


Addressing unanswered questions in transcatheter aortic valve replacement: lifetime management, leaflet modification, and cerebral protection
 0
0 Abstract
Transcatheter aortic valve replacement (TAVR) has rapidly evolved from a therapy reserved for high-risk surgical candidates to a preferred treatment option across a broad range of patients with severe aortic stenosis. Contemporary randomized trials have demonstrated comparable or superior early outcomes to surgical aortic valve replacement (SAVR), leading to expanded indications in intermediate- and low-risk populations, as well as select patients with bicuspid anatomy. Recent guideline updates, including the 2025 European Society of Cardiology recommendations, unify the age threshold for TAVR to ≥ 70 years in appropriately selected patients and support consideration of early intervention in asymptomatic severe aortic stenosis based on emerging evidence. As younger patients increasingly undergo TAVR, several key uncertainties have become central to clinical decision-making. Long-term valve durability beyond the first decade remains insufficiently defined, emphasizing the need for structured lifetime management strategies that account for anticipated reinterventions, prosthesis-patient mismatch, and coronary access preservation. The rise in valve-in-valve and redo-TAVR procedures introduces complex anatomical challenges, including coronary obstruction and sinus sequestration, which has driven the development of advanced leaflet-modification techniques. In parallel, the role of cerebral embolic protection (CEP) remains uncertain, as randomized trials have demonstrated neutral results, leading to ongoing investigation into which patients may benefit and which technologies may offer meaningful protection. This review synthesizes current evidence and unresolved questions in three domains essential to contemporary TAVR practice: lifetime management, leaflet modification strategies, and CEP.
Keywords
INTRODUCTION
Transcatheter aortic valve replacement (TAVR) has transformed the management of severe aortic stenosis over the past decade. Initially restricted to patients deemed high risk surgical candidates, TAVR is now considered an effective therapy in intermediate and low risk cohorts, as supported by randomized controlled trials demonstrating comparable or superior early outcomes compared to surgical aortic valve replacement (SAVR). As a result, TAVR is now being increasingly offered to lower-risk and younger populations, as well as those with suitable anatomy, including some with bicuspid valves[1].
This paradigm shift is reflected in the 2020 American College of Cardiology (ACC)/American Heart Association (AHA) guidelines, which support either TAVR or SAVR in patients aged 65-80 years, while favoring SAVR in those younger than 65 years and recommending TAVR in patients aged 80 years or older[2].
The prior European Society of Cardiology (ESC) 2021 guidelines recommend TAVR for patients aged ≥ 75 years or those at increased surgical risk, with SAVR favored in younger, low-risk patients. Both guidelines emphasized the importance of a multidisciplinary heart team and individualized decision-making[3].
ESC guidelines released in 2025 introduced a few major updates[4].
1. Lowering the age threshold for TAVR to ≥ 70 years for patients with tricuspid aortic valve stenosis and suitable anatomy, irrespective of surgical risk.
2. Considering intervention in asymptomatic patients with severe, high-gradient aortic stenosis and preserved left ventricular ejection fraction (LVEF; ≥ 50%), as an alternative to surveillance, if procedural risk is low.
For asymptomatic patients with severe, high gradient aortic stenosis and preserved LVEF (≥ 50%), intervention (either TAVR or SAVR) can be considered if the procedural risk is low, confirmed by a normal exercise test with absence of symptoms. This recommendation is supported by recent trials including EARLY TAVR, EVOLVED, AVATAR, and RECOVERY[5-8]. The EARLY TAVR trial demonstrated that TAVR in truly asymptomatic patients reduced the composite of death, stroke, or unplanned cardiovascular hospitalization compared to surveillance, with better quality of life and cardiac function[5]. The EVOLVED, AVATAR, and RECOVERY trials (SAVR-focused) showed mixed mortality benefits but consistently reduced heart failure symptoms and hospitalizations with early intervention, particularly in select high risk or younger cohorts[6-8].
TAVR is now being recommended in patients ≥ 70 years of age with tricuspid aortic valve stenosis and suitable anatomy, regardless of surgical risk, as supported by evidence from the DEDICATE and NOTION 2 trials[9,10]. This marks a significant shift toward broader eligibility and earlier intervention, aiming to prevent irreversible cardiac damage and improve outcomes.
Nevertheless, bicuspid aortic valve anatomy remains an important area of ongoing uncertainty. Although growing observational experience supports the feasibility of TAVR in selected bicuspid anatomies, these patients were underrepresented in pivotal randomized trials, and certain anatomical features, including markedly elliptical annuli, asymmetric bulky calcification, raphe calcification, and associated aortopathy, may increase procedural complexity and adverse outcomes. Accordingly, contemporary guidelines continue to emphasize individualized Heart Team assessment, with bicuspid morphology remaining an important consideration that may favor SAVR in selected patients.
Despite this momentum, several questions remain unanswered. Many landmark trials on TAVR have limited long-term follow-up, with valve durability remaining a significant concern in younger patients who may require multiple lifetime interventions. Similarly, the increasing prevalence of redo-TAVR (TAV-in-TAV) procedures not only introduces new technical challenges but also increases concerns for increased risk of coronary obstruction. Furthermore, the role of cerebral embolic protection (CEP) remains unclear after two large, randomized controlled trials failed to demonstrate clear benefit.
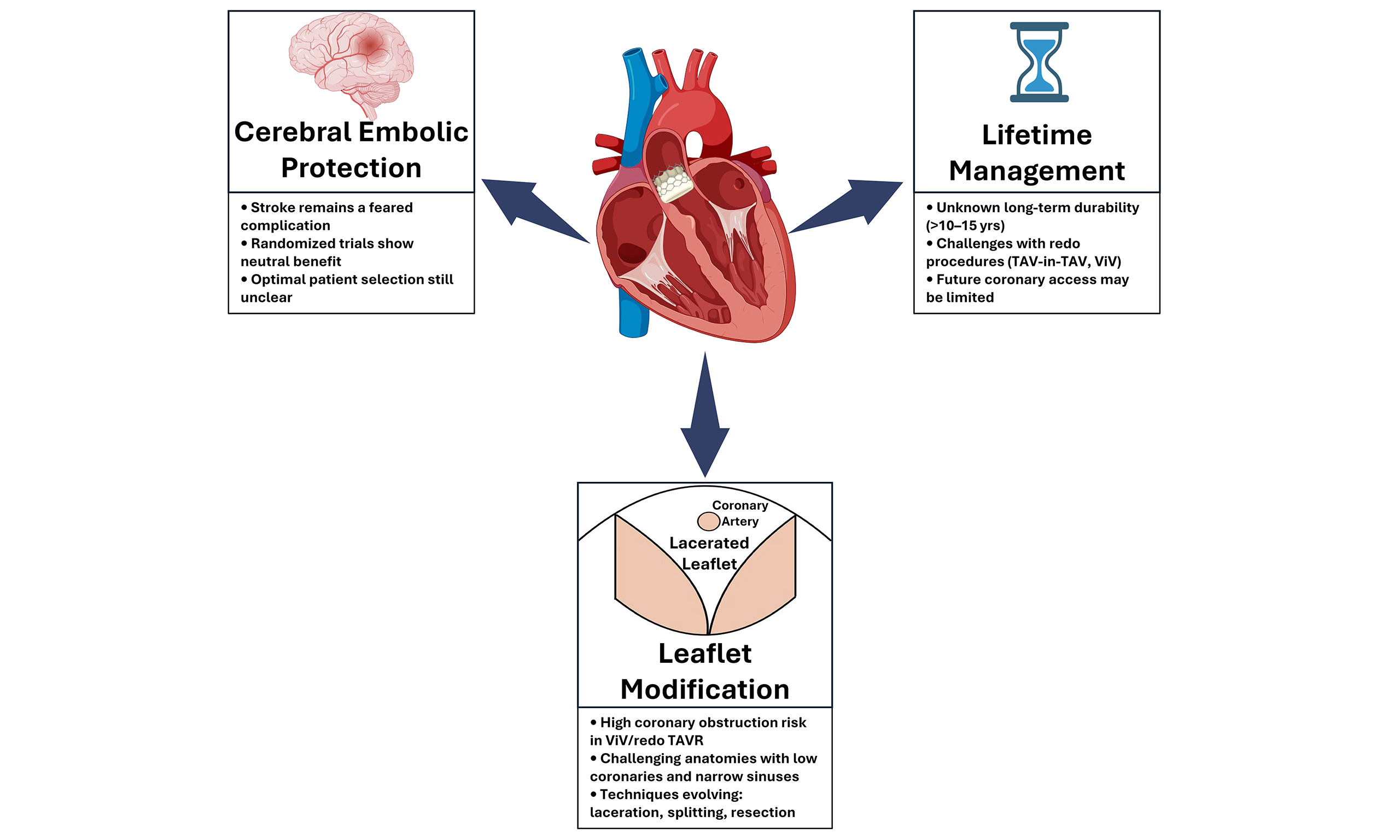
This review focuses on three major areas central to the ongoing discourse in current TAVR practice: lifetime management strategies, leaflet modification techniques to minimize coronary obstruction during redo procedures, and the role of CEP.
LIFETIME MANAGEMENT OF AORTIC STENOSIS
Durability of aortic valve prostheses remains the cornerstone of lifetime management strategies. Randomized trials and observational studies have progressively increased the follow-up data available for transcatheter heart valves (THVs). Current pooled analyses to mid‑term follow‑up show no consistent increase in clinically significant structural valve deterioration after TAVR compared to surgical bioprosthetic valves. Similarly, meta‑analyses and comparative studies with up to 5 years of follow-up have shown similar rates of echocardiographic valve deterioration and clinically driven reintervention between TAVR and SAVR patients[11,12]. Longer observational follow‑up in selected cohorts offers additional reassurance: early TAVR series and randomized studies now show stable valve hemodynamics and low rates of clinically significant structural valve deterioration in up to 8 to 10 years in some patient populations[13,14]. Overall, these datasets from randomized trials and real-world registries have been synthesized in reviews and lifetime management analyses to reach an optimistic albeit cautious view that modern TAVR prostheses show durability comparable to that of surgical bioprostheses during the first decade after implantation.
The 7-year follow-up of the PARTNER 3 trial shows that TAVR in low-risk patients with severe, symptomatic aortic stenosis provides reassuring long-term outcomes[15]. There were no significant differences compared to SAVR in the composite endpoints of death, stroke, or rehospitalization. The individual event rates were also similar, and valve durability was comparable, with valve failure rates of 6.9% for TAVR and 7.3% for surgery at 7 years. Valve gradients remained stable, and patients in both groups maintained good functional status.
Early benefits of TAVR, such as reduced rehospitalization and lower rates of new-onset atrial fibrillation, were observed to become less pronounced over time. While late events, such as stroke and rehospitalization, were slightly more common in the TAVR group, although not statistically significant. Paravalvular regurgitation occurred more often after TAVR but did not affect mortality or valve durability. Overall, these findings support the use of TAVR as an effective alternative to surgery in appropriately selected low-risk patients, with similar long-term clinical and valve-related outcomes.
Nevertheless, long-term outcomes after TAVR are influenced by factors beyond structural valve durability alone. Large observational registries have reported more heterogeneous late clinical outcomes than contemporary randomized trials, likely reflecting broader patient complexity and comorbidity burden encountered in real-world practice[16-18]. In addition, factors such as paravalvular regurgitation and conduction disturbances requiring permanent pacemaker implantation may also impact long-term survival and rehospitalization after TAVR[19,20].
When evaluating a patient with native aortic stenosis, it is important to consider the possibility of future valve procedures, particularly in younger patients whose life expectancy may exceed the durability of bioprosthetic or transcatheter valves.
The initial choice between surgical and transcatheter valve replacement should be guided by factors such as age, comorbidities, valve anatomy, and the feasibility of future valve-in-valve (ViV) or TAVR-in-TAVR procedures. For example, younger patients and those with complex anatomy may require careful planning to facilitate future interventions, including the selection of valve type and implantation strategy.
The ACC guidelines and recent expert reviews emphasize that lifetime management of aortic stenosis should anticipate the need for second or even third interventions, given the risk of structural valve deterioration and evolving procedural options. Technical challenges such as patient–prosthesis mismatch, coronary access, and long-term device durability must be considered, especially as long-term data beyond 10 years remain limited[21].
The following summarizes the current expert opinion on this subject matter:
1. Life Expectancy > 30 Years: For younger patients requiring a definitive solution, the Ross procedure or mechanical SAVR is often favored. These options offer the highest long-term freedom from structural failure, avoiding the cumulative risk of multiple redo procedures.
2. Life Expectancy 20-30 Years: This intermediate group requires individualized Heart Team evaluation. A “SAVR-first” approach (potentially with root enlargement) is reasonable when maximizing the initial valve size is important to keep future TAVR options open. Conversely, a “TAVR-first” strategy is viable if anatomy supports a feasible future ViV procedure.
3. Life Expectancy < 20 Years: For patients with more limited life expectancy, TAVR is increasingly considered a reasonable first strategy in appropriately selected patients. Although robust long-term durability data beyond the first decade remain limited, current evidence suggests acceptable mid- to long-term valve performance, and if valve failure occurs, TAV-in-TAV may remain a feasible reintervention strategy in selected anatomies.
4. Patients with small aortic annuli present a specific challenge due to the risk of patient-prosthesis mismatch (PPM). In these patients, the goal is to implant at least a 23 mm valve, as this is commonly believed to be the minimum size required for successful deployment of a future ViV prosthesis. In these cases, when surgical risk is appropriate, SAVR with root enlargement is often preferred over TAVR. Root enlargement facilitates the implantation of a larger prosthesis, optimizing hemodynamics and creating a superior landing zone for future ViV procedures. Conversely, TAVR in small annuli increases the risk of high residual gradients and coronary obstruction during future interventions.
As TAVR indications expand to younger patients with longer life expectancies, the management of valve failure has become a major concern. Population-level simulation models now predict a significant rise in redo-TAVR procedures over the next decade. This projected surge is driven by a consistent annual volume of bioprosthetic SAVRs (approximately 50,000 per year), and the rapidly growing number of TAVR patients. Current models use a bimodal failure pattern for TAVR valves estimating about 20% failing or in 4 years and the remaining 80% around 11.5 years. This suggests ongoing structural valve deterioration at the population level. As early TAVR and SAVR patients reach these expected failure points, health systems must prepare for a rapidly growing pool of ViV candidates and technical solutions available to match technically challenging anatomical scenarios[22].
Technical planning for redo-TAVR is more complex than TAVR in native valves and requires individualized planning strategies given the fact that the interaction between the first valve frame and the second implant creates specific geometric risks. The main concerns are coronary obstruction and sinus sequestration, which become more challenging because of variability in TAV designs and frame heights[23]. Available clinical data suggest that overt coronary obstruction during redo-TAVR is uncommon, with retrospective series reporting rates of approximately 0% to 0.9%[24,25]. In contrast, computed tomography (CT)-based simulation studies have identified substantially higher anatomical risk of coronary obstruction or sinus sequestration in selected TAV-in-TAV configurations, with estimated risks ranging from approximately 23% to 45% depending on valve combination and patient-specific anatomy[26,27]. While certain valve design characteristics, such as frame height and leaflet position, may influence neoskirt geometry during redo-TAVR, the risk of coronary obstruction and sinus sequestration varies substantially between patients and valve combinations, and each TAV-in-TAV configuration presents unique anatomical considerations. Factors including implantation depth, commissural alignment, sinotubular junction anatomy, and patient-specific CT measurements also contribute to procedural risk assessment. Accordingly, individualized CT planning remains central to procedural strategy selection in TAV-in-TAV procedures.
Coronary obstruction occurs when the “neoskirt” of the second valve, along with the displaced leaflets of the first valve impinges on the coronary ostia. The risk increases when there is significant leaflet overhang, poor commissural alignment, or a short valve to aorta distance at the sinotubular junction[23].
Sinus sequestration is where the “neoskirt” extends above the sinotubular junction, sealing off the aortic sinus and blocking coronary flow. This is particularly prominent in “short-in-tall” valve setups or when using supra-annular index valves with high implantation depths[23]. Because of these risks, multiphase CT planning is essential to quantify valve to coronary distance, valve-to-aorta distance, and commissural alignment/orientation. Unfortunately, there is no “one-size-fits-all” approach. Each plan must be customized based on how the first valve expands and the second valve geometry/design.
LEAFLET MODIFICATION
As TAVR expands into younger populations and in more complex reintervention scenarios, managing coronary access and preventing coronary obstruction has become increasingly important. Coronary obstruction is a rare but catastrophic complication of TAVR, and it occurs more often in ViV and Redo-TAVR cases.
It is usually caused by the expanding transcatheter valve pushing the native or surgical leaflets outward. In patients with high-risk anatomy, such as low coronary ostial height, small sinuses of Valsalva, or a short valve-to-coronary (VTC) distance, the displaced leaflets can block the coronary arteries or sequester the sinus, leading to rapid hemodynamic collapse[28].
Historically, “chimney” or “snorkel” stenting was the main bailout strategy for high-risk cases[29,30]. However, this method is now seen as suboptimal because it carries risks of stent crush, thrombosis, and difficult future coronary access. As a result, the field has shifted toward preventive leaflet-modification techniques, which reshape the leaflet geometry before valve implantation, ensuring a patent pathway for coronary blood flow.
The Established Standard: BASILICA. The first technique to gain widespread acceptance and clinical adoption was BASILICA (Bioprosthetic or Native Aortic Scallop Intentional Laceration to prevent Iatrogenic Coronary Artery obstruction). Developed at the National Heart, Lung, and Blood Institute (NHLBI), this procedure utilizes standard catheterization tools to perform electrosurgical laceration. The technique involves traversing the target leaflet with an electrified guidewire, which is then captured by a snare in the left ventricular outflow tract (LVOT). By applying radiofrequency energy to the wire loop, the operator slices through the leaflet tissue from base to tip[31].
The functional goal of BASILICA is to create a “splay”. Upon deployment of the THV, the lacerated leaflet halves separate laterally, creating a triangular space that preserves blood flow to the coronary artery. The BASILICA trial and later registries have shown strong proof-of-concept, with high procedural success and effective prevention of obstruction in high-risk anatomies[31]. However, BASILICA remains technically demanding. It requires complex catheter manipulation, creating an “electrosurgical loop”, and precise snaring in the LVOT, which introduces a significant learning curve and prolongs procedure times. Furthermore, while effective, the resulting “splay” may still be insufficient in cases with extremely bulky leaflets or severely constrained sinuses.
Recognizing the technical limitations of the off-label BASILICA technique, industry innovation has focused on dedicated devices that standardize and simplify leaflet modification. TELLTALE represents the next generation of electrosurgical solutions. It is a purpose-built system designed to integrate the wire traversal and laceration steps into a single dedicated platform. By eliminating the need for BASILICA’s complex setup using off-the-shelf tools, TELLTALE significantly simplifies the procedure. Recent trial data shows that this device can achieve 100% technical success with a robust safety profile, making it easier for operators to use prophylactic leaflet modification in challenging cases[32].
Alongside electrosurgical advances, the ShortCut device introduces a mechanical alternative. Unlike BASILICA or TELLTALE, ShortCut does not rely on radiofrequency energy. Instead, it utilizes a mechanical cutting element to split the leaflet. This approach addresses specific safety concerns associated with electrosurgery, such as thermal injury to surrounding structures or electromagnetic interference. The pivotal ShortCut study demonstrated that mechanical splitting is effective, offering an alternative that may be preferable in patients with specific anatomical limitations or for operators less comfortable with electrosurgical setups[33].
While splitting techniques (laceration) are effective for many patients, a linear split may not suffice in the most challenging anatomies. In cases of “Short-to-Tall” ViV procedures or extremely effaced sinuses, a split leaflet can still prolapse and obstruct the coronary ostium (sinus sequestration). This limitation has driven the development of “Annihilation” and “Resection” technologies, which aim to remove or destroy leaflet tissue rather than just dividing it.
UNICORN (Undermining Iatrogenic Coronary Obstruction with Radiofrequency Needle) and its variants represent this “annihilation” technique. Rather than a single cut, these techniques use a combination of radiofrequency traversal and balloon maceration to disintegrate a portion of the leaflet structure. The goal is to create a wide window in the leaflet rather than a slit. Preliminary preclinical and early clinical experience suggests that “annihilation” techniques may provide a larger safety margin in selected high-risk anatomies; however, current evidence remains limited, and further validation is required before broader adoption can be recommended[34-36].
Finally, the frontier of leaflet modification lies in true percutaneous resection, as seen with early technologies like TRESECT (TreSquare Technologies). This device aims to replicate the surgical “cut-and-sew” standard by physically resecting and capturing the native or bioprosthetic leaflet. By removing the leaflet entirely from the body, TRESECT eliminates the obstruction source rather than just displacing it. While still in its early phases of investigation, it offers a theoretical technique ideal for lifetime management, potentially allowing TAVR to more closely approximate the hemodynamic and anatomical results of surgical valve replacement[37]. Notably, its procedural feasibility, and reproducibility remain largely undefined and require further study.
CEP
Stroke remains one of the most feared complications of TAVR, with estimated rates of approximately 2%-3% despite significant improvements in valve systems and operator experience over the years. To address this, CEP devices were developed to capture or deflect debris dislodged during the procedure. Potential high-risk phenotypes that may derive greater benefit from selective CEP use include patients with severe valvular or aortic arch calcification, bulky leaflet calcium, complex aortic arch atheroma, ViV or redo-TAVR procedures, bicuspid valve anatomy, and cases requiring extensive device manipulation or adjunctive interventions. These anatomical and procedural features are believed to increase embolic burden during TAVR and may represent more appropriate targets for future risk-enriched CEP trials. Although the rationale behind CEP is strong and it can reliably capture debris in nearly all patients, showing a clear clinical benefit has been a challenge.
Two pivotal randomized trials PROTECTED TAVR and BHF PROTECT-TAVI found no statistically significant difference in the primary outcome of stroke within 72 h or before discharge between patients treated with CEP and those without[38,39]. In PROTECTED TAVR, stroke rates were 2.3% (CEP) vs. 2.9% (control), and in BHF PROTECT-TAVI, 2.1% (CEP) vs. 2.2% (control), with no meaningful reduction in disabling stroke or mortality. These findings are consistent across both trials and are reinforced by recent meta-analyses and systematic reviews, which show no statistically significant reduction in stroke, disabling stroke, or mortality with CEP use in randomized controlled settings[38,39].
A recent meta-analysis comprised a total of 10,635 patients, representing the largest randomized dataset on embolic protection ever assembled. The primary analysis was conducted on a modified intention-to-treat (mITT) population (N = 10,580), which included all randomized participants in whom the TAVR procedure was attempted.
The results for the primary endpoint (incidence of all stroke at 72 h or hospital discharge) were neutral. The stroke rate was 2.3% in the control arm (N = 5,293) compared to 2.2% in the CEP arm (N = 5,287), resulting in a non-significant risk difference of -0.1% (P = 0.641). Similarly, the analysis for the secondary endpoint of disabling stroke also failed to show statistical significance in the mITT population. The rate was 1.3% in the control group vs. 1.0% in the CEP group, yielding a P-value of 0.090. Based on these data, there is no evidence that a routine strategy of CEP is effective in reducing overall or disabling stroke in the TAVR population.
Despite the neutral primary outcomes, a significant controversy emerged regarding the Per-Protocol analysis. This analysis was restricted to patients who received the intervention exactly as intended i.e specifically, those in whom the CEP device was successfully deployed with both filters in place (83.4% of cohort). In this subgroup (N = 9,663), CEP use appeared to confer a statistically significant benefit. The Per-Protocol analysis showed a significant reduction in all stroke (2.3% vs. 1.7%; P = 0.023) and a robust reduction in disabling stroke (1.3% vs. 0.8%; P = 0.007). Thus, while the per-protocol findings must be interpreted cautiously given the loss of randomization, they nonetheless underscore an important point for device-based therapies: when the device is successfully deployed as intended, a potential clinical benefit may emerge.
Taken together, the null findings in both the modified ITT and CACE analyses suggest that routine use of CEP does not confer a consistent reduction in overall or disabling stroke, and the per-protocol signal, while intriguing, must be interpreted with caution given the inherent selection bias introduced by excluding patients in whom deployment was unsuccessful. Nevertheless, enthusiasm persists within the structural heart community, driven by the biological plausibility of embolic protection and the expectation that the technology should work when applied in the right patients and with reliable device delivery. As such, the current evidence supports a shift in focus toward identifying high-risk phenotypes, optimizing patient selection, and improving deployment success rates rather than broad, all-comer adoption. In parallel, the development of next-generation devices with broader coverage, simplified delivery, and enhanced capture or deflection mechanisms may ultimately be required to realize a meaningful and reproducible clinical benefit.
The current landscape is evolving toward devices designed for broader coverage and easier delivery. ProtEmbo (Protembis) represents the next generation of deflection devices. Unlike current filters, it utilizes a fine-pore mesh canopy deployed at the aortic roof to deflect debris away from all three supra-aortic vessels. One thing to note is that it is designed for delivery via a 6-Fr left radial approach, potentially improving workflow by avoiding femoral congestion[40].
Other novel concepts aim to move beyond simple deflection. Emboliner employs a “capture-and-remove” mechanism, deploying a cylindrical filter that lines the ascending aorta to entrap debris within a sleeve for subsequent removal, rather than redirecting it[41,42]. Similarly, the TriGUARD 3 continues the lineage of arch-deflection devices with a self-expanding mesh designed to cover the entire supra-aortic trunk[43]. Lastly, concepts like CAPTIS and Point-Guard aim for “full-body” filtration, attempting to manage embolic load from the arch and descending aorta to provide global protection[43].
CONCLUSION
The evolution of TAVR over little more than a decade has been remarkable, but its future will depend on how effectively the field addresses the unanswered questions that now accompany its broader use. As TAVR expands into younger, lower-risk populations, the paradigm must shift from procedure-level decision-making to true lifetime planning, anticipating durability constraints, preserving coronary access, and ensuring that each intervention facilitates, rather than limits, the next. Redo-TAVR, once viewed as an uncommon scenario, is now an expected component of long-term care, and its associated challenges have catalyzed the development of sophisticated leaflet-modification technologies designed to mitigate coronary obstruction and sinus sequestration. Similarly, despite biologically compelling rationale, the role of CEP remains unresolved, underscoring the need for more precise patient selection and next-generation devices capable of delivering meaningful clinical benefit. Critical points of these concepts are summarized in Table 1.
Key considerations in TAVR: established knowledge, persistent uncertainties, and emerging directions
| Domain | Established knowledge | Persistent uncertainties | Emerging directions |
| Lifetime management | • Contemporary THVs demonstrate mid-term durability comparable to surgical bioprostheses (up to ~8-10 years) • Index procedural choices, including valve type, size, implantation depth, and commissural alignment, directly influence feasibility of future interventions • Small annuli increase the risk of PPM and challenge long-term planning | • Durability of THVs beyond 12-15 years • Modes and timing of failure for second-/third-generation THVs • Long-term safety and hemodynamics of sequential interventions (e.g., redo-TAVR, ViV) | • CT-based lifetime strategy planning (neo-skirt height, VTC/VTA, commissural alignment modeling) • Anatomically driven “TAVR-first vs. SAVR-first” algorithms • Broader application of surgical root enlargement to preserve future ViV options • THV designs optimized for lifetime reaccess and multiple reinterventions |
| Leaflet modification and coronary protection | • BASILICA demonstrates that controlled leaflet splitting can prevent coronary obstruction in high-risk anatomies • Coronary obstruction risk is significantly higher in ViV and redo-TAVR compared with native TAVR • High-risk anatomical profiles (low coronary height, narrow sinuses, low VTC, tall frames) are well characterized | • Standardized thresholds for when leaflet modification is required • Durability and reproducibility of electrosurgical vs. mechanical approaches • Purpose-built devices (TELLTALE, ShortCut) aimed at simplifying leaflet modification • Standardization of commissural alignment across THV platforms | • Identification of scenarios where laceration is insufficient and resection is needed • “Annihilation” and resection technologies (UNICORN) that may more closely mimic surgical leaflet removal • Next-generation THVs incorporating coronary reaccess considerations in design |
| CEP | • Stroke remains a clinically meaningful adverse event (~2%-3%) • CEP devices consistently capture or deflect debris when deployed • Large RCTs (PROTECTED TAVR, BHF PROTECT-TAVI) show no reduction in overall or disabling stroke in all-comer populations | • Optimal patient subgroups that may benefit from CEP (e.g., heavy calcifications, redo cases, leaflet modifications) • Whether complete arch coverage improves outcomes relative to partial filters • Long-term neurocognitive consequences of microembolization • Trial designs needed to evaluate selective, risk-enriched strategies | • Next-generation deflection and capture systems (ProtEmbo, Emboliner, CAPTIS) with broader coverage • Selective CEP guided by imaging-based embolic risk stratification • Trials assessing neurocognitive and silent infarct outcomes |
Ultimately, the next era of TAVR will be defined not by expanding indications alone, but by how deliberately and safely we navigate the complexities that accompany repeat interventions and longer life expectancy. Integrating high-resolution imaging, individualized procedural planning, and emerging adjunctive technologies will be essential to optimizing outcomes across the patient lifespan. Continued collaboration among clinicians, engineers, and industry partners will be critical to refining these strategies and ensuring that TAVR remains not only a transformative therapy for today’s patients, but a durable, future-ready solution for the next generation.
DECLARATIONS
Acknowledgements
The elements of the graphical abstract were created with BioRender.com.
Authors’ contributions
Contributed equally to the literature review and drafting of the manuscript: Sturla M, Rizvi S, Lin J
Provided conceptual guidance, critical revisions, and expert oversight throughout the development of the manuscript: Sugiura T
All authors reviewed and approved the final version.
Availability of data and materials
Not applicable.
AI and AI-assisted tools statement
During the preparation of this manuscript, the AI tool ChatGPT (version 5.1, released 2025-11-12) was used solely for language editing. The tool did not influence the study design, data collection, analysis, interpretation, or the scientific content of the work. All authors take full responsibility for the accuracy, integrity, and final content of the manuscript.
Financial support and sponsorship
None.
Conflicts of interest
Sugiura T is an Editorial Board Member of Mini-invasive Surgery. Sugiura T was not involved in any stage of the editorial process, including reviewer selection, manuscript handling, or decision-making. The other authors declare that they have no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
2. Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. Circulation. 2021;143:e72-227.
3. Vahanian A, Beyersdorf F, Praz F, et al.; ESC/EACTS Scientific Document Group. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43:561-632.
4. Praz F, Borger MA, Lanz J, et al.; ESC/EACTS Scientific Document Group. 2025 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2025;46:4635-736.
5. Généreux P, Schwartz A, Oldemeyer JB, et al.; EARLY TAVR Trial Investigators. Transcatheter aortic-valve replacement for asymptomatic severe aortic stenosis. N Engl J Med. 2025;392:217-27.
6. Loganath K, Craig NJ, Everett RJ, et al.; EVOLVED investigators. Early intervention in patients with asymptomatic severe aortic stenosis and myocardial fibrosis: the EVOLVED randomized clinical trial. JAMA. 2025;333:213-21.
7. Kang DH, Park SJ, Lee SA, et al. Early surgery or conservative care for asymptomatic aortic stenosis. N Engl J Med. 2020;382:111-9.
8. Banovic M, Putnik S, Da Costa BR, et al. Aortic valve replacement vs. conservative treatment in asymptomatic severe aortic stenosis: long-term follow-up of the AVATAR trial. Eur Heart J. 2024;45:4526-35.
9. Jørgensen TH, Thyregod HGH, Savontaus M, et al.; NOTION-2 investigators. Transcatheter aortic valve implantation in low-risk tricuspid or bicuspid aortic stenosis: the NOTION-2 trial. Eur Heart J. 2024;45:3804-14.
10. Blankenberg S, Seiffert M, Vonthein R, et al.; DEDICATE-DZHK6 Trial Investigators. Transcatheter or surgical treatment of aortic-valve stenosis. N Engl J Med. 2024;390:1572-83.
11. Barbanti M, Costa G, Zappulla P, et al. Incidence of long-term structural valve dysfunction and bioprosthetic valve failure after transcatheter aortic valve replacement. J Am Heart Assoc. 2018;7:e008440.
12. Makkar RR, Thourani VH, Mack MJ, et al.; PARTNER 2 Investigators. Five-year outcomes of transcatheter or surgical aortic-valve replacement. N Engl J Med. 2020;382:799-809.
13. Sathananthan J, Lauck S, Polderman J, et al. Ten year follow-up of high-risk patients treated during the early experience with transcatheter aortic valve replacement. Catheter Cardiovasc Interv. 2021;97:E431-7.
14. Jørgensen TH, Thyregod HGH, Ihlemann N, et al. Eight-year outcomes for patients with aortic valve stenosis at low surgical risk randomized to transcatheter vs. surgical aortic valve replacement. Eur Heart J. 2021;42:2912-9.
15. Leon MB, Mack MJ, Pibarot P, et al.; PARTNER 3 Investigators. Transcatheter or surgical aortic-valve replacement in low-risk patients at 7 years. N Engl J Med. 2026;394:773-83.
16. Sá MP, Jacquemyn X, Van den Eynde J, et al. Midterm survival of low-risk patients treated with transcatheter versus surgical aortic valve replacement: meta-analysis of reconstructed time-to-event data. J Am Heart Assoc. 2023;12:e030012.
17. Krasniqi L, Brandes A, Mortensen PE, Gerke O, Riber L. Severe aortic stenosis treated with transcatheter aortic valve implantation or surgical aortic valve replacement with Perimount in Western Denmark 2016-2022: a nationwide retrospective study. Interdiscip Cardiovasc Thorac Surg. 2024;39:ivae122.
18. Biancari F, D’Errigo P, Barbanti M, et al. Ten-year outcomes after transcatheter or surgical aortic valve replacement in low-risk patients: the OBSERVANT study. Int J Cardiol Heart Vasc. 2024;55:101545.
19. Watanabe Y, Yamamoto M, Hioki H, et al.; OCEAN-TAVI Investigators. Long-term impact of mild paravalvular regurgitation after transcatheter aortic valve replacement: the OCEAN-TAVI registry. JACC Cardiovasc Interv. 2026;19:63-75.
20. Badertscher P, Stortecky S, Serban T, et al.; SwissTAVI Investigators. Long-term outcomes of patients requiring pacemaker implantation after transcatheter aortic valve replacement: the SwissTAVI registry. JACC Cardiovasc Interv. 2025;18:1163-71.
21. Jubran A, Patel RV, Sathananthan J, Wijeysundera HC. Lifetime management of patients with severe aortic stenosis in the era of transcatheter aortic valve replacement. Can J Cardiol. 2024;40:210-7.
22. Généreux P, Leon MB, Dar RD, et al. Predicting treatment of bioprosthetic aortic valve failure in the United States: a proposed model. Struct Heart. 2025;9:100339.
23. Bapat VN, Fukui M, Zaid S, et al. A guide to transcatheter aortic valve design and systematic planning for a redo-TAV (TAV-in-TAV) procedure. JACC Cardiovasc Interv. 2024;17:1631-51.
24. Testa L, Agnifili M, Van Mieghem NM, et al. Transcatheter aortic valve replacement for degenerated transcatheter aortic valves: the TRANSIT International Project. Circ Cardiovasc Interv. 2021;14:e010440.
25. Landes U, Webb JG, De Backer O, et al. Repeat transcatheter aortic valve replacement for transcatheter prosthesis dysfunction. J Am Coll Cardiol. 2020;75:1882-93.
26. Ochiai T, Oakley L, Sekhon N, et al. Risk of coronary obstruction due to sinus sequestration in redo transcatheter aortic valve replacement. JACC Cardiovasc Interv. 2020;13:2617-27.
27. Forrestal BJ, Case BC, Yerasi C, et al. Risk of coronary obstruction and feasibility of coronary access after repeat transcatheter aortic valve replacement with the self-expanding evolut valve: a computed tomography simulation study. Circ Cardiovasc Interv. 2020;13:e009496.
28. Lederman RJ, Babaliaros VC, Rogers T, et al. Preventing coronary obstruction during transcatheter aortic valve replacement: from computed tomography to BASILICA. JACC Cardiovasc Interv. 2019;12:1197-216.
29. Mercanti F, Rosseel L, Neylon A, et al. Chimney stenting for coronary occlusion during TAVR: insights from the chimney registry. JACC Cardiovasc Interv. 2020;13:751-61.
30. Mangieri A, Gallo F, Popolo Rubbio A, et al. Outcome of coronary ostial stenting to prevent coronary obstruction during transcatheter aortic valve replacement. Circ Cardiovasc Interv. 2020;13:e009017.
31. Khan JM, Greenbaum AB, Babaliaros VC, et al. The BASILICA trial: prospective multicenter investigation of intentional leaflet laceration to prevent TAVR coronary obstruction. JACC Cardiovasc Interv. 2019;12:1240-52.
32. Rogers T, Khan JM, Laham R, et al.; TELLTALE Investigators. Electrosurgical leaflet modification to prevent coronary obstruction during transcatheter aortic valve replacement in failing native and bioprosthetic valves. JACC Cardiovasc Interv. 2025;18:2355-68.
33. Dvir D, Tchétché D, Leon MB, et al. Leaflet modification before transcatheter aortic valve implantation in patients at risk for coronary obstruction: the ShortCut study. Eur Heart J. 2024;45:3031-41.
34. Wong CK, Eric Chan KY, Chan DT, et al. UNICORN for valve-in-valve transcatheter aortic valve replacement: UNICORN Hong Kong Registry. JACC Asia. 2026;6:52-63.
35. Chan KE, Tai-Leung Chan D, Lam CS, et al. First-in-human undermining iatrogenic coronary obstruction with radiofrequency needle (UNICORN) procedure during valve-in-valve transcatheter aortic valve replacement. Circ Cardiovasc Interv. 2022;15:928-31.
36. Haberman D, Lupu L, Merdler I, et al. UNICORN with a self-expanding valve to treat a degenerated balloon-expandable valve. JACC Cardiovasc Interv. 2025;18:123-5.
37. TreSquare Technologies. Available from: https://tresquaretech.com/. [Last accessed on 30 Jun 2026].
38. Kharbanda RK, Kennedy J, Jamal Z, et al.; BHF PROTECT-TAVI Investigators. Routine cerebral embolic protection during transcatheter aortic-valve implantation. N Engl J Med. 2025;392:2403-12.
39. Kapadia SR, Makkar R, Leon M, et al.; PROTECTED TAVR Investigators. Cerebral embolic protection during transcatheter aortic-valve replacement. N Engl J Med. 2022;387:1253-63.
40. Jagielak D, Targonński R, Ciećwierz D. First-in-human use of the next-generation ProtEmbo cerebral embolic protection system during transcatheter aortic valve-in-valve implantation. Interv Cardiol. 2021;16:1-4.
41. Preda A, Montalto C, Galasso M, et al. Fighting cardiac thromboembolism during transcatheter procedures: an update on the use of cerebral protection devices in Cath Labs and EP Labs. Life. 2023;13:1819.
42. Van Gils L, Kroon H, Daemen J, et al. Complete filter-based cerebral embolic protection with transcatheter aortic valve replacement. Catheter Cardiovasc Interv. 2018;91:790-7.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Special Topic
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].