


Robotic gastrectomy for gastric cancer: feasibility and outcomes of a newly established program
 0
0 Abstract
Aim: Robotic-assisted surgery has emerged as a minimally invasive alternative to open gastrectomy for gastric cancer, offering potential advantages in visualization, instrument precision, surgeon posture, and decreased length of stay (LOS). This study compares peri-operative and oncologic outcomes between robotic and open gastrectomy during an institutional transition to robotic-assisted gastric surgery.
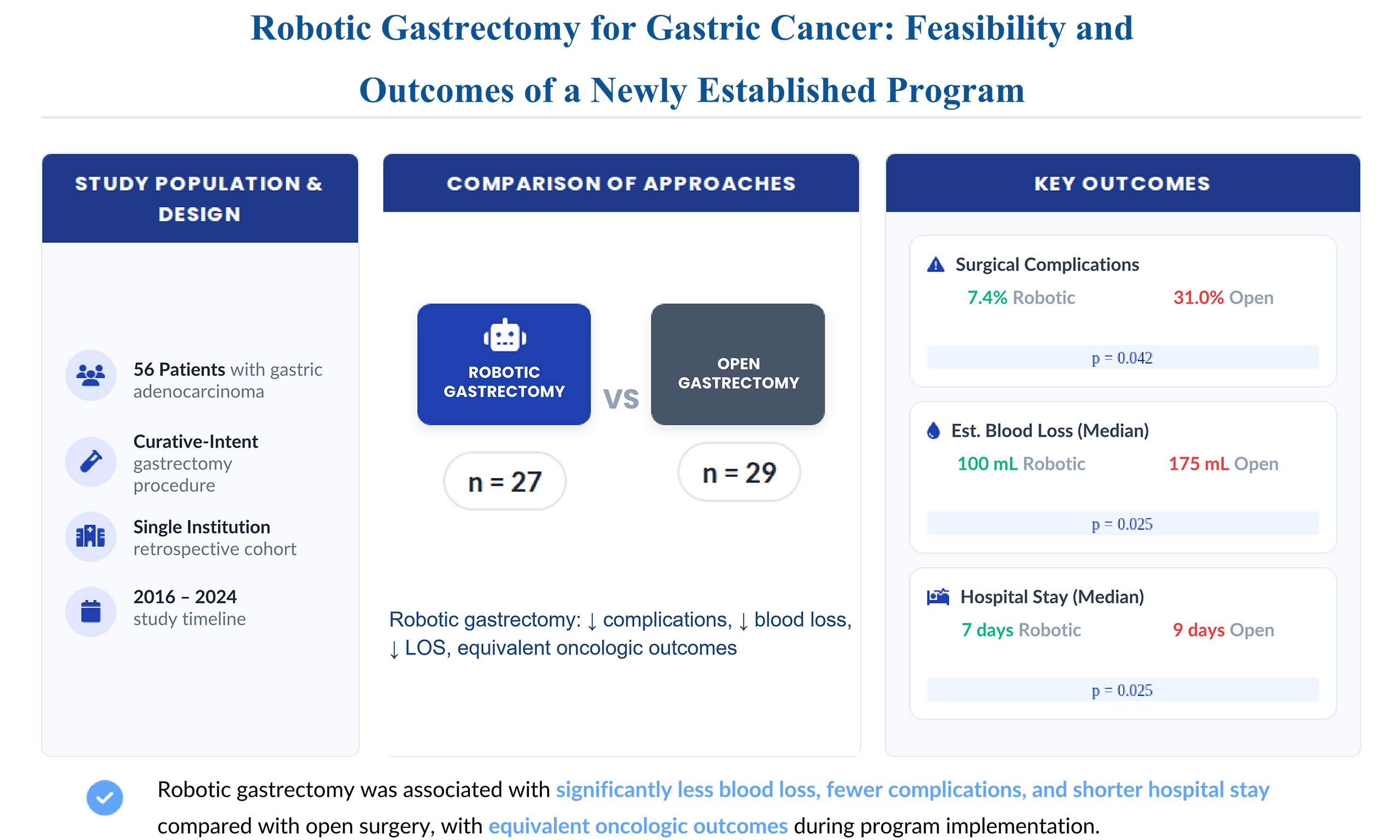
Methods: A retrospective cohort study was conducted of 56 patients who underwent curative-intent gastrectomy for gastric adenocarcinoma between February 2016 and December 2024. Twenty-seven patients underwent robotic-assisted gastrectomy and 29 underwent open surgery. Demographic, operative, pathologic, and postoperative outcomes were compared using Fisher’s exact and Wilcoxon rank-sum tests, with overall survival analyzed by Kaplan–Meier methods.
Results: Baseline characteristics were comparable between groups. Operative time was significantly longer for robotic surgery (median 320 vs. 255 minutes, P = 0.012), but estimated blood loss was lower (100 vs. 175 mL, P = 0.025). Operative complications were significantly fewer in the robotic group (7.4% vs. 31.0%, P = 0.042), and postoperative LOS was significantly shorter (7 vs. 9 days, P = 0.025). While lymph-node yield, R0 resection rate, and 5-year overall survival were numerically higher in the robotic group, these differences did not reach statistical significance.
Conclusion: Robotic gastrectomy demonstrated reduced blood loss, fewer complications, and shorter hospitalization compared with open surgery, with equivalent oncologic outcomes. These findings support the safety and feasibility of robotic gastrectomy during program implementation with significant benefits to the patients.
Keywords
INTRODUCTION
Gastric cancer is the fifth most diagnosed malignancy worldwide, with significant variation in incidence across geographic regions. Eastern Asia reports the highest rates of gastric cancer, whereas all regions of Africa have among the lowest. Despite a global decline in incidence - suspected to be linked to improved food preservation methods and decreasing prevalence of Helicobacter pylori infection - gastric cancer remains the fifth leading cause of cancer-related mortality globally[1].
The surgical management of gastric cancer, along with the technologies used to perform it, has evolved considerably over time. While ongoing clinical trials such as CRITICS, SENORITA, TOPGEAR, PILGRIM, and RENAISSANCE[2-6] continue to refine and optimize treatment strategies, the standard approach for T1b–T4 tumors remains partial or total gastrectomy with an adequate D2 lymph node dissection, or a minimum of 16 lymph nodes evaluated in the specimen as outlined in current NCCN guidelines[7]. Historically, this procedure was carried out via an open approach, and is inherently complex due to meticulous dissection, intestinal reconstruction, and thorough nodal evaluation.
In recent decades, the emergence of minimally invasive techniques has challenged the traditional open approach by offering potential benefits such as reduced postoperative pain, faster recovery, and shorter hospital stays. However, performing a gastrectomy laparoscopically significantly increases the technical demands of the procedure. These challenges hindered the widespread adoption of laparoscopic gastrectomy in many surgical centers[8].
The introduction of robotic-assisted surgery for gastric cancer in 2002 marked a pivotal advancement[9]. The robotic platform offers enhanced dexterity through multi-directional articulating instruments, improved instrument stability, tremor filtration, and superior three-dimensional camera visualization and 10× magnification. These features help overcome many of the limitations associated with conventional laparoscopy and have facilitated the more widespread use of minimally invasive techniques in complex gastric cancer surgery.
This study retrospectively evaluates the peri-operative and oncologic outcomes of robotic vs. open gastrectomy for gastric cancer, as performed by a single institution transitioning to robotic surgery without prior experience in complex laparoscopy.
METHODS
Study design and setting
This was a retrospective cohort study conducted at a tertiary teaching facility, evaluating clinical outcomes among patients who underwent surgical resection for gastric adenocarcinoma between February 2016 and December 2024, comparing robotic vs. open oncologic gastric resection. This study was approved by the Institutional Review Board (IRB) of PRISMA Health (Protocol ID: 2339137-2) and was authorized to use the relevant data. Given the retrospective nature of the study and the use of de-identified patient data, the requirement for written informed consent was waived.
Patient population
Adult patients (≥ 18 years) who underwent curative-intent gastrectomy for histologically confirmed gastric adenocarcinoma were included. Patients who underwent palliative procedures, had incomplete operative or follow-up data, or were younger than 18 years were excluded. Eligible cases were identified through the institutional surgical oncology database and verified through operative and pathology reports.
Data collection
Clinical data were extracted from the institutional Epic electronic health record and managed using a secure, HIPAA-compliant REDCap database. Data abstraction included demographic characteristics, comorbidities, operative details, pathologic outcomes, and 30-day postoperative events. All data were de-identified prior to analysis. Access to protected health information (e.g., medical record numbers, dates of service) was limited to ensure accurate patient linkage and temporal follow-up. No identifiable information was used in final analyses or dissemination.
Surgical technique
A total of four surgeons were included in the study with the surgical technique being dependent on the surgeon’s preference. Robotic procedures were performed using the da Vinci® Surgical System (Intuitive Surgical, Sunnyvale, CA), employing a standardized port configuration and lymphadenectomy. Reconstruction following distal or total gastrectomy was carried out using a Billroth II, Roux-en-Y gastro-jejunostomy, or esophago-jejunostomy, depending on resection extent. Open gastrectomies were performed via a midline laparotomy using conventional techniques for lymph node dissection and gastrointestinal reconstruction.
Outcome measures
The primary outcomes evaluated were lymph-node yield, postoperative complications (including anastomotic leak, return to the operating room, delayed bowel function, 30-day readmission, and 30-day mortality), estimated blood loss (EBL), and length of stay (LOS). Secondary outcomes included resection margin status, operative time, and overall survival.
Statistical analysis
Descriptive statistics were used to summarize patient demographics and peri-operative variables. Continuous data were expressed as medians with ranges and compared using the Wilcoxon rank-sum test. Categorical variables were compared using Fisher’s exact test. Kaplan–Meier survival analysis was carried out to estimate overall survival, with differences assessed using the log-rank test. Statistical significance was defined as P < 0.05. Statistical analysis was done with an intention to treat for both study groups.
RESULTS
Patient characteristics
A total of 56 patients met inclusion criteria between February 2016 and December 2024, comprising 27 robotic and 29 open gastrectomies. Baseline demographic and clinical characteristics were comparable between groups [Table 1]. The median age at surgery was 68 years (range, 27-91), and 60.7% of patients were male. Median body mass index (BMI) was similar across groups (26 vs. 24 kg/m2; P = 1.000). The prevalence of comorbidities - including hypertension (66.1%), coronary artery disease (19.6%), and chronic obstructive pulmonary disease (COPD) (14.3%) - did not differ significantly, although diabetes was more common in the open cohort (44.8% vs. 18.5%; P = 0.047), which may reflect differences in patient selection during the early phase of robotic program adoption. Prior intra-abdominal surgery was reported in 60.7% of all patients, with no significant difference between groups (P = 0.585). Cases were relatively evenly distributed throughout the study period.
Patient characteristics by surgical approach
| Characteristic | Total (N = 56) | Robotic (n = 27) | Open (n = 29) | P-value |
| Number of patients | 56 | 27 | 29 | - |
| Age at surgery, median [range] | 68 [27-91] | 69 [27-91] | 66 [43-87] | 0.948 |
| Sex, n (%) | 0.790 | |||
| Female | 22 (39.3) | 10 (37.0) | 12 (41.4) | |
| Male | 34 (60.7) | 17 (63.0) | 17 (58.6) | |
| Race/ethnicity, n (%) | 0.915 | |||
| White | 27 (48.2) | 12 (44.4) | 15 (51.7) | |
| Black | 20 (35.7) | 10 (37.0) | 10 (34.5) | |
| Hispanic | 5 (8.9) | 3 (11.1) | 2 (6.9) | |
| Asian | 4 (7.1) | 2 (7.4) | 2 (6.9) | |
| BMI (kg/m2), median [range] | 24 [16-40] | 26 [16-33] | 24 [17-40] | 1.000 |
| Nicotine use, n (%) | 0.420 | |||
| Current (within 30 days) | 11 (19.6) | 5 (18.5) | 6 (20.7) | |
| Former | 22 (39.3) | 13 (48.2) | 9 (31.0) | |
| Never | 23 (41.1) | 9 (33.3) | 14 (48.3) | |
| Comorbidities, n (%) | ||||
| Hypertension | 37 (66.1) | 18 (66.7) | 19 (65.5) | 1.000 |
| Diabetes | 18 (32.1) | 5 (18.5) | 13 (44.8) | 0.047* |
| COPD | 8 (14.3) | 4 (14.1) | 4 (13.8) | 1.000 |
| Chronic renal insufficiency | 2 (3.5) | 0 | 2 (6.9) | 0.492 |
| Liver insufficiency/failure | 1 (1.7) | 0 | 1 (3.5) | 1.000 |
| CHF | 3 (5.4) | 0 | 3 (10.3) | 0.264 |
| Coronary artery disease | 11 (19.6) | 5 (18.5) | 6 (20.7) | 1.000 |
| Cardiac arrhythmia | 11 (19.6) | 3 (11.1) | 8 (27.6) | 0.181 |
| IBD | 1 (1.8) | 0 | 1 (3.5) | 1.000 |
| PVD | 1 (1.8) | 0 | 1 (3.5) | 1.000 |
| Previous intra-abdominal surgery, n (%) | 0.585 | |||
| No | 22 (39.3) | 12 (44.4) | 10 (34.5) | |
| Yes | 34 (60.7) | 15 (55.6) | 19 (65.5) | |
| Previous surgery type, n | ||||
| Cholecystectomy | 14 | 5 | 9 | - |
| Colectomy | 4 | 0 | 4 | - |
| Appendectomy | 7 | 3 | 4 | - |
| Hysterectomy | 5 | 3 | 2 | - |
| Cesarean section | 2 | 1 | 1 | - |
| Esophagectomy | 1 | 0 | 1 | - |
| Ventral hernia repair | 1 | 0 | 1 | - |
| Inguinal hernia repair | 4 | 1 | 3 | - |
| Year of surgery, n (%) | 0.879 | |||
| 2016 | 8 (14.3) | 3 (11.1) | 5 (17.2) | |
| 2017 | 6 (10.7) | 4 (14.8) | 2 (6.9) | |
| 2018 | 4 (7.1) | 2 (7.4) | 2 (6.9) | |
| 2019 | 5 (8.9) | 1 (3.7) | 4 (13.8) | |
| 2020 | 8 (14.3) | 4 (14.8) | 4 (13.8) | |
| 2021 | 5 (8.9) | 2 (7.4) | 3 (10.3) | |
| 2022 | 7 (12.5) | 3 (11.1) | 4 (13.8) | |
| 2023 | 6 (10.7) | 4 (14.8) | 2 (6.9) | |
| 2024 | 7 (12.5) | 4 (14.8) | 3 (10.3) |
Operative characteristics
Operative details are summarized in Table 2. Neoadjuvant chemotherapy was administered in 57.1% of patients overall, with a higher, though not statistically significant, frequency in the robotic group (70.4% vs. 44.8%; P = 0.064). This difference may reflect patient selection or evolving multidisciplinary treatment patterns during early robotic program adoption rather than an effect of surgical approach. Similarly, neoadjuvant radiation was used in 17.9% of patients (25.9% vs. 10.3%; P = 0.171), which was also without statistical significance and potentially influenced by selection factors. Partial gastrectomy was the most common procedure (71.3%), with comparable distribution between robotic (77.8%) and open (65.5%) approaches (P = 0.382).
Operative details by surgical approach
| Characteristic | Total (N = 56) | Robotic (n = 27) | Open (n = 29) | P-value |
| Number of patients | 56 | 27 | 29 | - |
| Neoadjuvant chemotherapy, n (%) | 32 (57.1) | 19 (70.4) | 13 (44.8) | 0.064 |
| Neoadjuvant radiation, n (%) | 10 (17.9) | 7 (25.9) | 3 (10.3) | 0.171 |
| Gastrectomy type, n (%) | 0.382 | |||
| Partial | 40 (71.3) | 21 (77.8) | 19 (65.5) | |
| Total | 16 (28.6) | 6 (22.2) | 10 (34.5) | |
| Conversion to open approach | - | 3 (11.1) | - | |
| Operative complication (excluding conversion), n (%) | 0.042* | |||
| No | 45 (80.4) | 25 (92.6) | 20 (69.0) | |
| Yes | 11 (19.6) | 2 (7.4) | 9 (31.0) | |
| Specific complications | ||||
| Bleeding | 1 | 1 | 0 | |
| Injury to adjacent organs | 6 | 0 | 6 | |
| Anastomotic leak | 2 | 0 | 2 | |
| Pancreatic injury/fistula | 1 | 0 | 1 | |
| Inadequate margins | 1 | 1 | 0 | |
| Operative time (min) | 285 [140-615] | 320 [190-615] | 255 [140-568] | 0.012* |
| Anesthesia time (min) | 296 [162-615] | 334 [210-615] | 265 [162-552] | 0.011* |
| ASA class, n (%) | 0.620 | |||
| 2 | 4 (7.1) | 3 (11.1) | 1 (3.5) | |
| 3 | 45 (80.4) | 21 (77.8) | 24 (82.8) | |
| 4 | 7 (12.5) | 3 (11.1) | 4 (13.8) | |
| EBL (mL) | 125 [15-900] | 100 [20-650] | 175 [15-900] | 0.025* |
| Margin status, n (%) | 1.000 | |||
| R0 | 53 (94.6) | 26 (96.3) | 27 (93.1) | |
| R1 | 2 (3.6) | 1 (3.7) | 1 (3.5) | |
| R2 | 1 (1.8) | 0 | 1 (3.5) | |
| Final tumor stage, n (%) | 0.683 | |||
| 0 | 3 (5.4) | 3 (11.1) | 0 | |
| IA | 7 (12.5) | 3 (11.1) | 4 (13.8) | |
| IB | 9 (16.1) | 5 (18.5) | 4 (13.8) | |
| IIA | 5 (8.9) | 2 (7.4) | 3 (10.3) | |
| IIB | 10 (17.9) | 5 (18.5) | 5 (17.2) | |
| IIIA | 5 (8.9) | 3 (11.1) | 2 (6.9) | |
| IIIB | 8 (14.3) | 4 (14.8) | 4 (13.8) | |
| IIIC | 4 (7.1) | 1 (3.7) | 3 (10.3) | |
| IV | 5 (8.9) | 1 (3.7) | 4 (13.8) | |
| Lymph node yield | 19 [7-52] | 19 [7-50] | 20 [8-52] | 0.328 |
Median operative time was significantly longer for robotic surgery (320 min [190-615]) compared with open gastrectomy (255 min [140-568]; P = 0.012). Median anesthesia time followed a similar pattern (334 vs.
Three robotic cases (11.1%) required conversion to open surgery. These cases and outcomes were included in the robotic cohort with an intention to treat analysis. The first was due to dense adhesions from prior open cholecystectomy and inguinal hernia repair; the second was related to intra-operative bleeding and poor visualization despite no prior abdominal surgery; and the third involved extensive fibrosis and poor visualization in a patient with a prior jejunostomy tube placement.
Pathologic and oncologic outcomes
R0 resection was achieved in 94.6% of all cases, with no significant difference between robotic and open groups (96.3% vs. 93.1%; P = 1.000). Median lymph-node yield was similar between robotic and open approaches (19 [7-50] vs. 20 [8-52]; P = 0.328). Final tumor stage distribution did not differ significantly between groups (P = 0.683).
At a median follow-up of 32 months (range, 0-105 months), Kaplan–Meier analysis demonstrated no statistically significant difference in estimated 5-year overall survival between robotic and open gastrectomy [66.1% (95% confidence interval, CI; 40.7-91.5) vs. 52.3% (95%CI, 32.1-72.5); P = 0.166].
Postoperative outcomes
Postoperative results are summarized in Table 3. The median LOS was significantly shorter following robotic surgery (7 days [4-21]) compared with open surgery (9 days [5-38]; P = 0.025). Operative complications occurred less frequently in the robotic group (7.4% vs. 31.0%; P = 0.002), with no significant differences in reoperation (11.1% vs. 24.1%; P = 0.299), 30-day readmission (7.4% vs. 25.9%; P = 0.142), or intensive care unit (ICU) admission rates (22.2% vs. 37.9%; P = 0.252). Thirty-day mortality occurred in two open cases; none were observed among robotic patients.
Outcomes at 30 days by surgical approach
| Outcome | Total (N = 56) | Robotic (n = 27) | Open (n = 29) | P-value |
| Number of patients | 56 | 27 | 29 | - |
| Surgical LOS (days) | 7 [4-38] | 7 [4-21] | 9 [5-38] | 0.025* |
| ICU admission, n (%) | 17 (30.4) | 6 (22.2) | 11 (37.9) | 0.252 |
| Discharge status, n (%) | 0.492 | |||
| Alive | 54 (96.4) | 27 (100) | 27 (93.1) | |
| Deceased | 2 (3.6) | 0 | 2 (6.9) | |
| Reoperation | 10 (17.9) | 3 (11.1) | 7 (24.1) | 0.299 |
| Readmission | 9 (16.7) | 2 (7.4) | 7 (25.9) | 0.142 |
| Follow-up (months) | 32 [0-105] | 35 [3-97] | 26 [0-105] | 0.317 |
| Kaplan–Meier estimated survival at 5 years | 59.8 | 66.1 | 52.3 | 0.166 |
| 95%CI | (44.1, 75.5) | (40.7, 91.5) | (32.1, 72.5) | |
| Deaths at 5 years (n) | 20 | 7 | 13 |
Two perioperative deaths (3.6%) occurred, both in the open group (P = 0.492) with both patients transitioning to comfort care after a prolonged and difficult hospital course. Median follow-up duration was 32 months (range 0-105), with no difference between groups (P = 0.317). Kaplan–Meier analysis demonstrated a 5-year estimated overall survival of 59.8% (95%CI, 44.1-75.5) for the total cohort, with a higher, though not statistically significant, survival rate in the robotic group (66.1% vs. 52.3%, P = 0.166).
DISCUSSION
In this single-center retrospective analysis comparing robotic and open gastrectomy for gastric adenocarcinoma, 56 cases were reviewed to assess differences between minimally invasive and traditional surgical approaches. Accordingly, this study is best interpreted as an evaluation of early program implementation rather than a definitive comparative effectiveness analysis. Although speculative, the open cohort may have represented a higher-risk subset, as early implementation of a robotic program often favors patient selection with fewer comorbidities, risk factors, or prior abdominal operations to minimize conversion risk and support a safer learning curve. Nonetheless, baseline demographic and clinical characteristics were largely comparable between groups, with the exception of diabetes, which was more prevalent in the open cohort (44.8% vs. 18.5%, P = 0.047). Additionally, a greater proportion of patients in the robotic group received neoadjuvant chemotherapy (70.4% vs. 44.8%, P = 0.064) and neoadjuvant radiation (25.9% vs. 10.3%, P = 0.171), though these differences did not reach statistical significance. No additional differences were observed in comorbidities, prior intra-abdominal surgery, or type of gastrectomy performed.
Three robotic cases (11.1%) required conversion to an open procedure. One conversion was necessitated by dense adhesions in a patient with prior open cholecystectomy and inguinal hernia repair. The second occurred due to intra-operative bleeding and limited visualization despite no prior abdominal surgery. The third involved extensive fibrosis and poor visualization in a patient with a history of jejunostomy tube placement. These cases underscore the technical challenges inherent to the early adoption of robotic gastrectomy, particularly in patients with complex surgical histories or altered anatomy. The observed conversion rate in this series (11.1%) was slightly higher than national averages reported in larger cohorts, which range from 3.8% to 7.8%[10,11]. Prior studies have identified factors such as large tumor size, total gastrectomy, and bulky nodal disease or adjacent organ invasion as predictors of conversion[10,11]. Notably, other institutional experiences have demonstrated that the standardization of operative techniques and accumulation of surgeon experience can substantially reduce conversion rates, from 46.0% to 15.8%[12], underscoring the impact of structured program development on procedural success.
In the present study, several peri-operative outcomes were observed to favor the robotic approach over open gastrectomy, including reduced EBL, fewer operative complications, and shorter postoperative hospital stay. EBL was significantly lower in the robotic cohort compared with the open group (100 vs. 175 mL, P = 0.025). Although our findings did not replicate the extremely low blood loss reported in some series (as low as
Interestingly, the observed reduction in operative complications in the robotic group was not driven by wound-related morbidity but rather by differences in specific intraoperative and technical complications. In our cohort, injuries to adjacent organs accounted for the majority of complications and occurred exclusively in the open group, suggesting a potential advantage of the robotic platform in facilitating precise dissection and improved visualization in confined operative planes. Similarly, anastomotic leaks were observed only in the open cohort, although the absolute number of events was small.
These findings differ somewhat from prior large database studies, which have primarily demonstrated reductions in systemic and postoperative complications - such as surgical site infections, pulmonary complications, and transfusion requirements - rather than intraoperative injuries[18]. In the pooled analysis by Solaini et al., overall complication rates for robotic gastrectomy were comparable to those observed in our study, with low reported rates of anastomotic leak (~2%-3%) and no clear difference between approaches[10]. Likewise, Garsot et al. found similar rates of anastomotic and major complications between open and minimally invasive approaches[19].
The predominance of adjacent organ injuries and anastomotic complications in the open cohort of our study may reflect technical factors, including exposure and visualization, but may also be influenced by case selection and the learning curve associated with early adoption of a robotic program. Therefore, while our findings suggest that robotic gastrectomy may reduce certain intraoperative technical complications, these results should be interpreted with caution and validated in larger cohorts.
Additionally, robotic gastrectomy was associated with a much shorter postoperative hospital stay (7 [4-21] vs. 9 [5-38] days, P = 0.025). The IMIGASTRIC registry demonstrated a median hospital stay of 8 days for robotic cases compared to 11 days for open surgery (P < 0.0001)[16], while the recent network meta-analysis by Manara et al. (2024) similarly found that robotic total gastrectomy was associated with faster postoperative recovery relative to open procedures[17]. Nakauchi et al. (2021), in a multi-center U.S. analysis, also reported that minimally invasive approaches - including robotic - were associated with reduced perioperative morbidity and shorter hospitalization without compromising oncologic outcomes[15]. These consistent findings likely stem from the reduced surgical trauma inherent to minimally invasive techniques, which utilize smaller incisions, magnified three-dimensional visualization, and enhanced instrument dexterity to minimize tissue disruption and accelerate recovery.
In contrast, the open approach had shorter operative time when compared to its robotic counterpart (median 255 vs. 320 min, P = 0.012). This finding aligns with the randomized controlled trial by Ribeiro
When evaluating lymphadenectomy, the open and robotic group demonstrated very similar results (20 [8-52] vs. 19 [7-50], P = 0.328). Our results do contrast with recent multi-center analyses demonstrating equivalent or superior lymph-node retrieval with robotic gastrectomy. Trastulli et al. (2023) reported comparable nodal yields and lower postoperative morbidity in the robotic group (16.2% vs. 24.1%, P =
Emerging strategies such as sentinel lymph-node (SLN) navigation surgery may further refine the balance between oncologic adequacy and surgical invasiveness. The SENORITA randomized trial reported no significant difference in 5-year disease-free, overall, or disease-specific survival between standard laparoscopic gastrectomy and SLN navigation surgery[22], suggesting that tailored nodal dissection strategies may play an increasing role in early-stage disease.
When comparing long-term outcomes, the 5-year estimated overall survival for the entire cohort was 59.8% (95%CI, 44.1-75.5), with a higher, though not statistically significant, rate observed in the robotic group compared with the open group (66.1% vs. 52.3%, P = 0.166). These findings are reassuring and consistent with previously published series reporting 5-year survival rates of approximately 50%-65%, with robotic gastrectomy demonstrating comparable or, in some cases, superior outcomes relative to the open approach[10,19]. However, our study is underpowered to detect differences in long-term survival.
Overall, our findings underscore that the transition from open to robotic gastrectomy involves a distinct and measurable learning curve. Importantly, these results demonstrate that robotic gastrectomy can be implemented safely, with perioperative and oncologic outcomes comparable to the open approach. Although minimally invasive techniques may offer advantages in postoperative recovery, achieving consistent oncologic equivalence - particularly in lymph-node harvest - depends on accumulated surgical experience, procedural standardization, and institutional support. While some outcomes were favorable in the robotic cohort, these findings are best interpreted as supporting feasibility and safety rather than establishing superiority. The evolution of robotic prostatectomy provides an instructive parallel: while early laparoscopic prostatectomy offered clinical benefits, its technical complexity limited widespread adoption until the introduction of robot-assisted platforms, which reduced operative times and improved oncologic outcomes as experience accrued[23].
Drawing from this precedent, the gastric cancer surgical community can benefit from implementing structured, competency-based training models to accelerate safe and effective adoption of robotic techniques. A modular curriculum incorporating simulation, mentorship, and proctoring could help mitigate early technical challenges and shorten the learning curve. Adapting evidence-based frameworks from urologic robotic surgery education - such as multimodal simulation, stepwise supervised progression, and video-based performance review - may further promote earlier attainment of proficiency while maintaining patient safety[24].
Limitations
This study has several limitations. Its retrospective, single-institution design introduces potential selection and information biases, as the choice of surgical approach was influenced by surgeon preference and institutional experience. In particular, the early adoption phase of the robotic program may have led to preferential selection of lower-risk patients, which could confound comparisons between groups. The modest sample size (n = 56) limits statistical power and may obscure smaller differences in outcomes. Additionally, the robotic cohort reflects an early learning phase, during which surgical performance and perioperative outcomes may improve with increasing experience.
The extended study period (2016-2024) represents another important limitation, as substantial evolution in surgical technique, perioperative management, anesthesia protocols, and institutional experience likely occurred over time. As a result, improvements in outcomes such as blood loss, complication rates, and LOS may partially reflect temporal advancements in care rather than the effect of the robotic platform alone. Therefore, the independent contribution of surgical approach to these outcomes cannot be definitively determined.
In addition, this study reflects outcomes during the early implementation phase of a robotic gastrectomy program, during which a learning curve is expected. Surgical performance, operative efficiency, and perioperative outcomes are known to improve with increasing surgeon and team experience. As this analysis did not account for case sequencing or adjust for the learning curve, improvements observed over time may be influenced by increasing familiarity with the robotic platform rather than the platform itself. Consequently, the isolated effect of robotic technology on outcomes cannot be fully distinguished from the impact of cumulative experience.
Survival analysis was limited by follow-up duration, and outcomes should be interpreted cautiously, as the study is underpowered to detect differences in long-term oncologic endpoints. Finally, cost comparisons were not performed.
Despite these limitations, this study provides meaningful real-world insight into the feasibility, safety, and perioperative advantages of robotic gastrectomy during program implementation and contributes to understanding the learning curve associated with transitioning from open to minimally invasive gastric cancer surgery.
Conclusion
In our transition to robotic gastric cancer surgery, robotic gastrectomy was associated with lower EBL, shorter LOS, and fewer complications, while maintaining comparable oncologic outcomes to open surgery. These findings support the feasibility and safety of robotic gastrectomy during program implementation. While certain perioperative outcomes were favorable, definitive conclusions regarding superiority over the open approach cannot be drawn from this study.
DECLARATIONS
Authors’ contributions
Made substantial contributions to conception and design of the study and performed data analysis and interpretation: Rodriguez N, Sweatt B, Trocha S
Performed data acquisition and provided administrative, technical, and material support: Rodriguez N, Sweatt B, Trocha S
Availability of data and materials
All data are available from the corresponding author upon reasonable request. This will have to be approved by the data committee prior to distribution.
AI and AI-assisted tools statement
During the preparation of this manuscript, the AI tool ChatGPT (version GPT-5, released October 2025) was used solely for language editing. During the preparation of this manuscript, the AI tool Google Gemini (version 3.1, released February 2026) was used solely for the creation of the graphical abstract. The tool did not influence the study design, data collection, analysis, interpretation, or the scientific content of the work. All authors take full responsibility for the accuracy, integrity, and final content of the manuscript.
Financial support and sponsorship
None.
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
This study was conducted in accordance with and was approved by the Institutional Review Board (IRB) of PRISMA Health (Protocol ID: 2339137-2). Given the retrospective nature of this study and the use of de-identified patient data, the requirement for written informed consent was formally waived by the IRB. All data were handled in compliance with HIPAA regulations to ensure patient confidentiality.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74:229-63.
2. Leong T, Smithers BM, Haustermans K, et al. TOPGEAR: a randomized, phase III trial of perioperative ECF chemotherapy with or without preoperative chemoradiation for resectable gastric cancer: interim results from an international, intergroup trial of the AGITG, TROG, EORTC and CCTG. Ann Surg Oncol. 2017;24:2252-8.
3. Cats A, Jansen EPM, van Grieken NCT, et al.; CRITICS investigators. Chemotherapy versus chemoradiotherapy after surgery and preoperative chemotherapy for resectable gastric cancer (CRITICS): an international, open-label, randomised phase 3 trial. Lancet Oncol. 2018;19:616-28.
4. Cui S, Liang H, Li Y, et al.; Chinese Peritoneal Oncology Study Group. PILGRIM: phase III clinical trial in evaluating the role of hyperthermic intraperitoneal chemotherapy for locally advanced gastric cancer patients after radical gastrectomy with D2 lymphadenectomy (HIPEC-01). J Clin Oncol. 2020;38:4538.
5. Kim YW, Min JS, Yoon HM, et al. Laparoscopic sentinel node navigation surgery for stomach preservation in patients with early gastric cancer: a randomized clinical trial. J Clin Oncol. 2022;40:2342-51.
6. Al-Batran S, Lorenzen S, Riera J, et al. Effect of chemotherapy/targeted therapy alone vs. chemotherapy/targeted therapy followed by radical surgical resection on survival and quality of life in patients with limited-metastatic adenocarcinoma of the stomach or esophagogastric junction: the IKF-575/RENAISSANCE phase III trial. J Clin Oncol. 2024;42:LBA4001.
7. NCCN. Gastric Cancer. 2025 Available from: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1434. [Last accessed on 27 May 2026].
8. Waller GC, Khan TM, Correa-Gallego C. Minimally invasive gastrectomy. Surg Clin North Am. 2025;105:15-30.
9. Hashizume M, Shimada M, Tomikawa M, et al. Early experiences of endoscopic procedures in general surgery assisted by a computer-enhanced surgical system. Surg Endosc. 2002;16:1187-91.
10. Solaini L, Avanzolini A, Pacilio CA, Cucchetti A, Cavaliere D, Ercolani G. Robotic surgery for gastric cancer in the west: a systematic review and meta-analyses of short-and long-term outcomes. Int J Surg. 2020;83:170-5.
11. Perez Holguin RA, Stahl KA, Hendriksen BS, et al. Predictors of conversion during minimally invasive gastrectomy for malignancy. J Surg Res. 2022;279:275-84.
12. Chen C, Lim T, Yang A, et al. Risk of open conversion during robotic gastrectomy for gastric cancer: optimizing patient selection. J Surg Oncol. 2025;132:503-13.
13. Ojima T, Nakamura M, Hayata K, et al. Short-term outcomes of robotic gastrectomy vs laparoscopic gastrectomy for patients with gastric cancer: a randomized clinical trial. JAMA Surg. 2021;156:954-63.
14. Ribeiro U Jr, Dias AR, Ramos MFKP, et al. Short-term surgical outcomes of robotic gastrectomy compared to open gastrectomy for patients with gastric cancer: a randomized trial. J Gastrointest Surg. 2022;26:2477-85.
15. Nakauchi M, Vos E, Janjigian YY, et al. Comparison of long- and short-term outcomes in 845 open and minimally invasive gastrectomies for gastric cancer in the United States. Ann Surg Oncol. 2021;28:3532-44.
16. Trastulli S, Desiderio J, Lin JX, et al. Open vs robotic gastrectomy with D2 lymphadenectomy: a propensity score-matched analysis on 1469 patients from the IMIGASTRIC prospective database. Langenbecks Arch Surg. 2023;408:302.
17. Manara M, Aiolfi A, Bonitta G, et al. Short-term outcomes analysis comparing open, lap-assisted, totally laparoscopic, and robotic total gastrectomy for gastric cancer: a network meta-analysis. Cancers. 2024;16:3404.
18. Bates KR, Jones W, Liggett MR, Zaza NN, Vitello DJ, Bentrem DJ. Complications following open versus minimally invasive resection of gastric adenocarcinoma. J Surg Oncol. 2025;131:1302-12.
19. Garsot E, Sentí S, Salvador H, et al.; the Spanish EURECCA Esophagogastric Cancer Group. Outcomes of minimally invasive versus open gastrectomy for gastric cancer surgery with curative intent: a population-based cohort study. Ann Surg. 2025;282:800-9.
20. Liao G, Chen J, Ren C, et al. Robotic versus open gastrectomy for gastric cancer: a meta-analysis. PLoS One. 2013;8:e81946.
21. Hirata Y, Chiang YJ, Mansfield P, Badgwell BD, Ikoma N. Trends of oncological quality of robotic gastrectomy for gastric cancer in the United States. World J Oncol. 2023;14:371-81.
22. Hur H, Lee YJ, Kim YW, et al. Clinical efficacy of laparoscopic sentinel node navigation surgery for stomach preservation in patients with early gastric cancer: 5-year results of the SENORITA trial. Ann Surg. 2025;281:296-303.
23. Tobias-Machado M, Mitre AI, Rubinstein M, Costa EF, Hidaka AK. Robotic-assisted radical prostatectomy learning curve for experienced laparoscopic surgeons: does it really exist? Int Braz J Urol. 2016;42:83-9.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].