


Epidemiological trends in the burden of atrial fibrillation and atrial flutter in China (1990-2023)
 0
0 Abstract
Aim: Atrial fibrillation and atrial flutter (AF/AFL) represent a growing public health challenge in China amid rapid population aging. This study aimed to comprehensively assess long-term trends, sex- and age-specific patterns, driving factors, and future projections of AF/AFL burden in China from 1990 to 2023.
Methods: Data were obtained from Global Burden of Disease 2023. Temporal trends, driving factors, and future projections were evaluated using joinpoint regression, age-period-cohort models, decomposition analysis, frontier analysis, and autoregressive integrated moving average (ARIMA) models.
Results: From 1990 to 2023, the absolute numbers of AF/AFL cases, deaths, and disability-adjusted life years (DALYs) increased substantially in China, whereas age-standardized mortality and DALY rates declined overall, with a recent upturn after 2020. Incidence and prevalence were generally higher in males, whereas females had higher mortality and DALYs at older ages. Population aging was the dominant contributor to increases in incidence, prevalence, mortality, and DALYs. Age-period-cohort models analyses showed that among individuals born after 1944, the burden of AF/AFL was higher in males than in females. Frontier analysis indicated that China still lags behind several high Socio-demographic Index regions in AF/AFL burden control. ARIMA projections suggested declining mortality and DALYs but heterogeneous future trends in incidence and prevalence by sex.
Conclusions: Despite improvements in age-standardized mortality and DALYs, the overall burden of AF/AFL in China continues to increase, primarily driven by population aging. Targeted prevention, early detection, and optimized management strategies - particularly among older adults and high-risk males - are urgently needed.
Keywords
INTRODUCTION
Atrial fibrillation and flutter (AF/AFL) are common atrial arrhythmias and represent a substantial public health burden owing to their associated morbidity and mortality. AF is characterized by an irregular and often rapid heart rate, whereas AFL typically exhibits a more organized but still abnormal rhythm. Despite these electrophysiological differences, both conditions are classified as atrial tachyarrhythmias and are frequently associated with similar cardiovascular complications. AF and AFL often coexist, thereby increasing the risk of adverse outcomes, particularly ischemic stroke and heart failure[1]. Both arrhythmias are independently associated with an approximately fivefold increased risk of stroke compared with sinus rhythm, with AF contributing to nearly 20% of all ischemic strokes[2,3]. This risk is further heightened when coexisting conditions, including hypertension, heart failure, and ischemic heart disease, are present[4]. Notably, AF is a major cause of ischemic stroke, especially among older adults, and even subclinical AF may increase the risk of future stroke events[5]. Early detection through screening, particularly in high-risk and elderly populations, offers an opportunity to prevent cardioembolic strokes and their associated cognitive sequelae[6]. Anticoagulant therapy may confer additional benefits by reducing subclinical cerebrovascular injury and lowering the subsequent risk of dementia, thereby potentially preserving cognitive function in patients with AF[7]. Moreover, AF and AFL are important contributors to the development of heart failure, as rapid and irregular ventricular rates can impair cardiac output and accelerate disease progression[8].
In China, AF/AFL has emerged as a major and growing public health burden, largely driven by rapid population aging and the increasing prevalence of cardiovascular risk factors. Estimates from the Global Burden of Disease Study 2021 indicate that more than 10 million individuals are affected by AF/AFL in China. Substantial numbers of incident cases and deaths, along with over 1.6 million disability-adjusted life years, are attributable to these arrhythmias, all of which have increased since 1990[8]. Population-based surveys further reveal a considerable burden of undiagnosed disease, with an AF prevalence of approximately 0.7% among Chinese adults aged 35 years or older and marked age-related increases accompanied by significant impairment in quality of life[9]. Moreover, substantial variation in AF/AFL burden has been observed across sex and age groups, with rising incidence rates in younger populations, divergent mortality trends between males and females, and projections suggesting a marked escalation in both incidence and mortality in the coming decades, particularly among women[10].
Despite increasing attention to the burden of AF/AFL in China, important knowledge gaps remain. In particular, integrated analyses that simultaneously examine incidence, prevalence, mortality, and disability-adjusted life years (DALYs), while accounting for temporal trends, age-period-cohort effects, and future projections, are still lacking. To address these gaps, the present study utilizes the most recent data from the Global Burden of Disease Study 2023 and applies multiple analytical approaches, including joinpoint regression, age-period-cohort modeling, decomposition analysis, frontier analysis, and autoregressive integrated moving average (ARIMA) models. By systematically evaluating AF/AFL burden from incidence, prevalence, mortality, and DALYs, this study offers a more comprehensive and up-to-date understanding of patterns, drivers, and future trajectories in China.
MATERIALS AND METHODS
Data sources
The Global Burden of Disease (GBD) database is a major international resource for health data, providing comprehensive data on a wide range of diseases, injuries, and risk factors that affect global health (https://vizhub.healthdata.org/gbd-results). The GBD study is conducted by the Institute for Health Metrics and Evaluation (IHME) at the University of Washington and systematically quantifies health loss across different populations and regions worldwide. This dataset tracks temporal trends in health outcomes and disease burden, offering valuable insights for policymakers, researchers, and healthcare providers[11,12].
In the present study, data on AF/AFL in China (excluding Taiwan) from 1990 to 2023 were extracted from the GBD database. AF/AFL cases in the GBD study were identified based on standard clinical diagnostic criteria, primarily relying on electrocardiographic evidence[13]. The analyses encompassed four key measures: incidence, prevalence, mortality, and DALYs. Sex-specific analyses were conducted, and the study population included individuals aged ≥ 30 years. As the GBD database contains aggregated data without individual-level identifiers, ethical approval was not required for this study.
Statistical analysis
Joinpoint regression analysis was applied to identify temporal trends and potential changes in trends over time. This method employs segmented linear regression models to divide the time series into multiple contiguous intervals, allowing distinct linear trends to be estimated for different time periods[14]. In this study, joinpoint analyses were conducted using the Joinpoint Regression Program (version 5.1.0). The analysis was performed on a logarithmic scale. Standard errors were calculated based on 95% uncertainty intervals (UI). Model selection was performed using the permutation test approach, with an overall significance level set at 0.05. A total of 4,499 permutations were used, and the model permitted up to six joinpoints.
The age-period-cohort model is a widely used statistical framework to analyze and interpret demographic data, particularly in epidemiology, sociology, and public health research. It facilitates the separation and evaluation of the distinct contributions attributable to age, temporal period, and birth cohort with respect to specific health outcomes or behavioral patterns. In the present study, a web-based analytical platform was utilized to examine how these three dimensions influence the aforementioned measures of disease burden; further methodological details are available at: https://analysistools.cancer.gov/apc[15]. The analysis incorporated data collected over three decades (1994-2023), with the overall timeframe segmented into successive five-year intervals to support age-period-cohort modeling.
Decomposition analysis is an important statistical approach for identifying the underlying drivers of changes in specific outcomes over time. This method has been widely applied in demographic studies, econometrics, and public health research, as it enables the attribution of changes in aggregate indicators, such as mortality rates, disease incidence, or economic ratios- to distinct contributing factors. In this study, we applied the Das Gupta method to decompose changes in the burden of AF/AFL over the past 34 years into three components: population aging, population growth, and epidemiological change. This approach allowed us to quantify the relative contributions of demographic structure and disease risk to the observed temporal trends in AF/AFL burden.
A nonparametric data envelopment analysis (DEA) framework was applied to conduct frontier analysis. To assess the robustness and stability of the estimated frontier, a resampling procedure was implemented. The original dataset was resampled with replacement for 100 iterations. In each iteration, a bootstrap sample of the same size as the original dataset was generated through random sampling with replacement[16]. In this analysis, the Socio-demographic Index (SDI) was defined as the input variable and DALYs as the output variable. The frontier was then estimated to represent the minimum achievable DALYs at different levels of SDI. Finally, locally weighted regression (LOESS) was used for data visualization to illustrate temporal trends and relative performance. This approach was applied to depict changes in DALYs attributable to AF/AFL in China from 1990 to 2023, in comparison with 204 countries.
The ARIMA model was employed as a time-series forecasting approach to project future disease burden trends. The ARIMA framework consists of three components: the autoregressive (AR), the differencing (I), and the moving average (MA). Annual data were used, with 1990 defined as the starting year and each calendar year treated as a single observation. If the time series was non-stationary, first-order differencing was applied to achieve stationarity. Model parameters - including the autoregressive order (p), degree of differencing (d), and moving average order (q) - were automatically selected using the auto.arima function based on optimal model fit criteria. Finally, the Ljung-Box test was performed to ensure model adequacy by verifying that the residuals were white noise [Supplementary Table 1]. The finalized ARIMA model was then applied to forecast disease burden indicators for the 15-year period following 2023 to estimate future trends in atrial fibrillation and flutter - related burden.
Statistical analyses were performed in R (version 4.3.2), with statistical significance defined as P value < 0.05.
RESULTS
Burden of AF/AFL in China
From 1990 to 2023, the numbers of incident cases, prevalent cases, deaths, and DALYs attributable to AF/AFL in China exhibited an overall increasing trend in both males and females. In contrast, the age-standardized incidence rate (ASIR) and age-standardized prevalence rate (ASPR) demonstrated a non-linear temporal pattern, characterized by an initial decline followed by a subsequent increase. Notably, the upward trend was most pronounced during the period from 2005 to 2010 [Figure 1A-D]. Overall, these findings indicate that although the absolute burden of AF/AFL increased substantially, the age-standardized rates followed a non-linear pattern with a marked rise during 2005-2010.
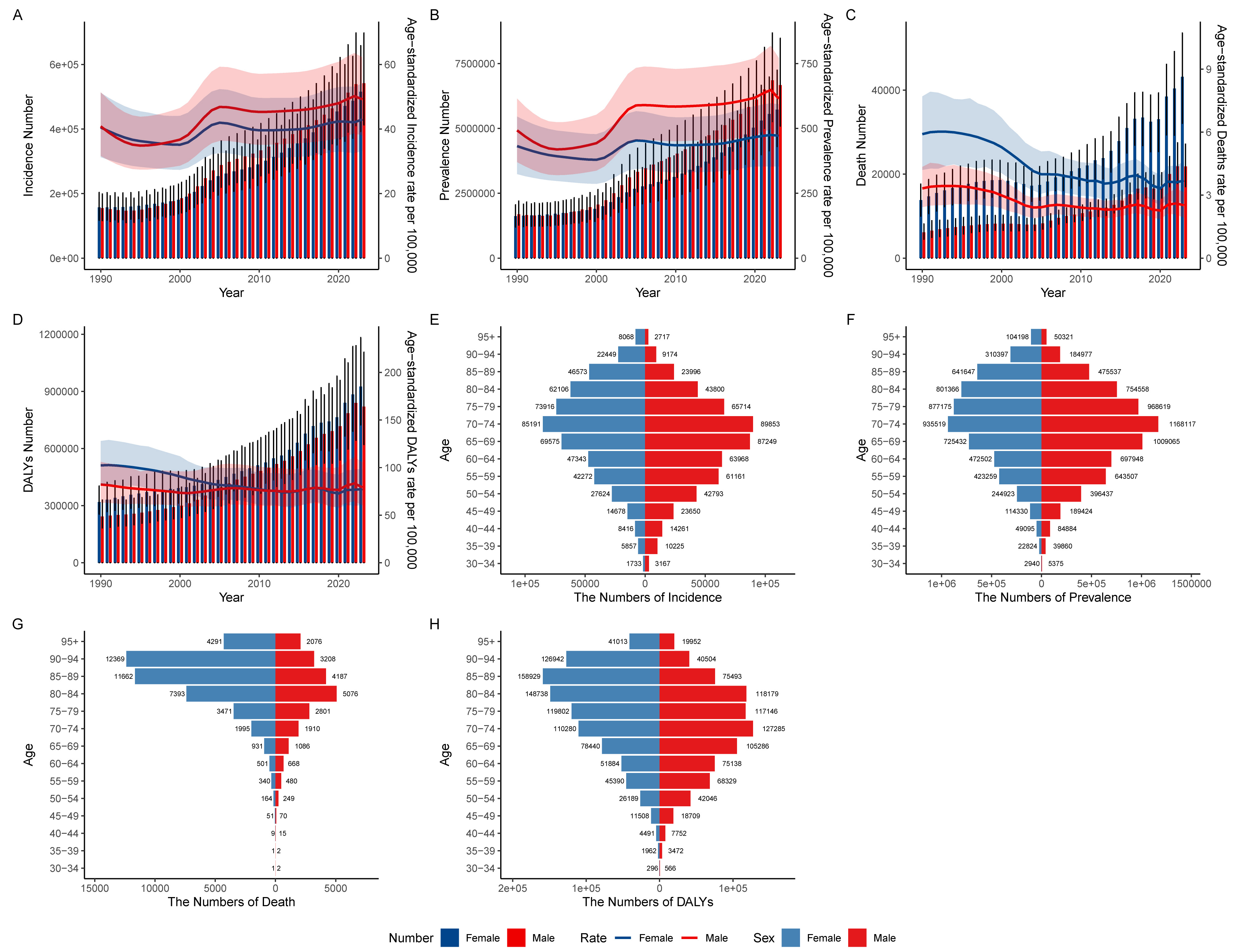
Figure 1. Trends in AF/AFL burden and age-standardized measures for males and females in China between 1990 and 2023 are shown. Panels (A-D) correspond to incidence, prevalence, mortality, and DALYs, respectively; Panels (E-H) depict the age-specific distributions in 2023 for incident cases (E), prevalent cases (F), deaths (G), and DALYs (H) in males and females. AF/AFL: Atrial fibrillation and flutter; DALYs: disability-adjusted life years.
Specifically, the number of incident AF/AFL cases in China increased from 312,558 (95% UI: 233,376-399,993) in 1990 to 1,057,528 (95% UI: 809,494-1,352,720) in 2023. Over the same period, the number of prevalent cases rose from 3,307,425 (95% UI: 2,484,120-4,223,896) to 12,394,235 (95% UI: 9,435,370-15,598,110). For both incident and prevalent cases, the absolute numbers were consistently higher in males than in females [Table 1]. In contrast, the number of deaths attributable to AF/AFL increased from 19,947 (95% UI: 15,522-24,005) in 1990 to 65,008 (95% UI: 51,849-75,275) in 2023, while DALYs rose from 562,194 (95% UI: 452,649-720,720) to 1,745,719 (95% UI: 1,398,854-2,293,705). Notably, females accounted for a higher number of deaths and DALYs than males throughout the study period. In summary, while males consistently exhibited higher incidence and prevalence, females had higher burden in terms of mortality and DALYs.
The numbers of cases and age-standardized rates of incidence, prevalence, mortality, and DALYs of AF/AFL in China in 1990 and 2023, along with the AAPC during the period from 1990 to 2023
| Characteristics | 1990 | 2023 | 1990-2023 | ||
| Incidence | No. (95% UI) | ASIR (95% UI) | No. (95% UI) | ASIR (95% UI) | AAPC (95%CI) |
| Both | 312558 (233376, 399993) | 41.33 (32.43, 51.93) | 1057528 (809494, 1352720) | 46.36 (36.04, 58.14) | 0.38 (0.29, 0.48) |
| Male | 155051 (116437, 198558) | 40.83 (31.7, 51.39) | 541727 (413163, 697731) | 49.22 (38.05, 62.24) | 0.62 (0.44, 0.80) |
| Female | 157507 (117292, 203568) | 40.49 (31.28, 51.23) | 515801 (392555, 658387) | 43 (33.23, 54.14) | 0.17 (0.03, 0.31) |
| Prevalence | No. (95% UI) | ASPR (95% UI) | No. (95% UI) | ASPR (95% UI) | AAPC (95%CI) |
| Both | 3307425 (2484120, 4223896) | 462.92 (348.45, 577.62) | 12394235 (9435370, 15598110) | 541.74 (410.72, 679.94) | 0.56 (0.36, 0.76) |
| Male | 1687948 (1276898, 2197692) | 492.33 (370.3, 614.68) | 6668627 (5090723, 8471959) | 614.89 (469.43, 771.41) | 0.80 (0.52, 1.07) |
| Female | 1619478 (1201607, 2058923) | 431.71 (324.17, 545.46) | 5725608 (4304441, 7245753) | 472.17 (353.46, 593.28) | 0.28 (0.23, 0.33) |
| Deaths | No. (95% UI) | ASMR (95% UI) | No. (95% UI) | ASMR (95% UI) | AAPC (95%CI) |
| Both | 19947 (15522, 24005) | 5.12 (3.89, 6.35) | 65008 (51849, 75275) | 3.23 (2.56, 3.76) | -1.38 (-1.81, -0.95) |
| Male | 6143 (4496, 8159) | 3.32 (2.43, 4.34) | 21829 (17019, 27147) | 2.52 (1.94, 3.14) | -0.79 (-1.30, -0.28) |
| Female | 13804 (10017, 17641) | 5.91 (4.2, 7.7) | 43179 (32101, 53609) | 3.69 (2.76, 4.6) | -1.46 (-1.89, -1.02) |
| DALYs | No. (95% UI) | ASDR (95% UI) | No. (95% UI) | ASDR (95% UI) | AAPC (95%CI) |
| Both | 562194 (452649, 720720) | 96.99 (78.52, 119.37) | 1745719 (1398854, 2293705) | 79.29 (64.23, 103.01) | -0.57 (-0.87, -0.26) |
| Male | 243089 (183667, 329097) | 82.22 (63.21, 105.92) | 819857 (621236, 1105794) | 79.24 (60.49, 105.46) | -0.04 (-0.29, 0.22) |
| Female | 319105 (255334, 403382) | 102.3 (82, 127.95) | 925862 (724013, 1182849) | 77.34 (60.6, 98.31) | -0.84 (-1.02, -0.66) |
With regard to age-standardized rates, the ASIR increased from 41.33 per 100,000 population (95% UI: 32.43-51.93) in 1990 to 46.36 per 100,000 population (95% UI: 36.04-58.14) in 2023, while the ASPR rose from 462.92 per 100,000 population (95% UI: 348.45-577.62) to 541.74 per 100,000 population (95% UI: 410.72-679.94). Across the study period, males exhibited higher ASIR and ASPR than females in most years. By contrast, the age-standardized mortality rate (ASMR) demonstrated an overall declining trend in China, decreasing from 5.12 per 100,000 population (95% UI: 3.89-6.35) in 1990 to 3.23 per 100,000 population
With respect to age distribution, in 2023, incident and prevalent AF/AFL cases in China reached their highest levels among individuals aged 70-74 years in both sexes. Prior to this age group, the numbers were higher in males than in females, whereas beyond the 70-74-year age group, females outnumbered males. For mortality and DALYs, older females accounted for substantially higher numbers than males, particularly among individuals aged 75 years and older [Figure 1E-H]. In summary, the burden of AF/AFL was concentrated in older populations, peaking at ages 70-74, with females experiencing disproportionately higher mortality and DALYs at advanced ages.
Joinpoint regression analysis of the burden of AF/AFL in China
To further characterize temporal trends in AF/AFL in China from 1990 to 2023 by sex, joinpoint regression analyses were conducted [Figure 2A-D]. The results indicated that the ASIR declined most rapidly during 1990-1994 in both males and females, with annual percent changes (APC) of -3.86 (P < 0.05) and -2.47 (P < 0.05), respectively. The most pronounced increases in ASIR were observed during 2000-2004 in males (APC = 6.37, P < 0.05) and during 2000-2005 in females (APC = 3.95, P < 0.05). After 2010, ASIRs in both sexes generally exhibited a slow upward trend.
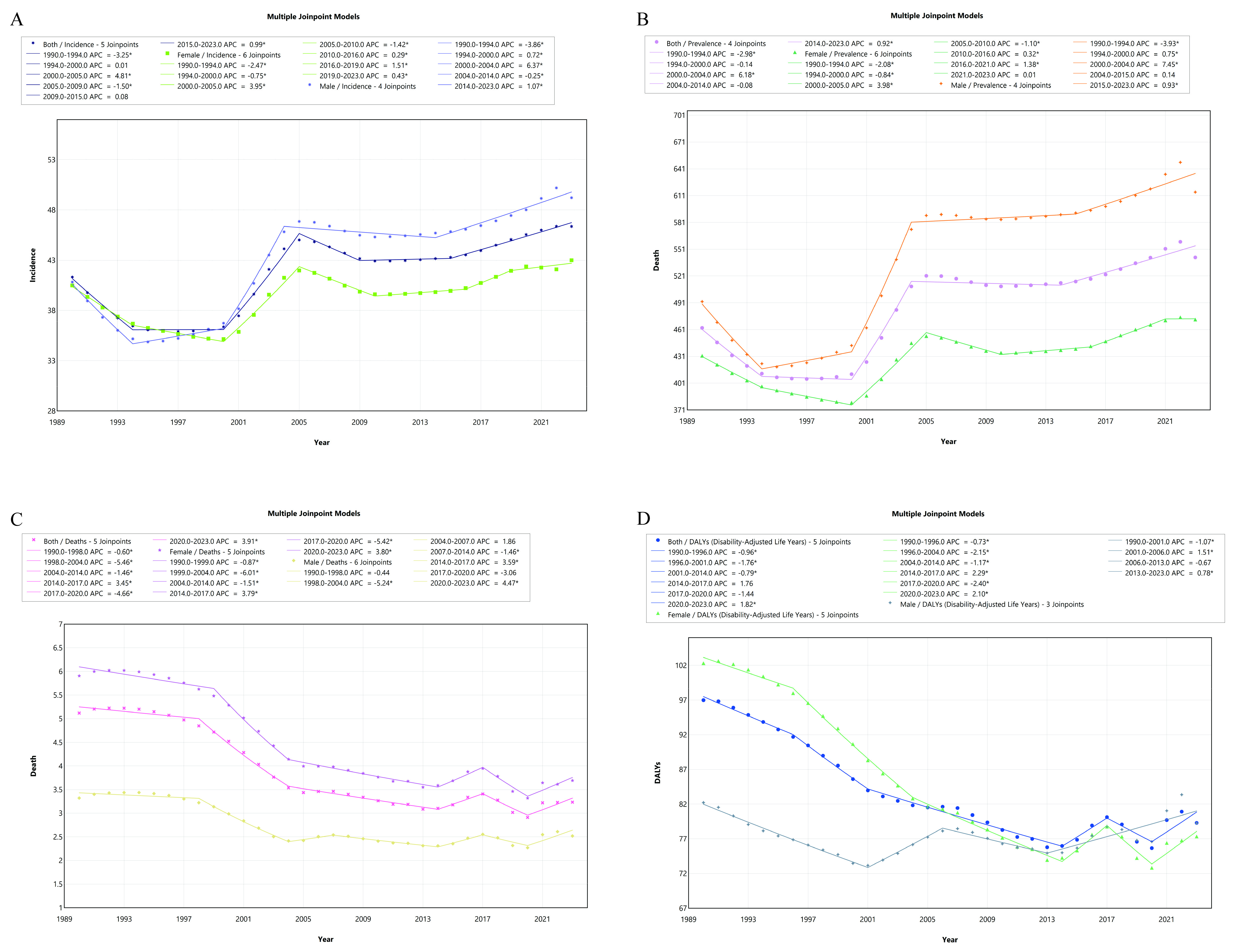
Figure 2. Joinpoint regression analysis illustrating changes in AF/AFL in males and females in China from 1990 to 2023: (A) incidence, (B) prevalence, (C) mortality, and (D) DALYs. (* indicates P < 0.05). AF/AFL: Atrial fibrillation and flutter; DALYs: disability-adjusted life years; APC: annual percent changes.
Similar temporal patterns were observed for the ASPR. The steepest declines occurred during 1990-1994, with APCs of -3.93 (P < 0.05) in males and -2.08 (P < 0.05) in females. The fastest increases in ASPR were identified during 2000-2004 among males (APC = 7.45, P < 0.05) and during 2000-2005 among females (APC = 3.98, P < 0.05).
The ASMR demonstrated an overall declining trend in both males and females. The most rapid decreases were observed during 1998-2004 in males (APC = -5.24, P < 0.05) and during 1999-2004 in females (APC = -6.01, P < 0.05). This trend reversed during 2020-2023, with ASMR increasing in both sexes, with APCs of 4.47 (P < 0.05) in males and 3.80 (P < 0.05) in females.
For ASDR, females experienced a prolonged period of decline, with the steepest decrease occurring during 1996-2004 (APC = -2.15, P < 0.05). Similar to the pattern observed for ASMR, both males and females exhibited increasing ASDR during 2020-2023, with APCs of 0.78 (P < 0.05) and 2.10 (P < 0.05), respectively.
Age-period-cohort model analysis
To further clarify the independent contributions of age, period, and cohort to AF/AFL patterns in China by sex, age-period-cohort model analyses were performed. Regarding incidence, rates in females surpassed those in males beyond the 75-79-year age group. Both period and cohort patterns suggested a progressive rise in incidence over successive calendar periods and cohorts [Figure 3A-C]. Among individuals born after 1944, males showed higher incidence rates compared with females [Supplementary Table 2].
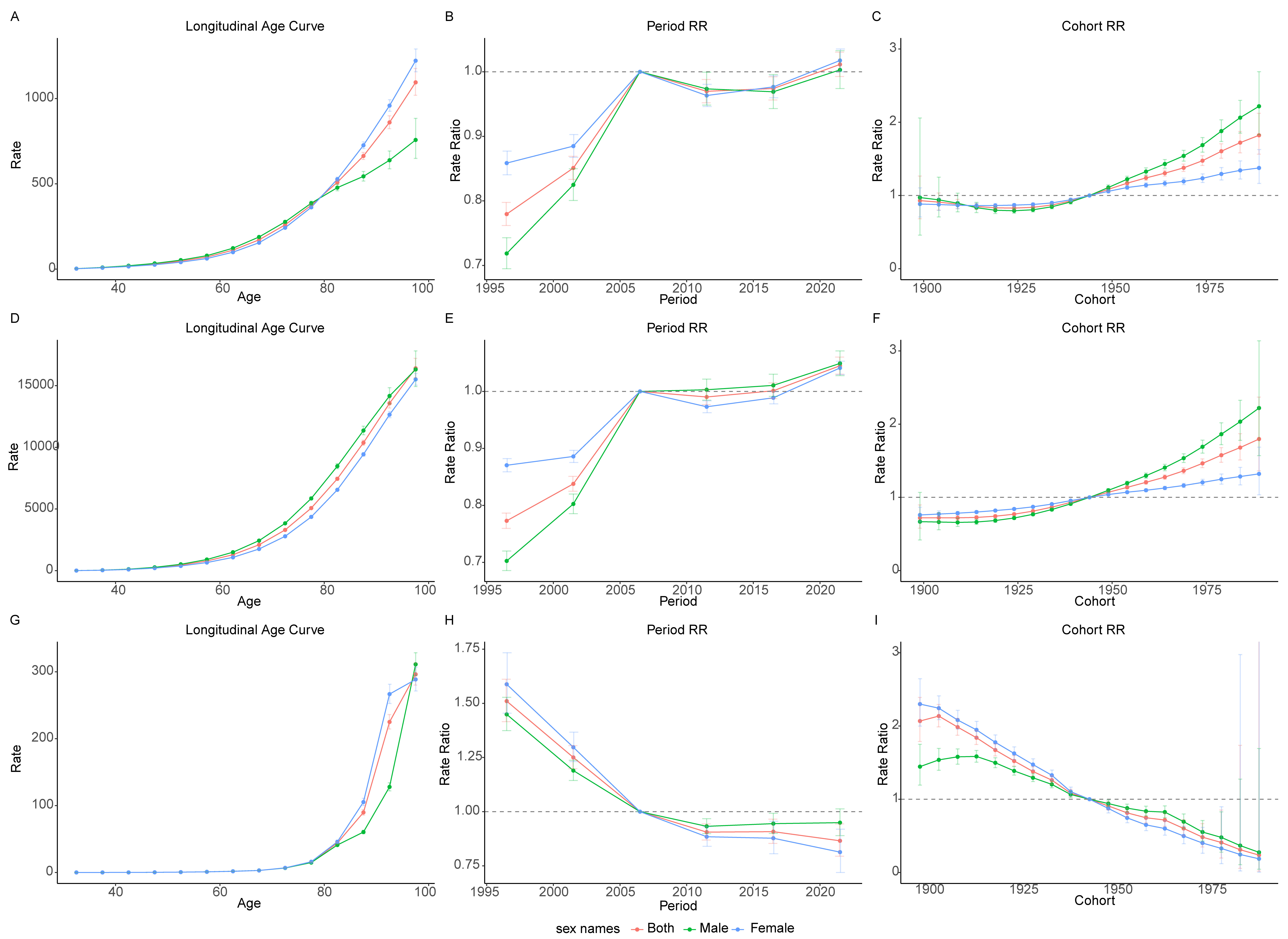
Figure 3. Age-period-cohort analysis of incidence, prevalence, and mortality rates among males and females in China, 1994-2023. Panels (A-C) show the longitudinal age (A), period relative risk (RR) (B), and cohort RR (C) for incidence; Panels (D-F) present the longitudinal age (D), period RR (E), and cohort RR (F) for prevalence; and Panels (G-I) depict the longitudinal age (G), period RR (H), and cohort RR (I) for mortality.
The patterns observed for prevalence were generally consistent with those for incidence in both period and cohort effects, with higher prevalence rates among males born after 1944 [Supplementary Table 3], which may partly reflect the increased incidence in this birth cohort. In terms of age effects, prevalence rates were consistently higher in males than in females across all age groups [Figure 3D-F].
For mortality, age effects showed no marked sex differences before the 80-84-year age group; however, beyond this age, mortality rates were higher in females than in males. Regarding period effects, males had lower mortality rates than females before 2004-2009, whereas males surpassed females thereafter [Supplementary Table 4]. Similarly, cohort effects revealed higher mortality rates among males born after 1944 compared with their female counterparts [Figure 3G-I].
Decomposition analysis of the burden of AF/AFL
To further quantify the contributions of aging, population growth, and epidemiological change to the burden of AF/AFL, a decomposition analysis was performed. Between 1990 and 2023, aging, population growth, and epidemiological change all contributed to the increases in incidence and prevalence, with aging as the predominant driver in both males and females [Figure 4A and B]. In the total population, aging accounted for 72.62% of the increase in incidence and 70.90% of the increase in prevalence [Supplementary Table 5].
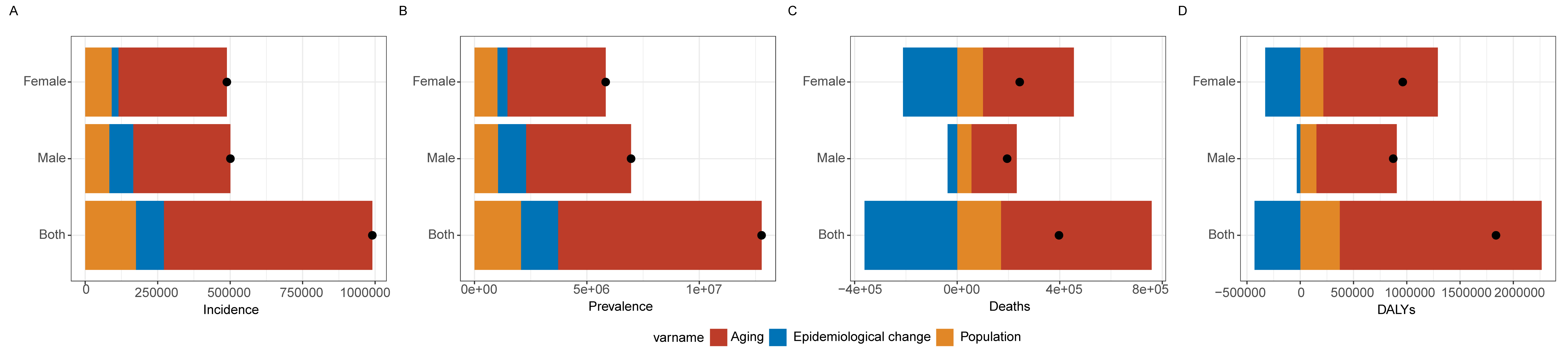
Figure 4. Decomposition analysis of changes in incidence (A), prevalence (B), mortality (C), and DALYs (D) among males and females in China from 1990 to 2023, attributed to aging, population growth, and epidemiological change. The black dots in each panel indicate the overall changes resulting from the combined effects of these three components. DALYs: Disability-adjusted life years.
In contrast, epidemiological change contributed negatively to mortality and DALYs [Figure 4C and D], indicating overall declines in AF/AFL-related mortality and DALYs in China from 1990 to 2023. This negative contribution was more pronounced among females, accounting for -86.62% of the change in mortality and -34.22% of the change in DALYs. Nevertheless, aging remained the dominant contributor to changes in mortality and DALYs, accounting for 147.95% and 103.17% of the total change in the overall population, respectively.
Frontier analysis of AF/AFL burden
To examine changes in the ASDR in China in relation to increasing sociodemographic development, a frontier analysis was performed using data from 204 countries and territories spanning 1990-2023. The results showed that China’s ASDR declined steadily from 1990 (96.99 per 100,000 population) to 2013 (75.78 per 100,000 population) [Supplementary Table 6]. Thereafter, ASDR exhibited a fluctuating pattern and demonstrated an overall upward trend after 2020 [Figure 5A].
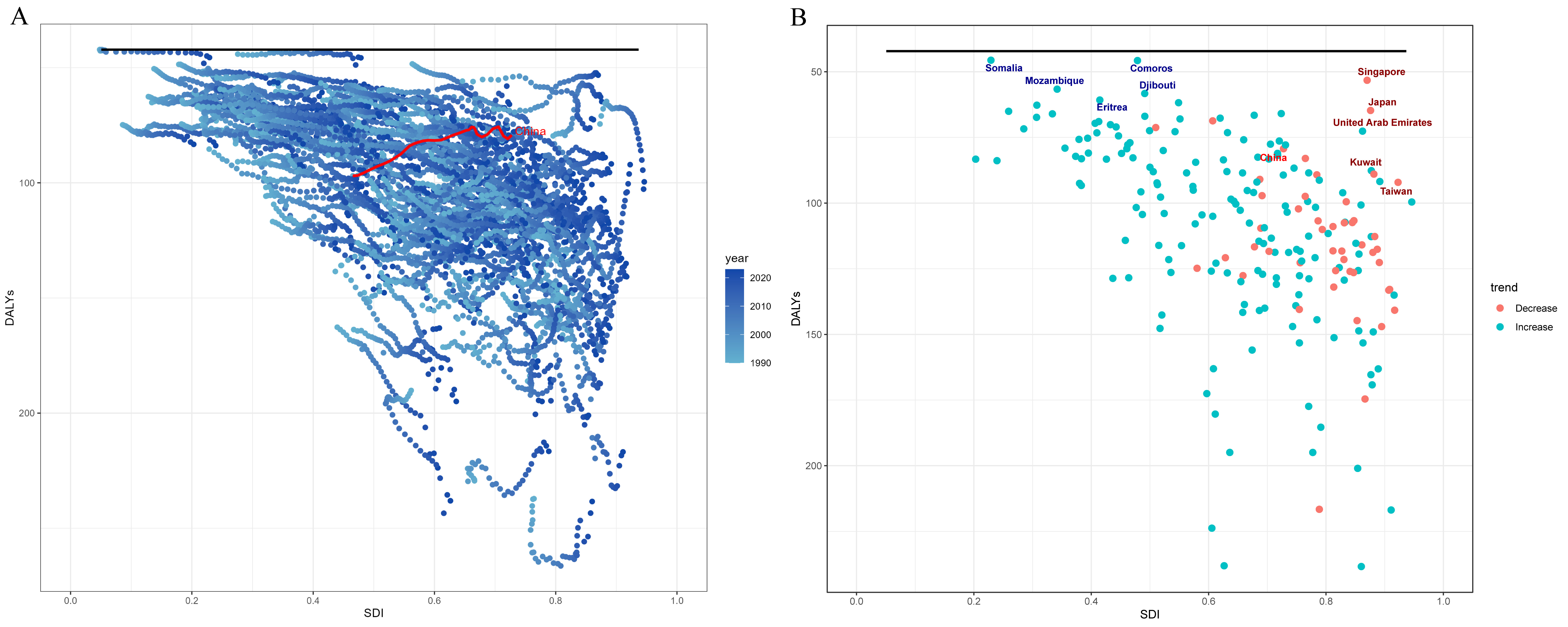
Figure 5. Association between DALYs and SDI across 204 countries and territories. Panel A shows DALYs trends in relation to SDI from 1990 to 2023. Panel B shows the distribution of DALYs versus SDI in 2023, with blue labels indicating the five locations with the lowest DALYs among those with SDI < 0.5 and red labels indicating those with the lowest DALYs among locations with SDI > 0.85. DALYs: Disability-adjusted life years; SDI: socio-demographic index.
Furthermore, among countries and territories with an SDI < 0.5 in 2023, the five locations with the lowest ASDR were Somalia, Comoros, Mozambique, Djibouti, and Eritrea [Figure 5B], with Somalia showing the lowest burden (45.61 per 100,000 population). Similarly, among countries and territories with an SDI > 0.85, the five locations with the lowest ASDR were Singapore, Japan, the United Arab Emirates, Kuwait, and Taiwan (China), among which Singapore had the lowest ASDR (53.25 per 100,000 population).
Projected trends in AF/AFL burden over the coming 15 years
ARIMA models were applied to estimate future patterns of AF/AFL burden in China for the upcoming 15-year period. The projections indicated that the ASIR among males is projected to decline from 49.22 per 100,000 population in 2023 to 41.14 per 100,000 population in 2028, followed by a plateau thereafter. In contrast, ASIR among females is projected to increase from 42.00 per 100,000 population in 2023 to 49.50 per 100,000 population in 2028 [Supplementary Table 7], followed by a gradual decline to 47.10 per 100,000 population by 2033 [Figure 6A-C].
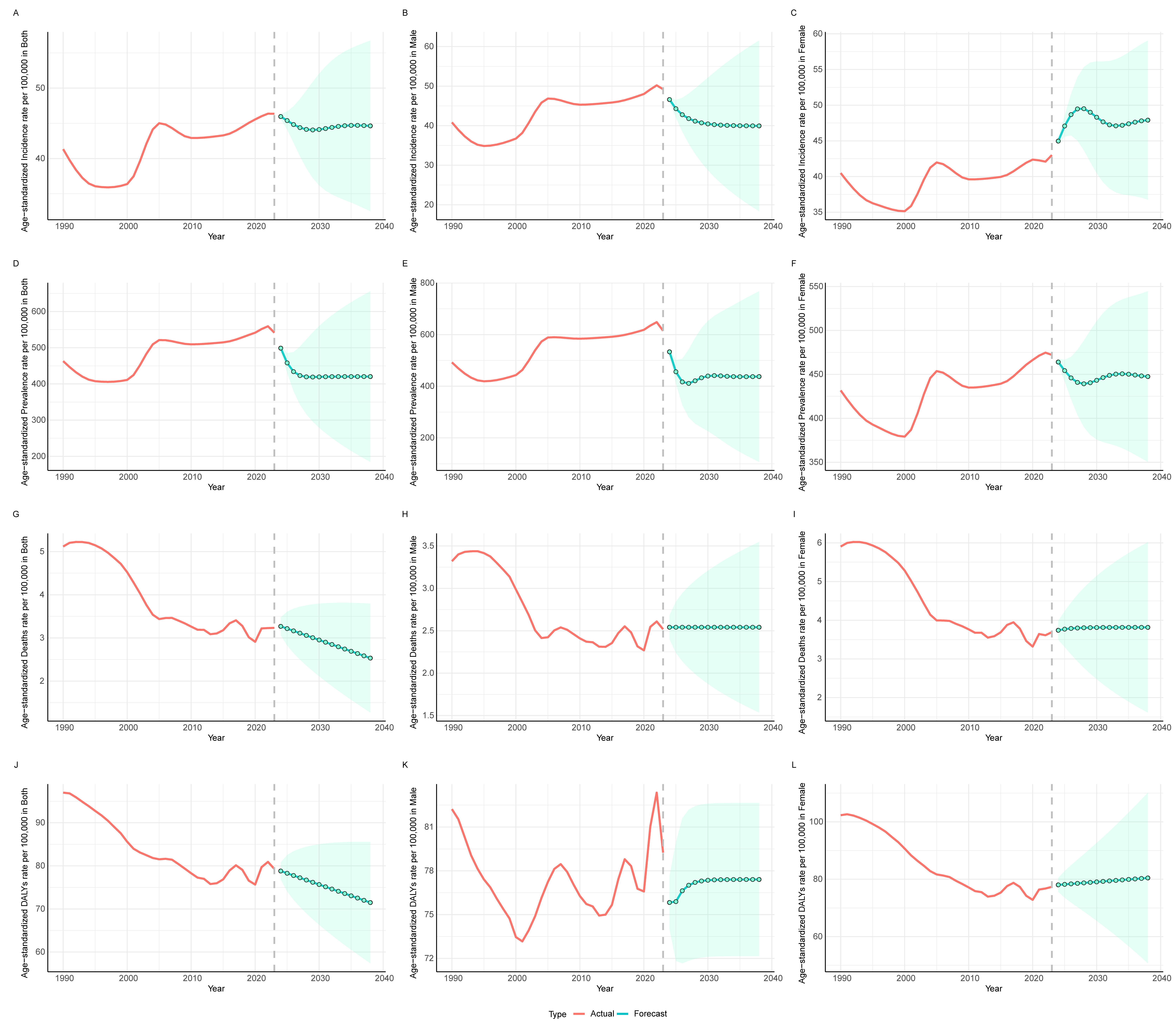
Figure 6. ARIMA forecasts of disease burden trends among males and females in China from 2024 to 2038. Panels (A-C) show the projected incidence rates for both sexes (A), males (B), and females (C); Panels (D-F) present the projected prevalence rates for both sexes (D), males (E), and females (F); Panels (G-I) depict the projected mortality rates for both sexes (G), males (H), and females (I); and Panels (J-L) illustrate the projected DALYs for both sexes (J), males (K), and females (L) over the 15-year period. The red solid line represents the trend of observed values from 1990 to 2023, the green dots indicate the projected values over the subsequent 15 years, and the green shaded area denotes the 95% confidence interval of the forecasts. ARIMA: Autoregressive integrated moving average; DALYs: disability-adjusted life years.
For prevalence, the ASPR among males is projected to decrease from 614.89 per 100,000 population in 2023 to 410.89 per 100,000 population in 2027. A similar declining trend is projected among females, with ASPR decreasing from 472.17 per 100,000 population in 2023 to 439.25 per 100,000 population in 2028 [Figure 6D-F].
Regarding mortality and overall disease burden, both the ASMR and the ASDR in the total population are projected to decline steadily over the next 15 years, decreasing from 3.23 to 2.53 per 100,000 population and from 79.29 to 71.48 per 100,000 population, respectively, between 2023 and 2038 [Figure 6G-L].
DISCUSSION
In this nationwide assessment of the burden of AF/AFL in China from 1990 to 2023, we identified marked increases in the total counts of new cases, existing cases, deaths, and DALYs in both sexes, largely driven by population aging and growth. Despite these increases in absolute burden, age-standardized rates exhibited heterogeneous temporal patterns. Specifically, the ASIR and ASPR initially declined and subsequently increased, whereas the ASMR and ASDR generally decreased but showed a modest rebound after 2020. Clear sex- and age-specific differences were also observed. Males had higher incidence and prevalence, whereas females experienced higher mortality and DALYs, particularly at older ages.
The age effect estimated from the age-period-cohort model demonstrated a clear increasing trend in AF/AFL incidence with advancing age. Consistent with this finding, the decomposition analysis further indicated that population aging was the dominant contributor to the increase in incidence. Accumulating evidence from prior studies has similarly shown that the incidence of atrial fibrillation rises markedly with age. A systematic review has reported that approximately 70% of patients with AF are aged between 65 and 85 years, underscoring the strong association between older age and the occurrence of AF[17]. Similarly, longitudinal cohort studies have shown that the incidence of AF rises significantly with age, further elucidating the age-dependent pattern of AF burden and indicating a steep increase in AF incidence among older populations[18,19].
From a pathophysiological perspective, aging is accompanied by structural and electrophysiological alterations in the myocardium. The concept of atrial cardiomyopathy has been proposed as an integrated framework describing a spectrum of atrial structural, architectural, contractile, and electrophysiological changes that underlie AF[20]. Previous studies have suggested that aging, neurohormonal activation, and chronic atrial stretch secondary to structural heart disease can activate multiple signaling pathways, leading to cardiomyocyte hypertrophy, fibroblast proliferation, and complex remodeling of the extracellular matrix, including atrial fibrosis[21,22]. These changes disrupt normal atrial conduction and electrical stability, thereby predisposing older individuals to the development and persistence of atrial arrhythmias, including AF.
In the present study, we observed a sustained decline in AF/AFL-related mortality in China over the past decades, which may be partly attributable to improvements in healthcare infrastructure and advances in therapeutic strategies. The widespread use of anticoagulation therapy and rhythm-control approaches, including catheter ablation, has been associated with reduced stroke risk and improved clinical outcomes in patients with AF[23,24]. Risk stratification tools, such as Predicting Bleeding Complications in Patients Undergoing Stent Implantation and Subsequent Dual-Antiplatelet Therapy (PRECISE-DAPT) and Academic Research Consortium for High Bleeding Risk (ARC-HBR), have been developed to assess bleeding risk in patients receiving antithrombotic therapy, although their applicability in AF populations remains under investigation. More recently, the PRECISE-HBR score, which integrates features of both tools, has been proposed to improve bleeding risk prediction in patients undergoing complex antithrombotic treatment[25-28].
In parallel, advances in medical technology have played an important role in improving AF management. The adoption of remote monitoring systems and telecardiology services enable continuous surveillance of patients’ cardiac rhythm, facilitating early detection of disease progression and timely clinical intervention, thereby helping to prevent severe complications[29]. In addition, wearable devices and mobile health applications have enhanced patient engagement and treatment adherence while allowing clinicians to monitor disease status more closely[30]. However, the effectiveness of these technologies depends on adequate digital health literacy, which is often limited among older adults and frail populations[31,32]. This limitation may reduce the usability and effectiveness of wearable monitoring, despite the higher disease burden in these groups. Moreover, disparities in digital access and the lack of standardized clinical workflows remain important challenges, potentially limiting the integration of these technologies into routine care and affecting the accurate assessment and management of AF.
In our study, older females experienced higher incidence and mortality rates than males, highlighting sex-specific differences in the burden of AF/AFL. Increasing evidence suggests that sex hormones, particularly estrogen, may play a protective role against the development of AF through multiple biological mechanisms. One major pathway involves the modulation of cardiac ion channels and electrophysiological properties. Experimental and clinical studies have demonstrated that estrogen can regulate the expression and function of ion channels, thereby influencing cardiac conduction and excitability[33]. In addition, estrogen exerts antioxidant effects that may reduce oxidative stress within myocardial tissue. Because oxidative stress is a major contributor to structural and electrical remodeling in AF, attenuation of these processes may help prevent maladaptive atrial remodeling and reduce susceptibility to AF[34].
Beyond biological mechanisms, sex-related differences in clinical presentation may further contribute to disparities in AF outcomes. Middle-aged and older women are more likely to present with atypical symptoms at the time of AF diagnosis, which may increase the risk of underdiagnosis and delayed treatment. While symptoms such as fatigue, dyspnea, and palpitations are common, women are less likely to experience classic or pronounced palpitations, potentially leading healthcare providers to underestimate their risk of AF[34]. This under-recognition may lead to suboptimal management and delayed intervention, ultimately contributing to worse outcomes. Moreover, women with AF frequently have a higher burden of comorbidities, such as hypertension and heart failure, which can further complicate symptom presentation and disease management, thereby contributing to poorer prognoses[35].
The cohort effect estimated from the age-period-cohort model revealed that males born after 1944 exhibited higher AF/AFL incidence rates than females, with the sex gap widening across successive birth cohorts. This pattern may be partly attributable to sex-specific lifestyle behaviors, particularly higher prevalences of alcohol consumption and smoking among males. Excessive alcohol intake and tobacco use have been shown to promote atrial remodeling through inflammatory and fibrotic pathways, thereby increasing susceptibility to AF[36]. In addition, contemporary lifestyle characteristics, including accelerated pace of life, chronic sleep deprivation, and heightened psychological stress, may further contribute to this cohort-specific increase in AF risk. These factors are closely linked to the development of hypertension, which is widely recognized as a major and modifiable risk factor for AF, accounting for approximately 25% of AF cases[37].
Insights from the frontier analysis suggest that among countries and territories with an SDI greater than 0.85, particular attention should be paid to Japan, Singapore, and Taiwan (China). Given their shared ethnic background with mainland China, these regions may offer valuable lessons in effective AF prevention and management strategies, including early screening, integrated care models, and optimized risk factor control.
Finally, the ARIMA-based projections for males demonstrated a pronounced stepwise decline, especially in DALYs. This pattern may reflect substantial fluctuations in the observed values between 2022 and 2023, which may have introduced instability into the time-series models and increased variability in the projections.
Limitations
This study has several limitations that warrant consideration. First, the analyses were based on nationally aggregated data, which may obscure substantial regional and subnational heterogeneity in the burden of AF/AFL. As a result, the findings may have limited applicability for informing individual-level research or locally tailored interventions. Second, reliance on secondary data sources may introduce potential biases, including inaccuracies in data collection, misclassification or misdiagnosis of disease, and reporting bias, particularly in low-SDI settings where limited healthcare access and weaker surveillance systems may lead to underdiagnosis and incomplete cause-of-death registration. Third, estimates from the GBD framework are model-based and depend on statistical assumptions and data imputation, especially in regions with sparse or low-quality data, which may introduce uncertainty and affect the robustness of the results. Although uncertainty intervals are provided, they may not fully capture all sources of systematic error. Fourth, temporal trends may be influenced by changes in diagnostic criteria, coding practices, and the accessibility of healthcare services over time, which can compromise the comparability of estimates across years and, consequently, reduce the accuracy of ARIMA models in forecasting future trends.
In addition, the GBD database categorizes multiple conditions into relatively broad disease groups, which may mask specific clinical subtypes or contextual health issues that warrant targeted prevention and management strategies. Future studies incorporating more granular, regionally representative, and individual-level data are needed to better characterize local patterns of AF/AFL burden and to support the development of more precise and effective public health interventions.
Conclusions
Despite improvements in age-standardized mortality and DALYs, the overall burden of AF/AFL in China continues to increase, primarily driven by population aging. Targeted prevention, early detection, and optimized management strategies - particularly among older adults and high-risk males - are urgently needed.
DECLARATIONS
Authors’ contributions
Contributed equally to this work and share first authorship: Xu, S.; Li, Y.
Responsible for conceptualization, study design, data collection, statistical analysis, and drafting of the manuscript: Xu, S.
Contributed to data analysis, interpretation of results, and critical revision of the manuscript: Li, Y.
Performed the literature review, data curation, and preparation of figures and tables: Lin, F.
provided methodology guidance, validation of analysis, and manuscript review: Zuo, P.
Supervised research methods, coordinated the project, and critically revised the manuscript: Fan, J.
Oversaw the overall study, secured funding, supervised the project, and provided final approval of the manuscript: Yang, X.
All authors have read and approved the final version of the manuscript.
Availability of data and materials
The Global Burden of Disease study 2023 is an open-access resource; data are available at https://vizhub.healthdata.org/gbd-results.
AI and AI-assisted tools statement
Not applicable.
Financial support and sponsorship
This study was supported by the National Natural Science Foundation of China [No. 82470533] and by a horizontal research project [No. 2023100].
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
Supplementary Materials
REFERENCES
1. Nieuwlaat R, Capucci A, Camm AJ, et al. Atrial fibrillation management: a prospective survey in ESC member countries. Eur Heart J. 2005;26:2422-34.
2. Jin Y, Wang K, Xiao B, et al. Global burden of atrial fibrillation/flutter due to high systolic blood pressure from 1990 to 2019: estimates from the global burden of disease study 2019. J Clin Hypertens. 2022;24:1461-72.
3. Sethi NJ, Safi S, Feinberg J, Nielsen EE, Gluud C, Jakobsen JC. Digoxin versus placebo, no intervention, or other medical interventions for atrial fibrillation and atrial flutter: a protocol for a systematic review with meta-analysis and trial sequential analysis. Syst Rev. 2017;6:71.
4. Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham study. Stroke. 1991;22:983-8.
5. Suomalainen OP, Martinez-majander N, Broman J, et al. Stroke in patients with atrial fibrillation: epidemiology, screening, and prognosis. J Clin Med. 2023;13:30.
6. Srichawla BS, Hamel AP, Cook P, et al. Is catheter ablation associated with preservation of cognitive function? Front. Neurol. 2024;14:1302020.
7. Lucà F, Abrignani MG, Oliva F, et al. Multidisciplinary approach in atrial fibrillation: as good as gold. J Clin Med. 2024;13:4621.
8. Kong X, Li M, He L, et al. Burden of atrial fibrillation and atrial flutter from 1990 to 2021 in China: global burden of disease study 2021 update. Pacing Clin Electrophysiol. 2025;48:447-54.
9. Wang Z, Chen Z, Wang X, et al. The disease burden of atrial fibrillation in China from a national cross-sectional survey. Am J Cardiol. 2018;122:793-8.
10. Zhang C, Zhang X, Zhou R, et al. Secular trend in disease burden of atrial fibrillation/flutter in China from 1992 to 2021 and its projection in 25 years. BMC Public Health. 2025;25:2064.
11. Murray CJL, Abbafati C, Abbas KM, et al. Five insights from the global burden of disease study 2019. Lancet. 2020;396:1135-59.
12. Yang G, Ouyang H, Zhao Z, et al. Discrepancies in neglected tropical diseases burden estimates in China: comparative study of real-world data and global burden of disease 2021 data (2004-2020). BMJ. 2025;388:e080969.
13. Dong X, Wang B, Hou F, et al. Global burden of atrial fibrillation/atrial flutter and its attributable risk factors from 1990 to 2019. EP Europac. 2023;25:793-803.
14. Pellicer PS, Tamayo RG, López VN. Reducing test request for anti-thyroglobulin and anti-thyroid peroxidase antibodies: trends before and after interventions based on rejection rules and profile management. Biochemia Medica. 2018;28:030709.
15. Rosenberg PS, Check DP, Anderson WF. A web tool for age-period-cohort analysis of cancer incidence and mortality rates. Cancer Epidemiol Biomarkers Prev. 2014;23:2296-302.
16. Xu S, Liu Z, Tang M, Xu C. Burden, risk factors, and projections of ischemic heart disease in China (1990-2021): findings from the 2021 GBD study. Front. Cardiovasc. Med. 2025;12:1549147.
17. Bul M, Shaikh F, Mcdonagh J, Ferguson C. Frailty and oral anticoagulant prescription in adults with atrial fibrillation: a systematic review. Aging Med. 2022;6:195-206.
18. Kannel WB, Abbott RD, Savage DD, Mcnamara PM. Epidemiologic features of chronic atrial fibrillation: the framingham study. N Engl J Med. 1982;306:1018-22.
19. Von Olshausen G, Schwieler J, Bastani H, et al. Incidence of atrial fibrillation and its association with long-term outcome in patients with an accessory pathway. Front Cardiovasc Med. 2025;12:1639305.
20. Goette A, Corradi D, Dobrev D, et al. Atrial cardiomyopathy revisited-evolution of a concept: a clinical consensus statement of the European Heart Rhythm Association (EHRA) of the ESC, the Heart Rhythm Society (HRS), the Asian Pacific Heart Rhythm Society (APHRS), and the Latin American Heart Rhythm Society (LAHRS). Europace. 2024;26:euae204.
21. Diallo EH, Brouillard P, Raymond JM, Liberman M, Duceppe E, Potter BJ. Predictors and impact of postoperative atrial fibrillation following thoracic surgery: a state‐of‐the‐art review. Anaesthesia. 2023;78:491-500.
22. Schotten U, Verheule S, Kirchhof P, Goette A. Pathophysiological mechanisms of atrial fibrillation: a translational appraisal. Physiol Rev. 2011;91:265-325.
23. Hylek EM, Go AS, Chang Y, et al. Effect of intensity of oral anticoagulation on stroke severity and mortality in atrial fibrillation. N Engl J Med. 2003;349:1019-26.
24. Roy D, Talajic M, Nattel S, et al. Rhythm control versus rate control for atrial fibrillation and heart failure. N Engl J Med. 2008;358:2667-77.
25. Andreotti F, Geisler T, Collet J, et al. Acute, periprocedural and longterm antithrombotic therapy in older adults. Eur Heart J. 2023;44:262-79.
26. Schukraft S, Huwyler T, Ottiger-mankaka C, et al. Bleeding risk profile in patients on oral anticoagulation undergoing percutaneous coronary interventions: a prospective 24 months cohort study. Front. Cardiovasc. Med. 2021;8:589426.
27. Capolongo A, De Sio V, Gragnano F, et al. Long-term antithrombotic therapy in patients with atrial fibrillation and percutaneous coronary intervention. JCM. 2025;14:3713.
28. Gragnano F, Van Klaveren D, Heg D, et al. Derivation and validation of the PRECISE-HBR score to predict bleeding after percutaneous coronary intervention. Circulation. 2025;151:343-55.
29. Scalvini S, Piepoli M, Zanelli E, Volterrani M, Giordano A, Glisenti F. Incidence of atrial fibrillation in an Italian population followed by their GPs through a telecardiology service. Int J Cardiol. 2005;98:215-20.
30. Srinivasan NT, Schilling RJ. ; Barts Heart Centre, St Bartholomew’s Hospital, London, UK. Sudden cardiac death and arrhythmias. Arrhythm Electrophysiol Rev. 2018;7:111.
31. Vitolo M, Ziveri V, Gozzi G, et al. DIGItal health literacy after COVID-19 outbreak among frail and non-frail cardiology patients: the DIGI-COVID study. J Pers Med. 2022;13:99.
32. Simonson JK, Anderson M, Polacek C, Klump E, Haque SN. Characterizing real-world implementation of consumer wearables for the detection of undiagnosed atrial fibrillation in clinical practice: targeted literature review. JMIR Cardio. 2023;7:e47292.
33. Gowd BMP, Thompson PD. Effect of female sex on cardiac arrhythmias. Cardiol Rev. 2012;20:297-303.
34. Ko D, Rahman F, Martins MAP, et al. Atrial fibrillation in women: treatment. Nat Rev Cardiol. 2016;14:113-24.
35. Dagres N, Nieuwlaat R, Vardas PE, et al. Gender-related differences in presentation, treatment, and outcome of patients with atrial fibrillation in Europe. J Am Coll Cardiol. 2007;49:572-7.
36. Kim YG, Han K, Choi J, et al. Non-genetic risk factors for atrial fibrillation are equally important in both young and old age: a nationwide population-based study. Eur J Prev Cardiol. 2021;28:666-76.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Special Topic
Copyright

Data & Comments
Data
0











Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].