


Comparison of the “Modine modification” with the standard reimplantation technique: indications and options for improvement
 0
0 Abstract
Reimplantation using a Valsalva graft is a well-established and validated technique for valve-sparing root replacement with sinus reconstruction. In 2014, Modine and collegues et al. proposed a modification to the standard procedure in which the aortic valve is resuspended by simply attaching the tops of the commissures to the neo-sinutubular junction. This approach eliminates the need for continuous in-graft suturing of the aortic wall remnants. However, a major concern with this technique is the creation of a gap between the commissures and the graft, along with concentrated diastolic hemodynamic stress at the suture sites securing the commissural posts. Recently, we introduced an enhancement to the modine modification by securing the commissural posts more firmly to the Valsalva graft using longitudinal pledgeted sutures placed within the interleaflet triangles. Early short-term outcomes of this approach called the simplified reimplantation appear promising. The aim of this commentary is to describe the simplified reimplantation technique, evaluate its potential advantages over the Modine modification and define its appropriate indications.
Keywords
INTRODUCTION
David and Feindel first described aortic valve-sparing reimplantation in 1992[1]. The procedure involved replacing the dilated aortic root and reimplanting the patient’s native aortic valve (AV) inside a straight tubular graft[1]. The AV was secured at two levels: below the leaflets using horizontal mattress sutures, and above the leaflets by suturing the remaining arterial wall to the Dacron graft. The proximal suture line corrects annulo-aortic ectasia, while the continuous suture of the aortic wall remnants serves a hemostatic function.
In 2000, the Valsalva graft was introduced, representing a further advancement toward more physiological root reconstruction and improved leaflet motion[2].
Since the conceptualization of the reimplantation technique, various technical modifications have been developed, all aiming to restore the normal geometry of the functional aortic annulus and stabilize the virtual basal ring (VBR) to ensure long-term durability[3,4].
In 2014, El Arid et al.[5] proposed a modification to the standard technique that eliminated the need for the hemostatic suture between the aortic wall remnants and the Dacron graft. In this approach, following excision of the sinuses, the Dacron graft is anchored to the VBR using a single line of closely spaced, pledgeted sutures - similar to the Bentall procedure. The AV is then resuspended by attaching each commissural tab to the neo-sinutubular junction (STJ) with one or more pledgeted sutures. Thus, the proximal suture line simultaneously serves as a hemostatic seal, corrects annulo-aortic ectasia, and prevents annular dilation. According to the authors, the benefits of this modification include shorter cross-clamp time, reduced bleeding risk, and better preservation of root geometry. A few years later, Modine and colleagues presented a retrospective cohort study comparing outcomes between the modified and standard reimplantation techniques, reporting similarly favorable preliminary results[6]. However, as they correctly noted, the Modine modification leaves a space between the commissures and the graft, which is exposed to high hemodynamic pressure [Figure 1]. Upon pressurization, the pledgeted sutures anchoring the commissural posts must withstand the full hemodynamic load. In our opinion, this is the principal limitation of the Modine technique. Another drawback is the absence of individually reconstructed sinuses, which are present in standard reimplantation.
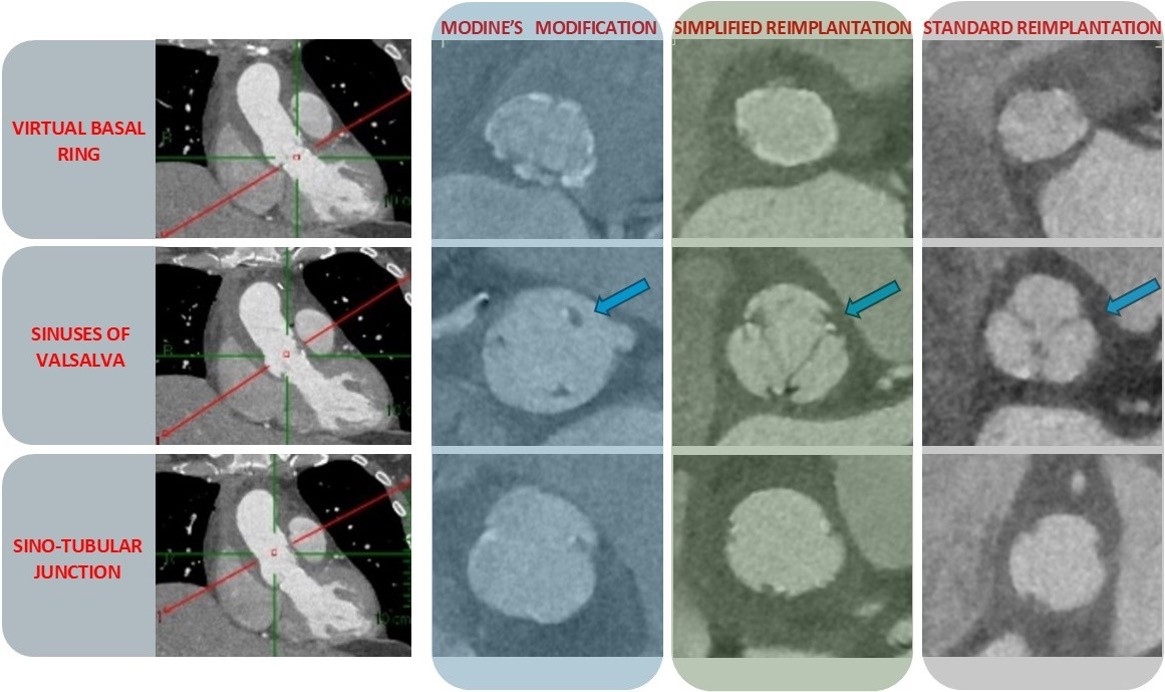
Figure 1. Early postoperative ECG-gated contrast-enhanced computed tomography (CT) scans showing short-axis views at various levels of the aortic root: the virtual basal ring, the sinuses of Valsalva, and the commissures. Note the absence of contrast agent behind the commissures in both the standard and simplified reimplantation techniques, whereas contrast is clearly visible behind the commissures in the Modine modification (indicated by blue arrows).
We recently reported an improvement to the modine modification[7], in which the commissural posts are more securely attached to the Valsalva graft using longitudinal pledgeted sutures placed within the interleaflet triangles [Figure 2]. Between December 2022 and January 2025, we employed this technique in 17 patients (3 with bicuspid and 14 with tricuspid AVs) as a bailout strategy when the aortic remnants were deemed too fragile for direct suturing to the Dacron graft. Early outcomes were favorable, with echocardiography showing no or only trivial aortic regurgitation and no reoperations required to date.
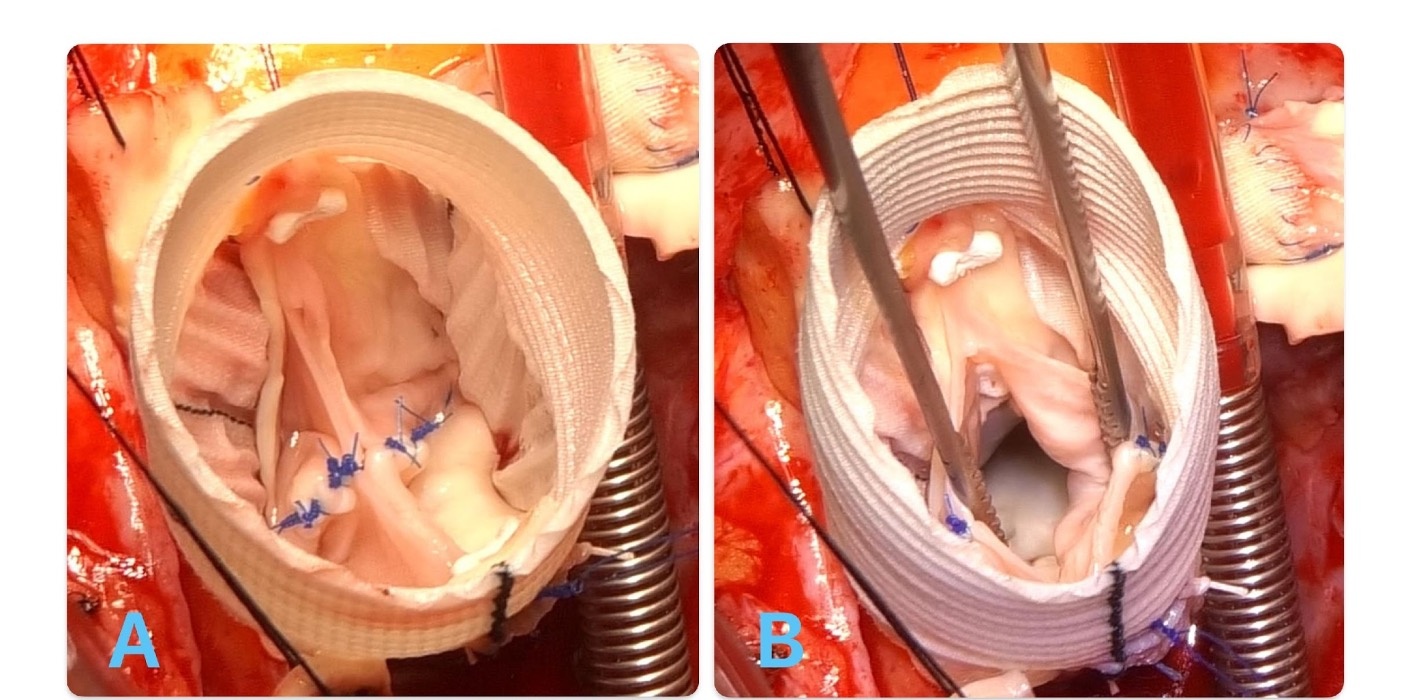
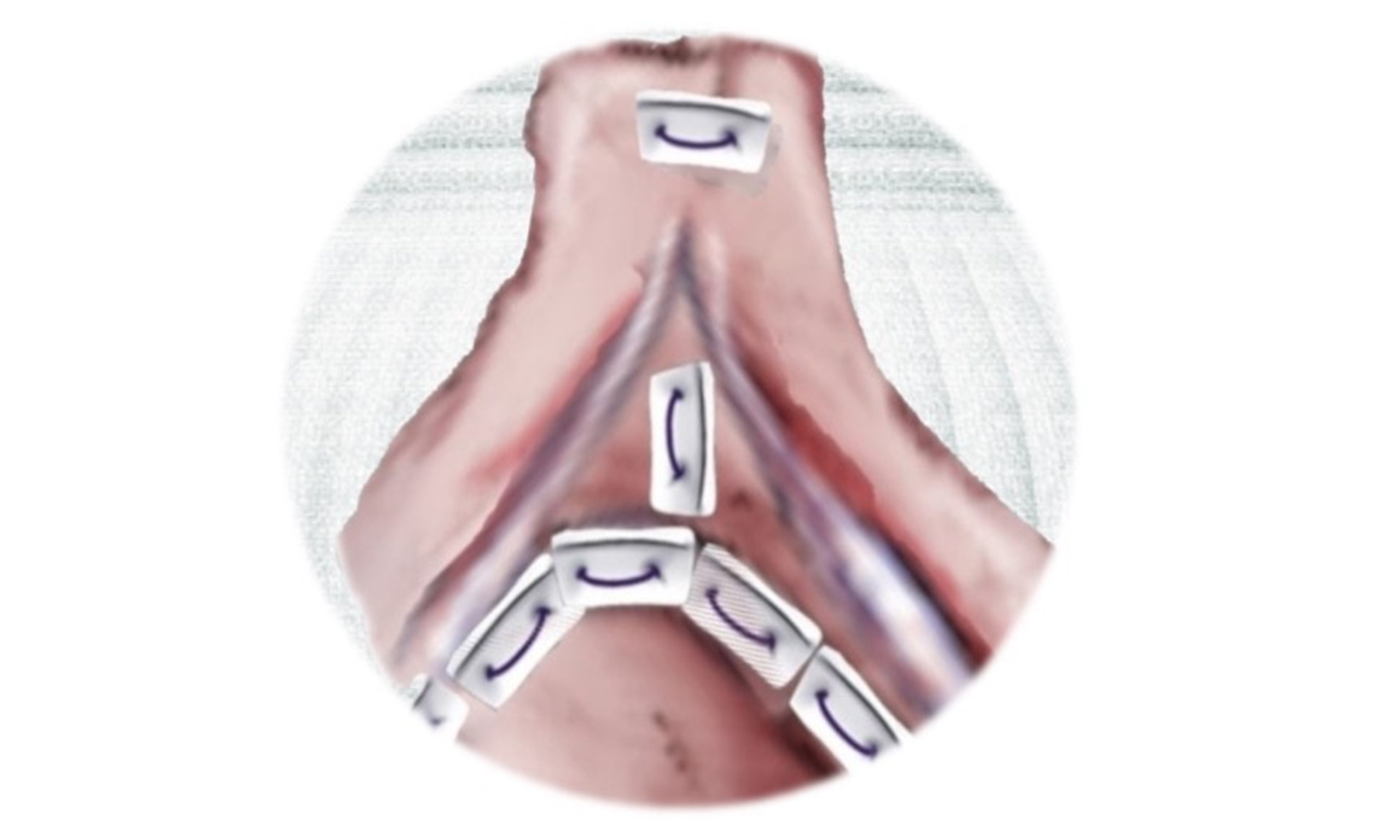
Figure 2. Simplified reimplantation in a bicuspid aortic valve. Observe the horizontal pledgeted suture securing the top of the commissure at the neo-sinutubular junction, and a single vertical pledgeted suture placed inside the interleaflet triangles to better support the commissure and seal the space behind it, thereby preventing blood flow between the commissure and the Dacron graft in closed (A) and open (B) position.
The aim of this commentary is to describe the simplified reimplantation technique, evaluate its advantages over the Modine modification, and define its appropriate indications.
THE SIMPLIFIED REIMPLANTATION
Following deep external root dissection, the arterial portion of the aortic wall forming the sinuses of Valsalva is completely excised, and the coronary buttons are prepared. Twelve pledgeted sutures are placed closely and circumferentially along the muscular myocardium and the fibrotic connective tissue that constitute the VBR, then passed through the designated level of the Valsalva graft. This proximal suture line serves as the hemostatic suture. In standard reimplantation, 3 to 5 mm of the aortic wall is typically preserved and sutured to the Dacron graft to achieve hemostasis. However, in the simplified approach, this step is no longer necessary, and the remaining aortic wall can be entirely removed. The graft is parachuted into place, and the commissures are elevated and secured at the new STJ using a single horizontal pledgeted suture at the top of each commissure. One or two pledgeted vertical sutures (depending on commissural height) are then placed within each interleaflet triangle. These sutures draw the Dacron graft toward the commissures and prevent blood leakage between the commissure and the graft [Figure 2]. The space behind the commissures and the Dacron is carefully probed, and if not fully sealed, an additional vertical suture is placed. Finally, leaflet coaptation is assessed using a caliper, and any prolapse is corrected with leaflet plication. The coronary buttons are then reimplanted, and the distal anastomosis is completed.
DISCUSSION
Valve-sparing root replacement (VSRR) techniques are the gold standard for preserving the AV in cases of aortic root pathology. Among these, the standard reimplantation technique is the most widely adopted, with excellent long-term outcomes[8].
Several minor modifications to the original reimplantation technique have been introduced to simplify the procedure. These variations share the common goal of restoring normal aortic annulus function[9] by stabilizing the VBR and re-establishing the appropriate STJ/VBR ratio. Both the Modine modification and the simplified reimplantation technique adhere to these principles. However, the Modine modification results in a less physiologic reconstruction of the root [Figure 1], due to the presence of blood flow between the commissures and the Dacron graft, as well as the concentration of stress at the commissures[10]. These factors may increase the risk of commissural detachment. Additionally, the blood flow between the graft and commissures leads to the formation of a single, spherical sinus rather than three distinct sinuses [Figure 1]. Preserving three independent sinuses in VSRR is desirable, as this anatomical configuration may enhance the motion and durability of the AV leaflets. With these considerations in mind, we improved the technique to ensure more complete attachment of the commissures to the Valsalva graft. This was achieved by placing one or two pledgeted vertical sutures (depending on the height of each commissure) within the interleaflet triangles. These sutures draw the Dacron graft toward the commissures and prevent blood flow between them [Figures 1 and 2]. Postoperative contrast-enhanced computed tomography (CT) was systematically performed prior to hospital discharge in all patients undergoing the simplified reimplantation. As summarized in Figure 1, these scans confirmed the absence of blood flow behind the commissures in both the simplified and standard reimplantation techniques. In axial views, the characteristic cloverleaf shape of the aortic root was successfully restored in both techniques. In contrast, the Modine modification demonstrated persistent contrast behind the commissures, preventing cloverleaf reconstruction of the root.
The potential advantages of alternative reimplantation techniques over the standard approach require further clarification. We used the simplified reimplantation as a bailout option in cases where the standard technique was considered particularly challenging. A common feature in these cases was the presence of extremely fragile aortic wall remnants, which were often associated with severe aortic pathology [Figure 3]. Examples include root aneurysms due to filamin-A deficiency, neo-aortic root aneurysm following an arterial switch operation, markedly dilated bicuspid aortic valves with “sinking sinuses”[11], localized intimal rupture, and aortic wall perforation extending into the leaflet hinge. In such cases, the aortic remnants were deemed unsuitable for secure suturing to the Dacron graft and unlikely to ensure hemostasis. The simplified reimplantation technique offers the advantage of allowing for complete excision of these fragile remnants while enabling strong and continuous attachment of the commissures to the Valsalva graft. This approach may expand the indications for valve-sparing procedures.
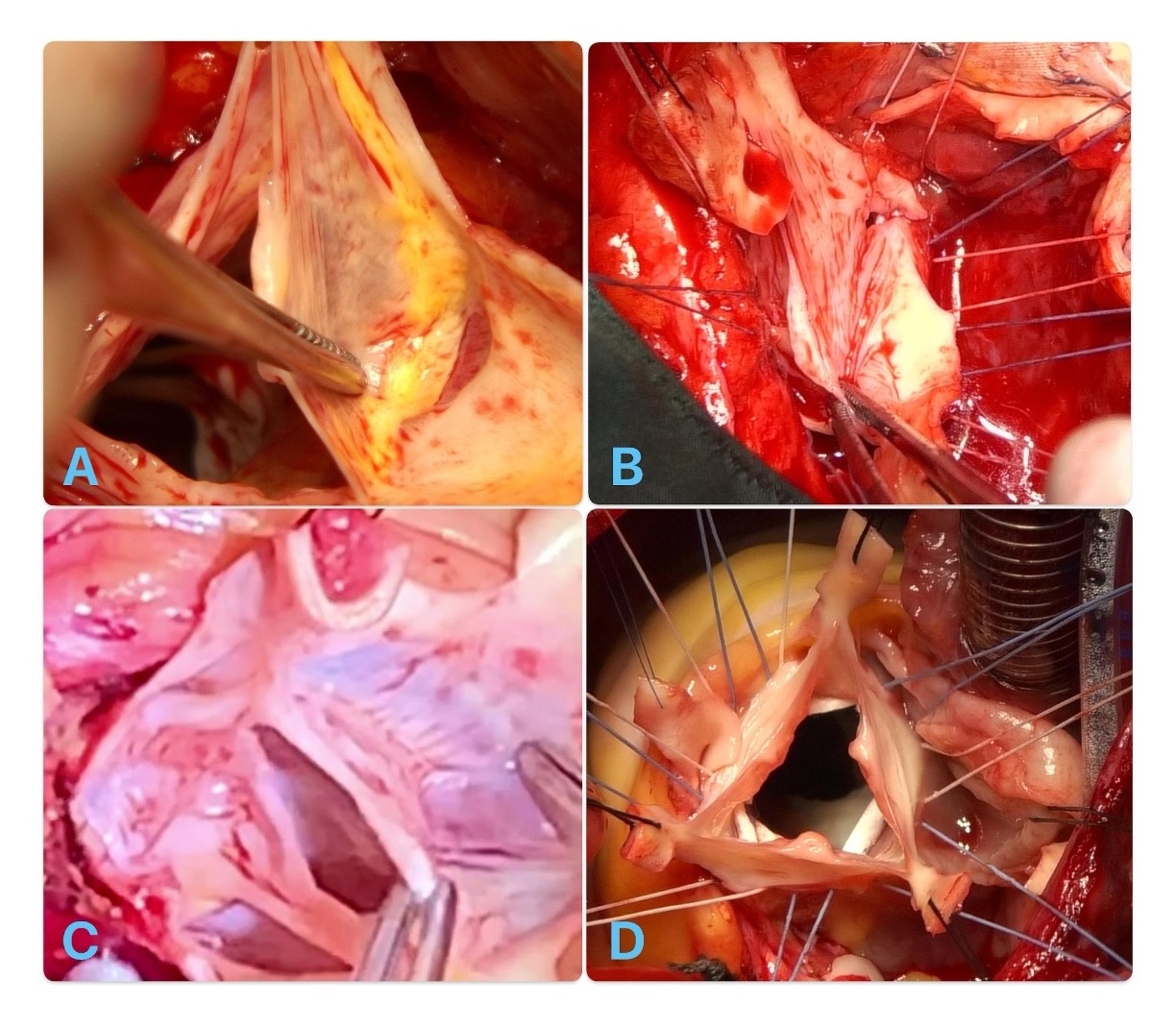
Figure 3. Examples of fragile aortic wall remnants: (A) Localized intimal rupture of the aortic wall remnant. (B) Small perforation of the aortic wall extending into the leaflet hinge at the non-coronary sinus. (C) Significant muscular inclusion at the right–non-coronary sinus (“sinking sinus”) with a translucent aortic wall firmly adhered. (D) Large root aneurysm associated with filamin-A deficiency.
CONCLUSION
Standard reimplantation remains the benchmark technique for preserving the AV in cases of root pathology. However, certain cases involving extremely fragile, diseased, or damaged aortic wall remnants may pose significant challenges to this approach or necessitate composite root replacement. This simplified reimplantation technique represents a promising alternative in such cases. In a small, carefully selected cohort, this modified approach was feasible, safe, and associated with favorable short-term outcomes.
DECLARATIONS
Authors’ contributions
Made substantial contributions to the conception and design of the study and performed data analysis and interpretation: Folino G, Torre M, De Paulis R
Availability of data and materials
Data are not publicly available due to the nature (commentary) of the current issue. The data supporting this study are available from the corresponding author upon reasonable request.
Financial support and sponsorship
None.
Conflicts of interest
De Paulis R is the Guest Editor of the Special Issue “Innovations in Aortic Surgery and Valve Repair”. De Paulis R was not involved in any steps of the editorial processing, notably including reviewer selection, manuscript handling, or decision making, while the other authors have declared that they have no conflicts of interest.
Ethical approval and consent to participate
This study was conducted in accordance with the Declaration of Helsinki. Ethical approval was waived due to its retrospective design.
Consent for publication
Patient consent was waived due to the retrospective nature of the study and the anonymization of personal information and data.
Copyright
© The Author(s) 2025.
REFERENCES
1. David TE, Feindel CM. An aortic valve-sparing operation for patients with aortic incompetence and aneurysm of the ascending aorta. J Thorac Cardiovasc Surg. 1992;103:617-21; discussion 622.
2. De Paulis R, De Matteis GM, Nardi P, Scaffa R, Colella DF, Chiarello L. A new aortic Dacron conduit for surgical treatment of aortic root pathology. Ital Heart J. 2000;1:457-63.
3. Ikonomidis JS. Valve-sparing aortic root replacement - “T. David V” method. Oper Tech Thorac Cardiovasc Surg. 2009;14:281-96.
4. Jahanyar J, de Kerchove L, Arabkhani B, et al. Three decades of reimplantation of the aortic valve-the Brussels experience. Ann Cardiothorac Surg. 2023;12:244-52.
5. El Arid JM, Azzaoui R, Koussa M, Modine T. Technique to facilitate the native valve reimplantation during the david procedure. J Card Surg. 2014;29:485-6.
6. Modine T, Piperata A, Coisne A, et al. Preliminary results of a simplified aortic valve-sparing technique: a feasibility study. J Card Surg. 2022;37:2564-70.
7. Folino G, Salica A, Torre M, et al. Simplified reimplantation: a bailout in fragile aortic wall remnants. JTCVS Tech. 2025;30:52-4.
8. Chirichilli I, Scaffa R, Irace FG, et al. Twenty-year experience of aortic valve reimplantation using the Valsalva graft. Eur J Cardiothorac Surg. 2023;63:ezac591.
9. El Khoury G, Glineur D, Rubay J, et al. Functional classification of aortic root/valve abnormalities and their correlation with etiologies and surgical procedures. Curr Opin Cardiol. 2005;20:115-21.
10. Stanová V, Rieu R, Thollon L, et al. Leaflet mechanical stress in different designs and generations of transcatheter aortic valves: an in vitro study. Struct Heart. 2024;8:100262.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Special Issue
Copyright

Data & Comments
Data
0










Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].