substantially increase disease burden and complicate long-term management[1-3].
Oral disorders are highly prevalent in PD. Reduced manual dexterity, bradykinesia, dysphagia, drooling, xerostomia, altered dietary habits, and cognitive decline may collectively impair routine oral hygiene and dental attendance, thereby predisposing patients with PD to plaque accumulation, gingival inflammation, caries, and periodontal breakdown[4-8]. Periodontitis is a chronic inflammatory disease of the tooth-supporting tissues, including the gingiva, periodontal ligament, cementum, and alveolar bone. It is initiated by a dysbiotic biofilm and sustained by an aberrant host immune-inflammatory response. Major periodontal pathogens include Porphyromonas gingivalis, Fusobacterium nucleatum, and Tannerella forsythia[8-10]. Beyond causing tooth mobility and tooth loss, periodontitis has been associated with several systemic conditions, including diabetes, cardiovascular disease, rheumatoid arthritis, and neurodegenerative disorders, although the strength and causality of these associations vary across diseases and study designs[9,11].
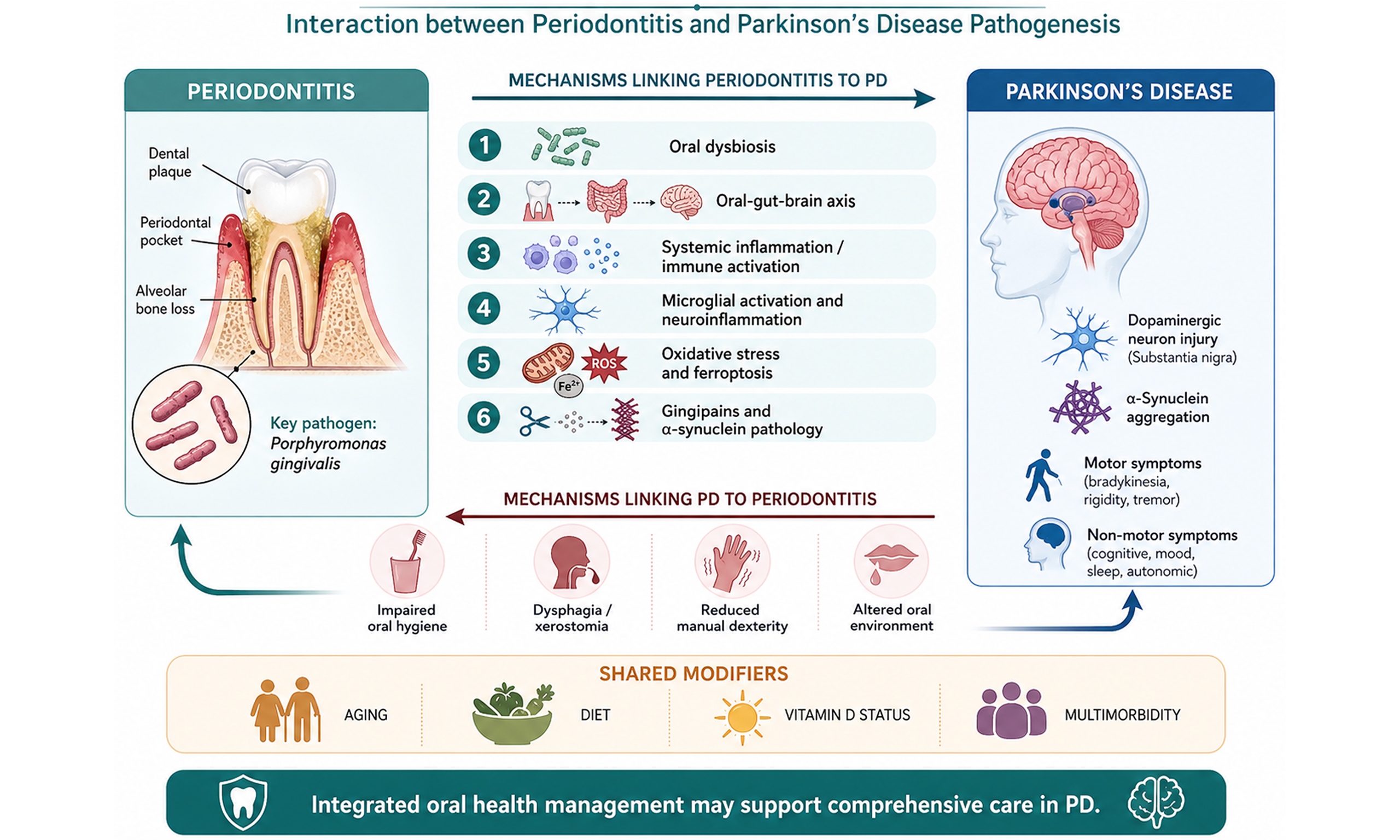
Emerging evidence suggests that the relationship between PD and periodontitis may be bidirectional but biologically asymmetric. On the one hand, PD plausibly worsens periodontal status mainly through impaired oral self-care, salivary dysfunction, altered mastication and swallowing, and reduced access to dental care[4-8]. On the other hand, periodontitis may contribute to PD-related pathology through oral dysbiosis, chronic low-grade systemic inflammation, blood-brain barrier dysfunction, immune activation, oxidative stress, ferroptosis-related injury, and possibly modulation of α-synuclein (α-syn) biology[10-31]. Importantly, however, the epidemiological evidence for periodontitis as a direct causal driver of PD remains mixed, and part of the observed association may reflect shared modifiers such as aging, frailty, multimorbidity, diet quality, and low serum 25-hydroxyvitamin D [25(OH)D] concentrations[11-16,32-38]. A schematic overview of the proposed bidirectional interaction between periodontitis and PD is shown in Figure 1.
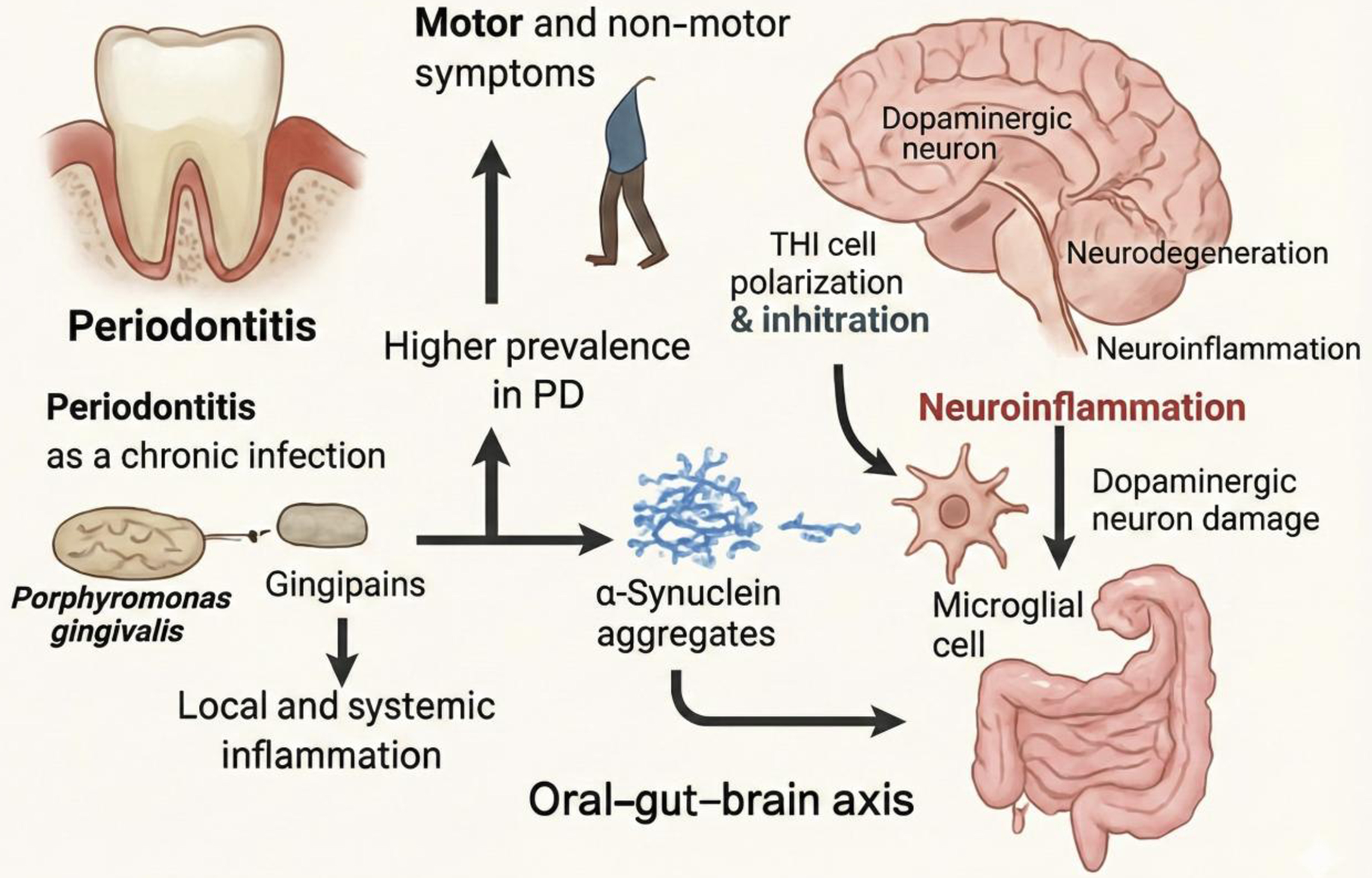
Figure 1. Bidirectional links between periodontitis and PD. PD-related motor and non-motor symptoms may impair daily oral self-care, thereby increasing the prevalence and severity of periodontitis. In the figure, the incomplete human silhouette represents gait impairment and reduced motor function in PD, including bradykinesia, postural instability, and mobility limitation, which can indirectly compromise oral hygiene practices. Periodontitis may, in turn, contribute to PD progression through chronic infection, local and systemic inflammation, microbial dysbiosis, and the oral-gut-brain axis. Key periodontal pathogens, particularly Porphyromonas gingivalis, and its Rgp/Kgp may promote pathological α-synuclein processing and aggregation. Peripheral immune skewing, such as Th1 polarization and infiltration, together with inflammatory mediators, can amplify microglial activation and neuroinflammation, ultimately contributing to dopaminergic neuronal damage. PD: Parkinson’s disease; Th1: T helper type 1; Rgp/Kgp: gingipains.
In this review, we synthesize current evidence on the epidemiological association and mechanistic interplay between periodontitis and PD, with particular emphasis on oral and gut microbiota, key periodontal pathogens, immune dysregulation, oxidative stress, ferroptosis, and shared modifiers such as diet and vitamin D. A separate graphic abstract is provided for submission.
EPIDEMIOLOGICAL ASSOCIATION BETWEEN PERIODONTITIS AND PD
Observational studies consistently indicate that oral health is poorer in patients with PD than in neurologically healthy controls. Systematic reviews and clinical studies have documented higher rates of periodontitis, xerostomia, drooling, tooth mobility, impaired chewing, and worse oral-health-related quality of life in PD populations[4-8,39,40]. As shown in Figure 2, the number of publications on the association between periodontitis and PD has risen markedly over the past decade, particularly after 2020, indicating increasing interest in this field.
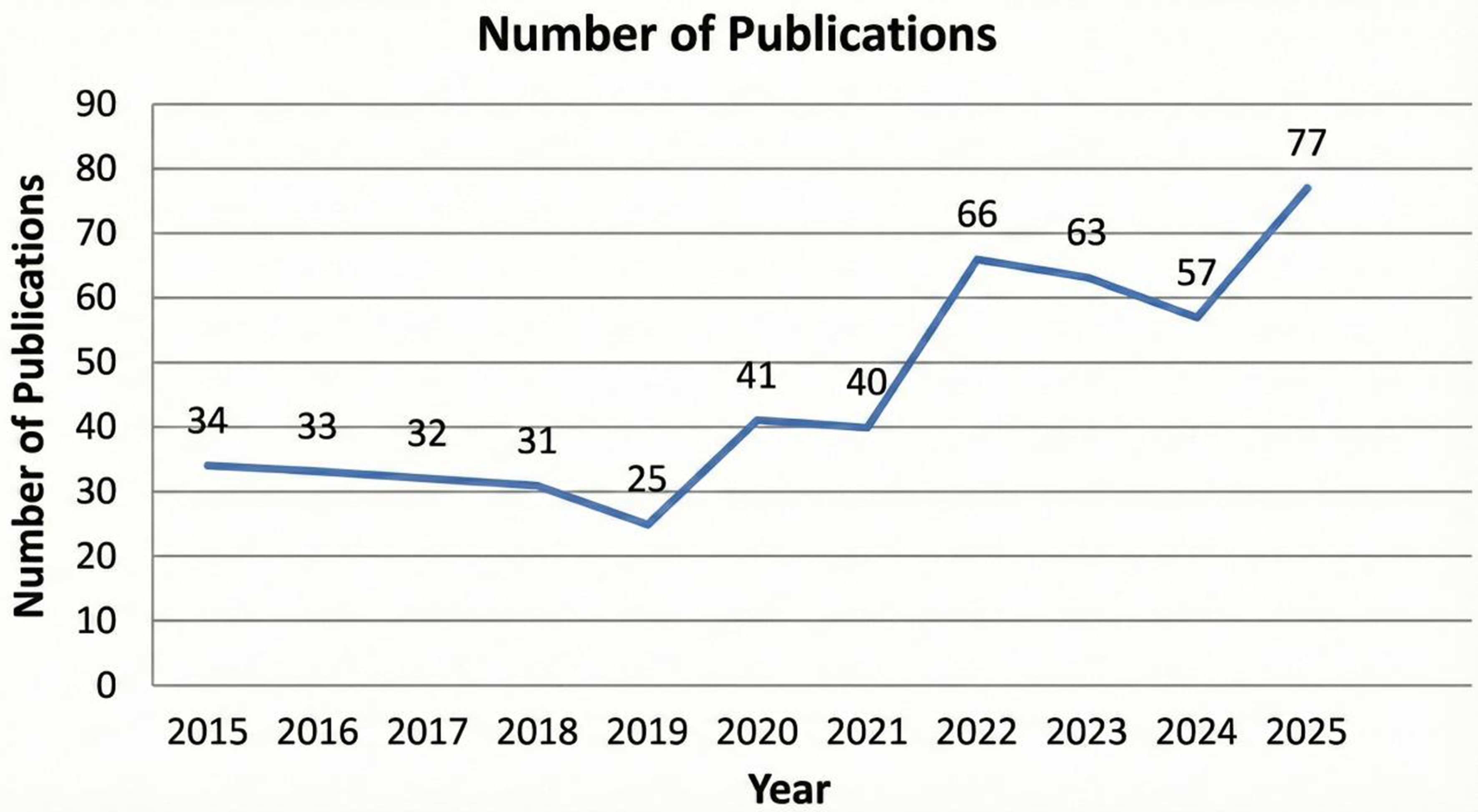
Figure 2. Annual publication trends in research on the association between periodontitis and PD (2015-2025). The x-axis represents publication year, and the y-axis represents the number of publications identified for each year. The overall upward trend indicates increasing academic interest in the relationship between periodontitis and PD, especially in relation to the oral-brain axis, neuroinflammation, and periodontal pathogen-driven neurodegeneration. A marked rise in publication output was observed after 2020, with a peak in 2025. Publications were identified through database searches of PubMed, Web of Science, CNKI, Wanfang, and VIP using combinations of the keywords “PD”, “oral health”, “dental caries”, and “periodontitis” for the period from 2015 to 2025. Inclusion criteria were articles published within the predefined time window; studies focusing on PD and periodontitis/oral health; and epidemiological, clinical, experimental, mechanistic, and review articles relevant to the interaction between periodontitis and PD. Exclusion criteria were duplicate records; studies unrelated to PD or periodontitis; conference abstracts without sufficient bibliographic information; editorials, news items, or letters lacking substantive scientific content; and articles with inaccessible or inadequate full-text information for evaluation. PD: Parkinson’s disease; CNKI: China National Knowledge Infrastructure; VIP: Chinese Science and Technology Journal Database.
Whether periodontitis itself increases the likelihood of later PD is less certain. Population-based studies from East Asia have reported statistically significant associations between chronic periodontitis and subsequent PD or parkinsonism[13-15]. Chen et al. reported that periodontal inflammatory disease was associated with a higher subsequent risk of PD in a matched cohort study[13]. Jeong et al. also observed an association in a nationwide retrospective cohort, although the effect estimates were modest and sensitive to confounder adjustment[14]. More recently, Lee et al. found that chronic periodontitis was associated with PD in a Korean national cohort, again with a relatively small effect size[15]. A bidirectional Mendelian randomization study further suggested a possible causal relationship, but the inference was limited by instrument strength and ancestry constraints[16].
However, the current evidence does not support an unequivocal causal claim. The most comprehensive meta-analysis available concluded that there was no clear bidirectional association between PD risk and periodontitis risk, although PD patients showed a higher prevalence of periodontitis and overall poorer oral status[12]. Therefore, the more robust conclusion at present is that PD is reliably associated with worse periodontal health, whereas the hypothesis that periodontitis increases PD susceptibility remains plausible but unproven[11-16].
An important unresolved issue is confounding by shared background determinants. Aging, chronic inflammation, dietary quality, frailty, metabolic disease, and low vitamin D status may predispose to both PD and periodontitis[9,32-38]. Thus, the epidemiological overlap between the two disorders may reflect both true biological interaction and partially shared upstream risk architecture.
MECHANISTIC LINKS BETWEEN PERIODONTITIS AND PD PATHOGENESIS
Oral dysbiosis, periodontal ecology, and the oral-gut-brain axis
Several studies suggest that PD may reshape the oral microbial environment, particularly in the setting of periodontitis. Yay et al. showed that PD was associated with altered subgingival microbiome composition in patients with periodontitis, supporting the view that PD-related host factors may modify periodontal dysbiosis rather than simply increase plaque accumulation[17]. This is biologically plausible: bradykinesia and rigidity impair brushing and interdental cleaning, dysphagia changes oral clearance, and xerostomia reduces salivary buffering[4-8,17].
In a subsequent oral-gut profiling study, Yay et al. found that salivary microbial β-diversity differed across healthy controls, periodontitis, and PD with periodontitis, whereas gut microbiome differences were less pronounced after accounting for the periodontal background[18]. These findings suggest that PD may exert a clearer and more reproducible influence on oral ecological structure than on the gut microbiome within mixed periodontal cohorts[17,18]. More recent work also points to potentially informative oral microbiome signatures in early PD and reinforces the idea that oral dysbiosis may have biomarker potential, although these observations still require external validation and standardization of sampling methods[18].
The oral-gut-brain axis provides a broader mechanistic framework for interpreting these findings. Chronic periodontal infection can repeatedly expose the host to lipopolysaccharide (LPS), proteases, inflammatory cytokines, and bacterial extracellular vesicles, thereby altering intestinal permeability, immune tone, and possibly vagal or systemic routes of signaling to the brain[10,19]. In mice, Bai et al. showed that oral pathogens aggravated motor dysfunction, enhanced dopaminergic neurodegeneration, and promoted both oral/gut microbial changes and immune-cell infiltration in an 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP) model of PD[19]. Feng et al. further demonstrated that oral P. gingivalis impaired gut permeability and triggered immune responses associated with neurodegeneration in LRRK2 R1441G mice, lending additional support to an oral-gut-immune route relevant to PD-like pathology[22].
Taken together, these data suggest that oral dysbiosis in PD is not merely a secondary epiphenomenon of poor hygiene. Rather, a reciprocal model is more appropriate: PD can modify the oral habitat, while chronic periodontal infection may feed back into systemic inflammatory and microbial pathways relevant to neurodegeneration.
Porphyromonas gingivalis and its virulence factors
Among periodontal pathogens, P. gingivalis has attracted particular attention because of its ability to drive persistent mucosal inflammation and systemic immune activation[10,20-22]. Its virulence repertoire includes LPS, gingipains, fimbriae, and outer membrane vesicles, all of which can disrupt host tissues and potentially contribute to extra-oral disease pathways[10].
Although much of the early interest in P. gingivalis centered on Alzheimer’s disease, increasing attention has been directed toward PD. Reviews have proposed that P. gingivalis may influence PD through hematogenous spread of virulence factors, peripheral immune priming, blood-brain barrier vulnerability, and promotion of neuroinflammation[10,20,21]. Ermini et al. provided especially notable neuropathological evidence by demonstrating ultrastructural localization of gingipains in dopaminergic neurons of the substantia nigra in PD brains and showing occasional spatial association with phosphorylated Ser129 α-syn aggregates[20]. They also showed that recombinant α-syn could be proteolytically cleaved by gingipains in vitro, supporting a plausible biochemical interface between chronic periodontal infection and α-syn processing[20].
A separate review specifically focused on P. gingivalis in PD with cognitive impairment and summarized evidence that this pathogen may contribute to cognitive and motor decline through neuroinflammation, altered proteostasis, and gut-brain signaling[21]. In parallel, the animal study by Feng et al. linked oral P. gingivalis exposure to gut permeability changes and neuroimmune activation in a PD-related genetic model[22]. These findings do not prove that P. gingivalis causes PD, but they make it one of the most biologically plausible periodontal candidates linking oral infection to PD-related neurodegenerative stress. The principal molecular pathways implicated in periodontal pathogen-driven neurodegeneration are summarized in Figure 3.
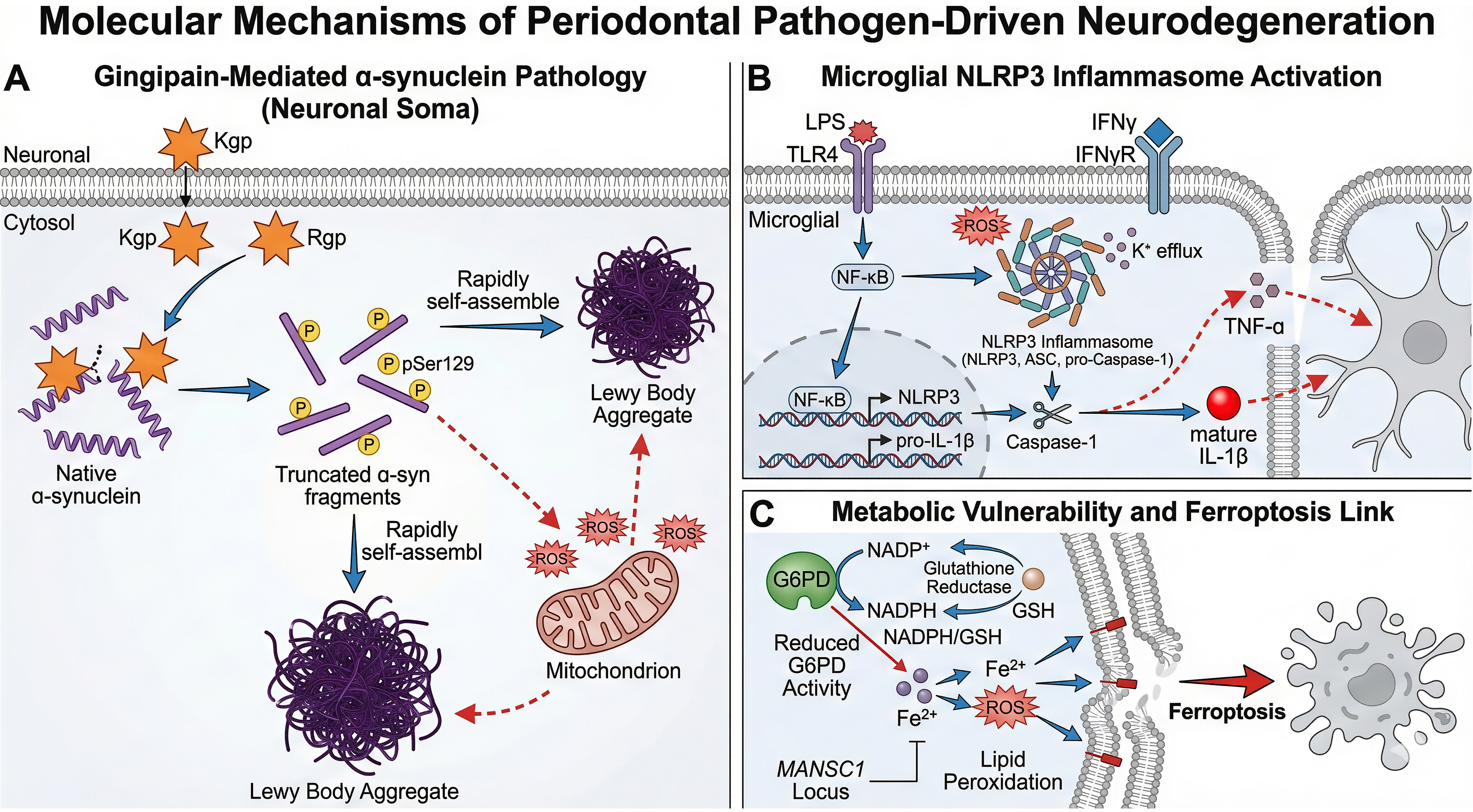
Figure 3. Molecular mechanisms of periodontal pathogen-driven neurodegeneration relevant to PD. (A) Gingipain-mediated α-syn pathology in neuronal soma. Virulence factors from Porphyromonas gingivalis, particularly Kgp and Rgp, may cleave native α-syn into truncated fragments that undergo phosphorylation, such as pSer129, and rapidly self-assemble into Lewy body-like aggregates. Concurrent mitochondrial dysfunction and ROS generation may further amplify protein aggregation and neuronal injury; (B) Microglial NLRP3 inflammasome activation. Periodontal-derived inflammatory signals, including LPS, may engage TLR4 on microglia, activate NF-κB, and prime NLRP3 inflammasome components. ROS accumulation and ionic fluxes, such as K+ efflux, may promote assembly of the inflammasome complex (NLRP3, ASC, and pro-caspase-1), leading to caspase-1 activation and maturation of IL-1β, thereby intensifying neuroinflammation. This response may be further amplified by IFN-γ signaling and downstream cytokines such as TNF-α; (C) Metabolic vulnerability linking oxidative stress to ferroptosis. Reduced G6PD activity may limit NADPH/GSH-dependent antioxidant capacity, thereby facilitating ferrous iron-driven lipid peroxidation and ferroptotic cell death. This pathway highlights a potential convergence of redox imbalance, iron dysregulation, and periodontal inflammation-associated neurodegenerative susceptibility. PD: Parkinson’s disease; α-syn: α-synuclein; pSer129: phospho-Ser129; Kgp: lysine-gingipain; Rgp: arginine-gingipain; ROS: reactive oxygen species; LPS: lipopolysaccharide; TLR4: Toll-like receptor 4; NF-κB: nuclear factor kappa B; NLRP3: NOD-, LRR-, and pyrin domain-containing protein 3; ASC: apoptosis-associated speck-like protein containing a CARD; IL-1β: interleukin-1β; IFN-γ: interferon-γ; TNF-α: tumor necrosis factor-α; G6PD: glucose-6-phosphate dehydrogenase; NADPH: nicotinamide adenine dinucleotide phosphate; GSH: glutathione.
Immune dysregulation and neuroinflammation
Immune dysregulation is one of the most convincing conceptual bridges between periodontitis and PD. Periodontitis is characterized by sustained activation of innate and adaptive immune pathways in response to a dysbiotic biofilm, whereas PD increasingly appears to involve both peripheral and central immune activation, microglial priming, and chronic neuroinflammatory signaling[19,23-30]. A coherent working model is that chronic periodontal inflammation increases systemic inflammatory burden and immune activation, which may in turn lower the threshold for neuroinflammatory amplification in vulnerable nigrostriatal circuits[10,23,26-30].
Clinical observations support this concept, albeit indirectly. In a cross-sectional analysis of two American PD cohorts, self-reported periodontitis was associated with higher circulating high-sensitivity C-reactive protein (hs-CRP), suggesting that periodontal disease may further increase systemic inflammatory load in PD[23]. This is consistent with broader evidence linking periodontitis to low-grade systemic inflammation[9-11].
More direct support comes from experimental studies. Bai et al. reported that oral pathogens exacerbated motor dysfunction and dopaminergic injury in MPTP-treated mice while increasing Th1-cell infiltration in the brain, cervical lymph nodes, ileum, and colon; importantly, neutralization of interferon-γ (IFN-γ) attenuated neuronal loss, implicating a Th1-IFN-γ-microglia axis[19]. This finding is mechanistically important because it connects oral infection not only to systemic inflammation, but also to adaptive immune polarization and central glial activation.
Bioinformatics studies further suggest shared inflammatory architectures between PD and periodontitis. Hu et al. identified FMNL1, MANSC1, PLAUR, RNASE6, and TCIRG1 as potential crosstalk genes linking the two disorders[24]. A separate study by Wen et al. also identified common molecular biomarkers and immune-related pathways shared by PD and chronic periodontitis[25]. These findings are hypothesis-generating rather than definitive, but they support the notion that shared immune and inflammatory networks may underlie the overlap between periodontal inflammation and neurodegeneration.
BBB dysfunction, aging, and peripheral-to-central signaling
Aging is the strongest risk factor for PD and also strongly influences oral health, immune regulation, and barrier integrity[1,9,28]. Blood-brain barrier (BBB) dysfunction has become an increasingly important topic in PD because barrier breakdown may allow greater trafficking of inflammatory mediators, microbial products, and immune cells into the central nervous system[27-29]. Reviews have highlighted that BBB alterations in PD can interact with α-syn pathology, oxidative stress, and inflammation, thereby facilitating neurodegenerative progression[27-29].
This concept is particularly relevant to periodontitis. Chronic periodontal inflammation can sustain peripheral cytokine production and repeated exposure to microbial products, which in an aging host may be more likely to influence the central nervous system because of impaired immune homeostasis and altered BBB resilience[10,26-29]. Bendig et al. emphasized that aging-related changes in vulnerable neurons, the immune system, and the BBB may collectively shape PD susceptibility, making peripheral inflammatory sources more relevant in older adults[28].
Oxidative stress and ferroptosis
Oxidative stress is a convergent process in both PD and periodontitis. In PD, dopaminergic neurons are particularly vulnerable to reactive oxygen species because of high metabolic demand, dopamine auto-oxidation, mitochondrial dysfunction, and impaired antioxidant defenses[1-3,30,31]. In periodontitis, persistent activation of neutrophils and macrophages within inflamed periodontal tissues generates sustained reactive oxygen species production and local oxidative damage, with potential systemic spillover[9,10,23,30].
Ferroptosis - an iron-dependent form of regulated cell death driven by lipid peroxidation - has emerged as an important framework for understanding dopaminergic degeneration in PD[30,31]. Reviews have highlighted the importance of iron dyshomeostasis, glutathione depletion, glutathione peroxidase 4 dysfunction, mitochondrial damage, and lipid reactive oxygen species accumulation in PD-related ferroptotic injury[30,31] . This concept can be linked back to periodontitis in several ways. Chronic periodontal inflammation may increase systemic oxidative burden, alter redox signaling, and sustain inflammatory cytokine exposure that sensitizes neurons to lipid peroxidation. In addition, pathogen-associated inflammation may disturb iron handling and mitochondrial function, thereby lowering the threshold for ferroptotic neuronal death[10,21,22,30,31]. At present, direct experimental evidence that periodontal inflammation triggers ferroptosis in nigral neurons is still limited, but the model is biologically coherent and worthy of dedicated testing. As illustrated in Figure 3, redox imbalance, inflammasome activation, and iron-dependent lipid peroxidation may converge to enhance dopaminergic neuronal vulnerability.
Shared modifiers: vitamin D and diet
Reviewer concerns about vitamin D and diet are well founded and should be explicitly addressed. Systematic reviews and meta-analyses have shown that serum vitamin D levels are lower in people with periodontitis, and vitamin D has recognized roles in bone metabolism, immune modulation, and host defense relevant to periodontal stability[32-34]. Separate reviews and meta-analyses have also reported lower vitamin D levels in PD and suggested associations between low vitamin D status, symptom severity, and PD risk, although causal inference and intervention efficacy remain uncertain[35-37].
Diet should also be considered explicitly. Reviews of PD indicate that dietary patterns may influence disease risk and symptom burden through metabolic, inflammatory, and microbiome-related pathways[38]. Likewise, systematic reviews in periodontology increasingly suggest that dietary patterns and micronutrient intake may influence periodontal inflammation and disease susceptibility[41,42]. Therefore, future studies on PD and periodontitis should not treat diet and vitamin D merely as nuisance variables; they may represent shared biological modifiers and potential intervention targets.
CONCLUSION
Current evidence supports a complex and likely asymmetric relationship between periodontitis and PD. The more robust clinical observation is that patients with PD are at increased risk of poor periodontal health because motor dysfunction, dysphagia, xerostomia, cognitive decline, and reduced self-care compromise oral hygiene and alter the oral ecosystem[4-8,39,40]. By contrast, the proposition that periodontitis contributes to PD onset or progression is biologically plausible and supported by selected epidemiological studies, experimental work, and mechanistic reviews, but the overall human evidence remains mixed and cannot yet establish causality[9,11-16].
The most compelling mechanistic links involve oral dysbiosis, chronic peripheral inflammation, pathogen-associated immune activation, BBB vulnerability, oxidative stress, and possible effects on α-syn biology[10,17-31]. Among periodontal pathogens, P. gingivalis and its gingipains are of particular interest because they may connect periodontal disease to neuroinflammatory and proteostatic pathways relevant to PD[10,20-22]. At the same time, shared modifiers such as aging, multimorbidity, vitamin D status, and diet may partly explain the observed epidemiological overlap and should be systematically measured in future studies[28,32-38,41,42].
Future work should prioritize well-phenotyped longitudinal cohorts, standardized periodontal definitions, objective oral function measures, multi-omics profiling, and interventional studies assessing whether periodontal treatment can alter systemic inflammation, oral dysbiosis, or PD-related outcomes. From a clinical perspective, oral-health assessment and periodontal management should be integrated into comprehensive PD care, not only to improve quality of life and nutrition, but also because periodontal inflammation may represent a modifiable contributor to disease-related biological stress.
DECLARATIONS
Authors’ contributions
Writing and drafting of the article: Wang Z
Editing of the article: Zou X
Availability of data and materials
Not applicable.
AI and AI-assisted tools statement
During the preparation of this manuscript, the AI tool Gemini (version 2.5 Pro, released 2025-03-25) was used solely for image creation for the figures and Graphic Abstract. The tool did not influence the study design, data collection, analysis, interpretation, or the scientific content of the work. All authors take full responsibility for the accuracy, integrity, and final content of the manuscript.
Financial support and sponsorship
This work is supported by the 2025 Medical Science and Technology Project of the Sichuan Provincial Health Commission (25LCYJ41), and the Graduate Research and Innovation Fund of Chengdu Medical College (YCX2025-01-92).
Conflicts of interest
Both authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Ben-Shlomo Y, Darweesh S, Llibre-Guerra J, Marras C, San Luciano M, Tanner C. The epidemiology of Parkinson’s disease. Lancet. 2024;403:283-92.
4. Verhoeff MC, Eikenboom D, Koutris M, et al. Parkinson’s disease and oral health: a systematic review. Arch Oral Biol. 2023;151:105712.
5. Auffret M, Meuric V, Boyer E, Bonnaure-Mallet M, Vérin M. Oral health disorders in Parkinson’s disease: more than meets the eye. J Parkinsons Dis. 2021;11:1507-35.
6. Zlotnik Y, Balash Y, Korczyn AD, Giladi N, Gurevich T. Disorders of the oral cavity in Parkinson’s disease and parkinsonian syndromes. Parkinsons Dis. 2015;2015:379482.
7. Špiljak B, Lisak M, Pašić H, Trkanjec Z, Lovrenčić Huzjan A, Bašić Kes V. Sialorrhea and xerostomia in Parkinson’s disease patients. Acta Clin Croat. 2022;61:320-6.
8. Kaur T, Uppoor A, Naik D. Parkinson’s disease and periodontitis - the missing link? A review. Gerodontology. 2016;33:434-8.
9. Plachokova AS, Gjaltema J, Hagens ERC, et al. Periodontitis: a plausible modifiable risk factor for neurodegenerative diseases? A comprehensive review. Int J Mol Sci. 2024;25:4504.
10. Huang Z, Hao M, Shi N, et al. Porphyromonas gingivalis: a potential trigger of neurodegenerative disease. Front Immunol. 2025;16:1482033.
11. Zhao Y, Zhang C, Chang X, et al. Causal association between periodontitis and systemic diseases: a systematic review and meta-analysis of mendelian randomization studies. BMC Oral Health. 2026;26:383.
12. Chen Y, Jin Y, Li K, et al. Is there an association between Parkinson’s disease and periodontitis? A systematic review and meta-analysis. J Parkinsons Dis. 2023;13:1107-25.
13. Chen CK, Wu YT, Chang YC. Periodontal inflammatory disease is associated with the risk of Parkinson’s disease: a population-based retrospective matched-cohort study. PeerJ. 2017;5:e3647.
14. Jeong E, Park JB, Park YG. Evaluation of the association between periodontitis and risk of Parkinson’s disease: a nationwide retrospective cohort study. Sci Rep. 2021;11:16594.
15. Lee NE, Yoo DM, Han KM, et al. Investigating the connection between chronic periodontitis and Parkinson’s disease: findings from a Korean National Cohort Study. Biomedicines. 2024;12:792.
16. Botelho J, Machado V, Mendes JJ, Mascarenhas P. Causal association between periodontitis and Parkinson’s disease: a bidirectional Mendelian randomization study. Genes. 2021;12:772.
17. Yay E, Yilmaz M, Toygar H, et al. Parkinson’s disease alters the composition of subgingival microbiome. J Oral Microbiol. 2023;15:2250650.
18. Yay E, Yilmaz M, Toygar H, et al. Oral and gut microbial profiling in periodontitis and Parkinson’s disease. J Oral Microbiol. 2024;16:2331264.
19. Bai XB, Xu S, Zhou LJ, et al. Oral pathogens exacerbate Parkinson’s disease by promoting Th1 cell infiltration in mice. Microbiome. 2023;11:254.
20. Ermini F, Low VF, Song JJ, et al. Ultrastructural localization of Porphyromonas gingivalis gingipains in the substantia nigra of Parkinson’s disease brains. NPJ Parkinsons Dis. 2024;10:90.
21. Li D, Ren T, Li H, Liao G, Zhang X. Porphyromonas gingivalis: a key role in Parkinson’s disease with cognitive impairment? Front Neurol 2022;13:945523.
22. Feng YK, Wu QL, Peng YW, et al. Oral P. gingivalis impairs gut permeability and mediates immune responses associated with neurodegeneration in LRRK2 R1441G mice. J Neuroinflammation. 2020;17:347.
23. Lyra P, Botelho J, Machado V, et al. Self-reported periodontitis and C-reactive protein in Parkinson’s disease: a cross-sectional study of two American cohorts. NPJ Parkinsons Dis. 2022;8:40.
24. Hu S, Li S, Ning W, et al. Identifying crosstalk genetic biomarkers linking a neurodegenerative disease, Parkinson’s disease, and periodontitis using integrated bioinformatics analyses. Front Aging Neurosci. 2022;14:1032401.
25. Wen Z, Zhao M, Liu P, Wang Y, Xu J, Wu T. Elucidation of common molecular diagnostic biomarkers between chronic periodontitis and Parkinson’s disease via bioinformatics analyses. J Periodontal Res. 2023;58:1212-22.
26. Isik S, Yeman Kiyak B, Akbayir R, Seyhali R, Arpaci T. Microglia mediated neuroinflammation in Parkinson’s disease. Cells. 2023;12:1012.
27. Kwon HS, Koh SH. Neuroinflammation in neurodegenerative disorders: the roles of microglia and astrocytes. Transl Neurodegener. 2020;9:42.
28. Bendig J, Frank A, Reichmann H. Aging and Parkinson’s disease: a complex interplay of vulnerable neurons, the immune system and the blood-brain barrier. Ageing Neur Dis. 2024;4:5.
29. Lau K, Kotzur R, Richter F. Blood-brain barrier alterations and their impact on Parkinson’s disease pathogenesis and therapy. Transl Neurodegener. 2024;13:37.
30. Ding XS, Gao L, Han Z, et al. Ferroptosis in Parkinson’s disease: molecular mechanisms and therapeutic potential. Ageing Res Rev. 2023;91:102077.
31. Mahoney-Sánchez L, Bouchaoui H, Ayton S, Devos D, Duce JA, Devedjian JC. Ferroptosis and its potential role in the physiopathology of Parkinson’s disease. Prog Neurobiol. 2021;196:101890.
32. Machado V, Lobo S, Proença L, Mendes JJ, Botelho J. Vitamin D and periodontitis: a systematic review and meta-analysis. Nutrients. 2020;12:2177.
33. Liang F, Zhou Y, Zhang Z, Zhang Z, Shen J. Association of vitamin D in individuals with periodontitis: an updated systematic review and meta-analysis. BMC Oral Health. 2023;23:387.
34. Shah M, Poojari M, Nadig P, et al. Vitamin D and periodontal health: a systematic review. Cureus. 2023;15:e47773.
35. Rimmelzwaan LM, van Schoor NM, Lips P, Berendse HW, Eekhoff EM. Systematic review of the relationship between vitamin D and Parkinson’s disease. J Parkinsons Dis. 2016;6:29-37.
36. Fullard ME, Duda JE. A review of the relationship between vitamin D and Parkinson disease symptoms. Front Neurol. 2020;11:454.
37. Zhou Z, Zhou R, Zhang Z, Li K. The association between vitamin D status, vitamin D supplementation, sunlight exposure, and Parkinson’s disease: a systematic review and meta-analysis. Med Sci Monit. 2019;25:666-74.
38. Anwar L, Ahmad E, Imtiaz M, Ahmad M, Faisal Aziz M, Ibad T. The impact of diet on Parkinson’s disease: a systematic review. Cureus. 2024;16:e70337.
39. Yilmaz M, Yay E, Balci N, et al. Parkinson’s disease is positively associated with periodontal inflammation. J Periodontol. 2023;94:1425-35.
40. Lyra P, Machado V, Proença L, et al. Parkinson’s disease, periodontitis and patient-related outcomes: a cross-sectional study. Medicina. 2020;56:383.
41. Shi X, Zhu P, Du M, et al. Dietary patterns and periodontitis: a systematic review. J Periodontal Res. 2025;60:300-14.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0













Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].