


Yttrium-90 combination therapies in hepatocellular carcinoma: current evidence and future directions
 0
0 Abstract
Yttrium-90 (Y-90) radioembolization, via endovascular delivery of high-dose beta radiation microspheres to tumors, is an invaluable locoregional therapy for hepatocellular carcinoma (HCC). Y-90’s limited off-target radiation exposure enables excellent tumor control with a favorable safety profile. Recent developments suggest that combining targeted radioembolization with systemic treatments, such as molecularly targeted therapies and immune checkpoint inhibitors (ICIs), may offer additive or even synergistic benefits, thereby enhancing both local tumor response and immune activation. This review explores the mechanistic rationale, clinical evidence, and therapeutic strategies involving Y-90 combination therapies in HCC. Data from phase I, II, and III trials suggest improved outcomes with Y-90 plus ICI combination therapy compared with monotherapy. By contrast, trials comparing Y-90 and multi-kinase combination inhibitors with monotherapy have yielded mixed results, highlighting the importance of continued research. Challenges remain in patient selection, optimal sequencing, and toxicity management. To date, no randomized clinical trials have directly compared Y-90 alone with Y-90-based combination therapy, but ongoing trials aim to clarify the role of Y-90 in the evolving systemic treatment landscape. This review highlights the potential of Y-90 combination therapies to enhance the multidisciplinary management of HCC and underscores future research priorities to optimize outcomes.
Keywords
INTRODUCTION
Hepatocellular carcinoma (HCC) is the most common primary liver malignancy and the third leading cause of cancer-related death worldwide[1]. Treatment options depend on tumor stage and liver function, with curative therapies such as ablation, resection, and transplantation typically limited to early-stage disease. Despite improvements in surveillance, many patients present with intermediate or advanced disease and are therefore excluded from traditionally curative options[2,3]. For these patients, locoregional therapies, including transarterial chemoembolization (TACE) and selective internal radiation therapy (SIRT) with yttrium-90 (Y-90) microspheres, are often used to control tumor burden[4,5,6]. In parallel, systemic therapies, including multi-kinase inhibitors such as sorafenib and lenvatinib, and immune checkpoint inhibitors (ICIs) combined with anti-angiogenic monoclonal antibodies, such as atezolizumab plus bevacizumab, have reshaped the therapeutic landscape[7,8,9].
The Barcelona Clinic Liver Cancer (BCLC) prognosis and treatment strategy has long been at the forefront of guiding decision-making in HCC management[10]. The five stages within the BCLC strategy are determined by considering tumor burden, performance status, and liver function. In the 2020 BCLC update, clinicians are provided with greater management flexibility, reflecting advances in HCC treatment strategies.
In addition to transplantation, surgical resection and ablation remain the primary curative treatments for very early- to early-stage HCC; however, the latest BCLC guidelines include Y-90 radioembolization as an appropriate treatment modality for patients with very early- to early-stage disease. In intermediate-stage disease, locoregional treatments including Y-90 therapy can downstage tumors and make patients eligible for transplantation. Beyond its antitumor effects, lobar Y-90 administration can promote contralateral hepatic lobe hypertrophy, thereby facilitating surgical resection in cases where primary resection is not safe or feasible. While portal vein ligation or embolization has traditionally been used to induce preoperative future liver remnant hypertrophy, studies show that lobar Y-90 can achieve comparable results, providing both direct therapeutic benefit and optimization of surgical candidacy[11].
Y-90 radioembolization delivers targeted internal radiation to tumors while minimizing harm to non-tumorous tissue. When paired with systemic therapies, it offers the potential to combine precise local tumor destruction with broader systemic disease control. This review aims to provide a comprehensive overview of Y-90 combination therapies in HCC, focusing on mechanistic rationale, clinical outcomes, safety considerations, and future directions to optimize patient outcomes.
MECHANISTIC RATIONALE FOR Y-90 COMBINATION THERAPIES
Y-90 radioembolization: principles and effects
Y-90 is a high-energy beta-emitting radionuclide with beta particles that penetrate tissue to an average depth of about 2.5 mm, allowing for targeted radiation delivery within the tumor while sparing adjacent tissues[6,12,13]. The microspheres, available as either glass or resin formulations with distinct physical and dosimetric properties (see Table 1), are selectively delivered into hepatic artery branches feeding the tumor, exploiting preferential arterial blood supply to HCC compared to the portal venous supply of normal liver parenchyma[14].
Comparison of commercially available yttrium-90 microsphere products
| Glass microspheres (TheraSphereTM) | Resin microspheres (SIR-Spheres®) | |
| Manufacturer | Boston Scientific, Marlborough, MA | Sirtex Medical Inc., Wilmington, MA |
| Microsphere size | 20-30 μm | 22-42 μm |
| Isotope incorporation | Y-90 integrated within a glass matrix | Y-90 on resin surface |
| Specific gravity | High | Low |
| activity per sphere at calibration | 2,500 Bq | 50 Bq |
| Activity per sphere at treatment | 100-1500 Bq | 52-148 Bq |
| Time of calibration | Prior to treatment | Day of treatment or up to 3 days after |
| Number of spheres per 3 GBq | 1.2 million | 44 ± 2.6 million |
| Mean tumor-absorbed dose | 197-794 Gy (varies by technique) | 73-308 Gy (varies by technique) |
| Tumoricidal dose for HCC | 205 Gy | 100-120 Gy |
| Clinical advantages | Fewer particles reduce embolic effects; suitable for portal vein invasion and radiation segmentectomy | Better distribution in larger tumors with high arterial flow |
| Gastrointestinal toxicity risk | Lower risk of GI tract injury | Higher risk of GI ulceration due to more particles |
| Radiation pneumonitis threshold | Higher dose tolerance (~ 41 Gy) | Lower dose tolerance (~ 21 Gy) |
There are currently two commercially available Y-90 microsphere products in clinical use worldwide: TheraSphere™ (glass microspheres) manufactured by Boston Scientific (Marlborough, MA) and SIR-Spheres® (resin microspheres) manufactured by Sirtex Medical Inc. (Wilmington, MA)[15]. These products differ substantially in their physical and radiobiological characteristics, which influence their clinical applications and dosimetric properties.
Glass microspheres (TheraSphere™) have Y-90 integrated within the glass matrix, with a higher specific gravity and significantly higher activity per sphere (2500 Bq at calibration, 100-1500 Bq at treatment). Due to the higher activity per particle, fewer microspheres are required to deliver a given radiation dose (approximately 1.2 million spheres per 3 GBq), which may reduce embolic effects. Glass microspheres are calibrated prior to treatment and are available in 3-20 GBq vials. TheraSphere™ has received regulatory approval in the United States, the European Union, and other major markets for the treatment of HCC[15].
Resin microspheres (SIR-Spheres®) have Y-90 bound to the resin surface, with lower specific gravity and lower activity per sphere (50 Bq at calibration, 52-148 Bq at treatment). Because of the lower activity per particle, more microspheres are needed to deliver equivalent radiation doses (approximately 44 ± 2.6 million spheres per 3 GBq vial), which may provide better distribution in larger tumors with high arterial flow. Resin microspheres are calibrated on the day of treatment or up to three days afterward and are available in 3 GBq vials. SIR-Spheres® has received regulatory approval in multiple jurisdictions worldwide, initially for colorectal liver metastases and subsequently for HCC in many regions[15].
The choice between glass and resin microspheres depends on multiple factors, including tumor characteristics, vascular anatomy, and treatment goals. Glass microspheres may be more suitable when early stasis or reflux is a concern, in the setting of portal vein invasion, and for radiation segmentectomy, because fewer particles are required[16]. Resin microspheres may be preferable for larger tumors and those with high arterial flow[16]. Studies comparing the two products have shown different dosimetric profiles, with glass microspheres typically delivering higher tumor-absorbed doses [mean, 197 gray (Gy) vs. 73 Gy for resin], though clinical outcomes in terms of tumor response and toxicity appear similar when appropriately dosed[17,18].
An emerging alternative product is Holmium-166 (Ho-166) poly(L-lactic acid) microspheres, which is approved in the European Union and under regulatory review in other jurisdictions[19]. This product offers the advantage of direct visualization on single-photon emission computed tomography/computed tomography (SPECT/CT) imaging due to Ho-166’s gamma-emission properties, potentially allowing for more precise dosimetry and treatment planning.
Once administered, the microspheres become lodged within the tumor microvasculature to deliver localized radiation doses that induce direct cytotoxic effects, primarily through the induction of double-stranded DNA breaks[23,24]. This DNA damage triggers apoptosis and mitotic catastrophe in malignant cells, effectively reducing tumor burden. The localized nature of this therapy allows for high radiation doses to be safely administered to patients with limited treatment options or who are not candidates for surgery or systemic therapies.
However, Y-90 microsphere beads exhibit heterogeneous distribution throughout the tumor microenvironment, likely owing to heterogeneous tumor perfusion[25]. This results in a heterogeneous beta-particle distribution, therefore, heterogeneous cytotoxic effects, especially in larger tumors. This effect may be further confounded with anti-vascular endothelial growth factor (anti-VEGF) agents such as sorafenib and lenvatinib, potentially leading to even more heterogeneous microsphere distribution. This mechanism may explain the dose-dependent response observed in the DOSISPHERE-1 study, in which overall survival (OS) was higher in the group treated with higher doses, overcoming this heterogeneity[26]. After combination therapy with Y-90, it is possible that untreated tumoral cells could then be targeted with other systemic therapies, such as ICIs, through immune-mediated pathways described below.
Beyond direct cytotoxicity, Y-90 radioembolization exerts significant effects on tumor vasculature. Radiation-induced endothelial injury leads to disruption of the tumor’s abnormal and fragile vasculature, resulting in ischemia and secondary tumor cell death[27]. This vascular insult not only deprives the tumor of oxygen and nutrients but also alters the tumor microenvironment in ways that may modulate therapeutic response.
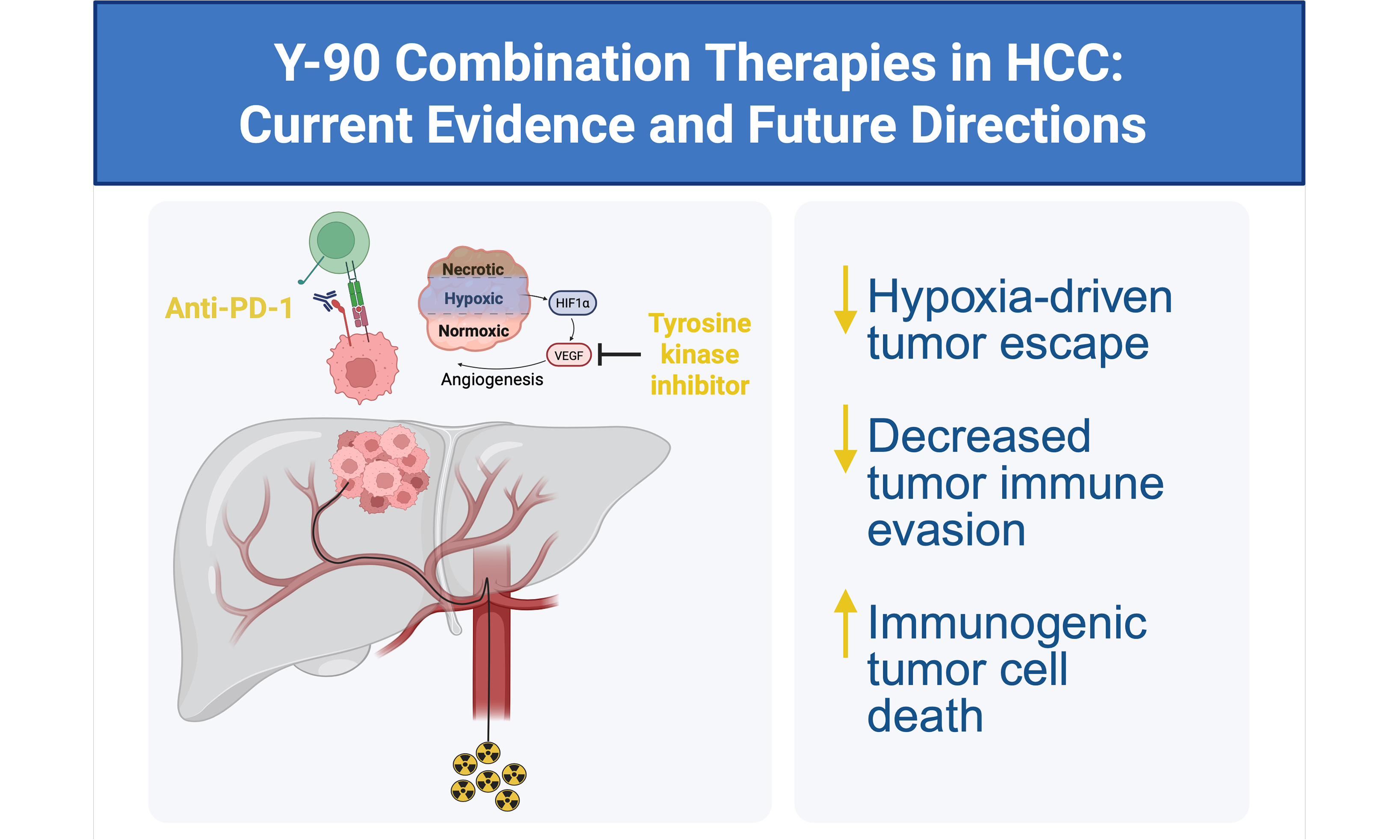
Recent studies have demonstrated that Y-90 treatment can provoke immunomodulatory effects within the tumor microenvironment. Radiation can enhance immune-cell infiltration, including cytotoxic T lymphocytes (CTLs) and antigen-presenting cells (APCs), potentially transforming an immunologically “cold” tumor into a more inflamed and “hot” tumor[28]. Additionally, radiation therapy (RT) enhances antitumor immunity by releasing damage-associated molecular patterns (DAMPs), which stimulate type I interferons (IFN-α and IFN-β) and activate immune responses. RT also remodels tumor vasculature and the tumor microenvironment, improving immune-cell infiltration. By upregulating IFN-γ and major histocompatibility complex (MHC) expression, RT further activates lymphocytes and increases immune-cell access to the tumor. The rise in IFN-γ can also reduce tumor resistance to anti-programmed death-1 (anti-PD-1) therapy [Figure 1][29,30].
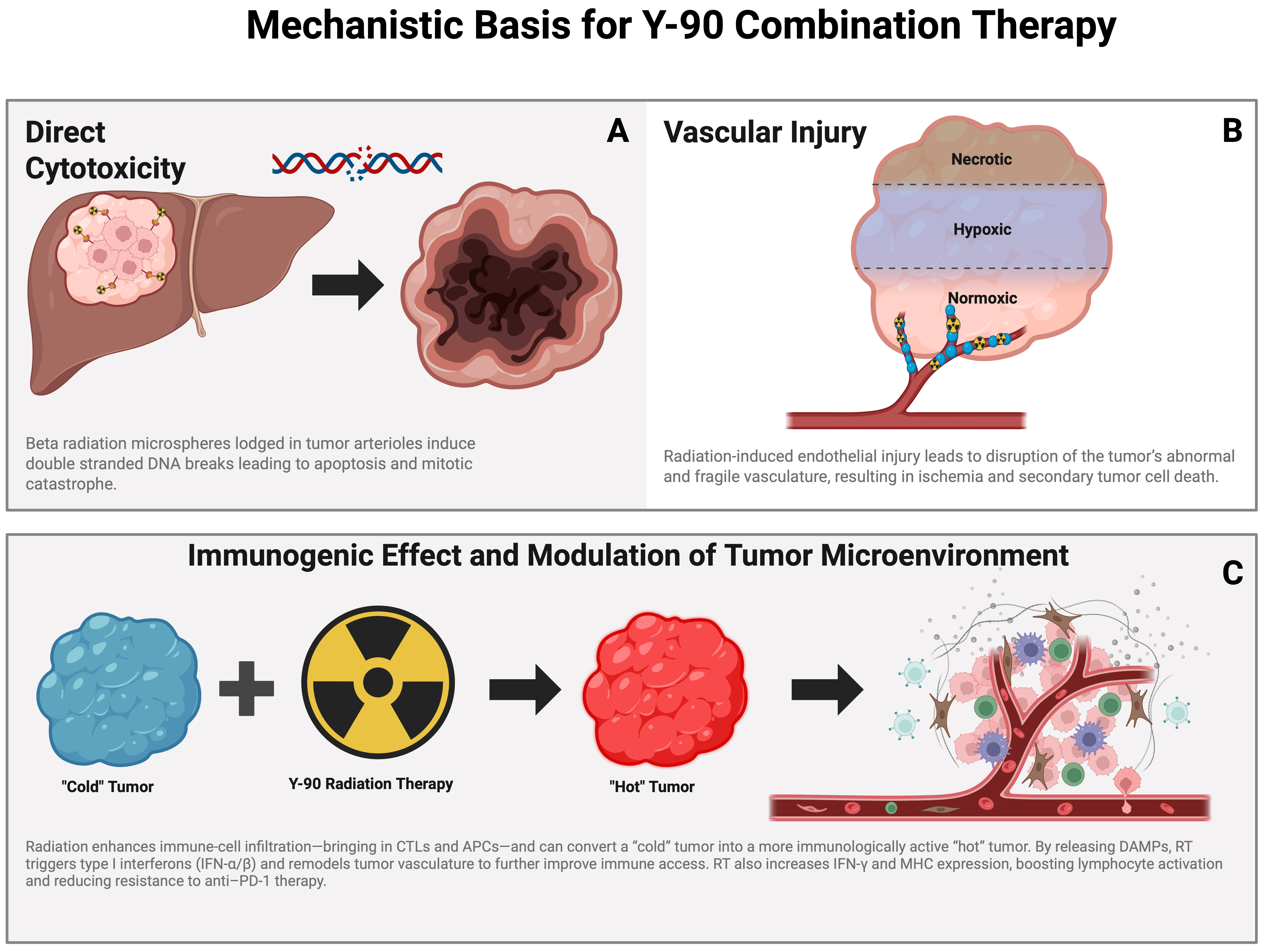
Figure 1. Schematic illustration demonstrating the multifactorial mechanisms of action of Y-90 radioembolization. (A) Direct cytotoxicity: Intra-arterially delivered Y-90-labeled microspheres preferentially lodge within tumor arterioles, emitting β-radiation that induces double-stranded DNA breaks, leading to apoptosis and mitotic catastrophe; (B) Vascular injury: Radiation-induced endothelial damage disrupts the tumor’s fragile neovasculature, resulting in ischemia, hypoxia, and progressive tumor necrosis; (C) Immunogenic modulation of the tumor microenvironment: Y-90 radiation promotes immunogenic cell death, release of DAMPs, and upregulation of interferon signaling and antigen presentation, facilitating immune cell infiltration and conversion of immunologically “cold” tumors into “hot” tumors. These effects provide a biologic rationale for combining Y-90 radioembolization with systemic therapies, including immune checkpoint inhibitors. Created in BioRender. D, M. (2026) https://BioRender.com/37vhiax CTL: Cytotoxic T lymphocyte; APC: antigen-presenting cell; DAMP: damage-associated molecular pattern; RT: radiation therapy; IFN: interferon; MHC: major histocompatibility complex.
These immune-related changes provide the basis for combining Y-90 radioembolization with immunotherapies, aiming to amplify durable antitumor immunity. The effects of Y-90 radioembolization are multifaceted; they encompass direct tumor cell cytotoxicity, vascular disruption, and immune microenvironment modulation. Collectively, these effects provide a strong mechanistic rationale for integrating Y-90 with systemic therapies. Understanding these mechanisms is critical for optimizing combination regimens designed to maximize therapeutic efficacy and overcome resistance in HCC.
Synergy with systemic agents
Targeted agents
Targeted agents, such as sorafenib and lenvatinib, exert their antitumor effects through inhibition of multiple tyrosine kinase receptors, most notably vascular endothelial growth factor receptors (VEGFRs) and platelet-derived growth factor receptors (PDGFRs), which play central roles in tumor angiogenesis, endothelial cell survival, and tumor cell proliferation[9]. By interrupting these signaling pathways, targeted therapies impair the tumor’s ability to establish and maintain a functional vascular network, thereby limiting oxygen and nutrient delivery and suppressing tumor growth. In HCC, where tumor progression is highly dependent on aberrant angiogenesis, blockade of these pathways has proven particularly relevant.
Y-90 radioembolization further exploits this vascular dependence by delivering high-dose, localized radiation to the tumor microenvironment. Radiation-induced endothelial injury leads to microvascular thrombosis, vessel collapse, and regional ischemia, resulting in substantial tumor necrosis. However, this vascular disruption also creates a hypoxic microenvironment that activates hypoxia-inducible factors (HIFs), which in turn drive compensatory upregulation of pro-angiogenic mediators, most prominently vascular endothelial growth factor (VEGF)[11]. This adaptive response promotes neovascularization, restoring blood flow to residual tumor cells and enabling regrowth. Such angiogenic rebound has historically limited the durability of tumor control following radiation-based therapies alone and represents a key mechanism of therapeutic resistance.
Combining Y-90 radioembolization with anti-angiogenic targeted agents may offer a biologically rational strategy to counteract this process. While Y-90 induces direct cytotoxicity and vascular destruction, concurrent or sequential inhibition of VEGFR and PDGFR would theoretically blunt the hypoxia-driven surge in angiogenic signaling, effectively suppressing rebound neovascularization. By preventing reconstitution of the tumor vasculature, targeted agents may prolong the ischemic and cytotoxic effects of radiation, thereby enhancing local tumor control. Systemic inhibition of angiogenic and proliferative pathways may also limit the growth of microscopic residual disease and distant metastases, further extending the therapeutic benefit beyond the treated hepatic territory.
This complementary interaction positions anti-angiogenic therapy as a critical modulator of radiation-induced tumor adaptation and may produce more durable disease control and improved clinical outcomes in patients with HCC.
Immune checkpoint inhibitors
ICIs targeting programmed death-1 (PD-1), programmed death-ligand 1 (PD-L1), and cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) have revolutionized cancer therapy by restoring T-cell-mediated tumor killing[12]. These agents essentially release the brakes on the immune system, allowing cytotoxic T-cells to recognize and eliminate tumor cells more effectively. Importantly, radiation delivered by Y-90 induces immunogenic cell death, characterized by the release of tumor-associated neoantigens. These neoantigens activate dendritic cells, which then prime and expand cytotoxic T-cell populations, effectively “vaccinating” the immune system against the tumor[14]. This process can convert immunologically “cold” tumors, which are typically resistant to immunotherapy due to a lack of immune infiltration, into “hot” tumors that are more responsive to ICIs.
The integration of Y-90 radioembolization with ICIs has the potential to produce synergistic antitumor immunity. Radiation-induced immunogenic cell death enhances tumor antigen presentation and T-cell activation, while ICIs sustain and amplify the immune response by preventing T-cell exhaustion and inhibition. This combined approach may yield more durable clinical responses and improve long-term survival outcomes compared to either modality alone.
CLINICAL EVIDENCE OF Y-90 COMBINATION THERAPIES
Y-90 plus targeted therapy
The combination of Y-90 radioembolization with systemic targeted therapies has been investigated in patients with HCC and demonstrated promising, yet nuanced clinical outcomes.
Phase II/III trials comparing therapies
The Sorafenib in Advanced Hepatocellular Carcinoma (SORAMIC) trial is a multicenter randomized, open-label phase II trial that compared survival in patients with advanced HCC treated with sorafenib alone to those treated with Y-90 in addition to sorafenib. According to the most recent BCLC staging and treatment strategy guidelines, sorafenib is a first-line systemic treatment alternative for advanced-stage HCC when atezolizumab-bevacizumab or durvalumab-tremelimumab are not feasible[10]. The study found no significant improvement in OS with the addition of Y-90 to sorafenib therapy. Specific subgroup analyses within this trial, however, did demonstrate statistically significant survival benefits with the addition of Y-90 to sorafenib therapy. For example, survival benefits were observed in patients without cirrhosis [Hazard ratio (HR), 0.46; 0.25-0.86; P = 0.02], in patients with cirrhosis of non-alcoholic etiology (HR 0.63; P = 0.012), and in patients aged 65 years or younger (HR 0.65; P = 0.05)[31].
An important consideration is that this landmark trial compared combination therapy with targeted monotherapy, rather than addressing this review’s focus on how combination therapy may be superior to SIRT monotherapy. Moreover, a post-hoc analysis of the SORAMIC trial assessed the follow-up images of 177 patients by mRECIST (modified Response Evaluation Criteria in Solid Tumors) and demonstrated a significantly increased objective response rate (ORR), complete response rate, and disease control rate among patients treated with combination therapy[32].
The SARAH (Efficacy and safety of selective internal radiotherapy with yttrium-90 resin microspheres compared with sorafenib in locally advanced and inoperable hepatocellular carcinoma) trial, a pivotal phase III randomized controlled study, compared Y-90 radioembolization with oral multi-kinase inhibitor sorafenib monotherapy in patients with advanced HCC[7]. Although the trial did not demonstrate a statistically significant superiority of Y-90 over sorafenib for overall survival (OS), subgroup analyses suggested potential benefits in select patient populations - particularly those with preserved liver function and limited tumor burden. This trial highlighted the importance of careful patient stratification when considering combination therapies.
The Selective Internal Radiation Therapy Versus Sorafenib in Asia-Pacific Patients with HCC (SIRveNIB) trial, a phase III randomized trial, also compared OS between patients with advanced HCC managed with Y-90 versus sorafenib[33]. Again, no significant difference in OS was found, but Y-90 radioembolization demonstrated a superior toxicity profile to sorafenib. These trials underscore the need for additional studies to identify cohorts most likely to benefit from Y-90-based combination strategies.
Retrospective and prospective clinical studies
Several retrospective studies have provided encouraging evidence supporting the additive effects of combining Y-90 with ICIs. Notably, Lee et al. reported results from a 2023 phase I/II trial investigating the efficacy and safety of Y-90 radioembolization combined with durvalumab in patients with unresectable HCC[8]. This study demonstrated a median progression-free survival (PFS) of 6.9 months and an ORR of 83.3%, outcomes that compare favorably to Y-90 monotherapy (PFS, 3 months; ORR, 42-57%). Importantly, the combination exhibited a tolerable safety profile, with common adverse events including fatigue, hypertension, and transient liver enzyme elevations, all manageable with dose modifications and supportive care[27].
Another study evaluating the combination of Y-90 with targeted agents demonstrated comparable survival outcomes between groups and confirmed an acceptable safety profile. Facciorusso et al. conducted a retrospective propensity score-matched study of 135 patients with intermediate-to-advanced HCC. Outcomes between Y-90 plus sorafenib and Y-90 alone were compared[34]. The combination group showed no significant difference in median overall survival (mOS) (10 vs. 10 months; P = 0.711) or PFS (6 vs. 7 months; P = 0.992). Importantly, adverse events were manageable, and no unexpected toxicities were identified[34].
Mechanistic and clinical implications
The rationale for combining Y-90 with targeted therapies centers on disrupting tumor vasculature and cellular proliferation through complementary mechanisms. While Y-90 induces localized radiation damage and vascular disruption, targeted agents inhibit signaling pathways such as VEGFR and PDGFR, mitigating angiogenic rebound and systemic tumor growth. Clinical data to date support the hypothesis that this dual approach may lead to improved local control, delayed disease progression, and potentially enhanced overall survival in carefully selected patients[7,9,11].
Y-90 plus immune checkpoint inhibitors
Emerging clinical evidence increasingly supports the strategic combination of Y-90 radioembolization with ICIs to harness the synergistic potential of radiation-induced immunomodulation and immune checkpoint blockade. This approach leverages the localized cytotoxic effects of Y-90 to promote immunogenic cell death and neoantigen release, thereby priming the tumor microenvironment to respond more effectively to ICIs.
IMbrave050 exploratory arm
The phase III IMbrave050 trial was designed to evaluate adjuvant atezolizumab plus bevacizumab after curative resection or ablation[35,36]. An exploratory arm included patients treated with Y-90 before systemic therapy. Preliminary analyses of the Y-90 subgroup showed improved recurrence-free survival compared with historical controls, with no unexpected toxicities.
Early-phase trials and case series
Phase I and II studies and retrospective series of Y-90 combined with PD-1/PD-L1 blockade (nivolumab, pembrolizumab, atezolizumab) have reported ORRs of 30%-50% and mOS approaching 20 months, exceeding outcomes typically observed with monotherapy. Safety signals were consistent with established ICI profiles, without evidence of enhanced toxicity. For example, the combination of Y-90 and nivolumab in NCT02837029 was tolerable and achieved a clinical benefit rate of 82%, including nine out of eleven patients with stable disease. Key characteristics and outcomes of key clinical trials are summarized in Table 2[8,37,38,39].
Key clinical studies evaluating Y-90 radioembolization combined with immune checkpoint inhibitors in hepatocellular carcinoma
| Trial ID(Year) | Study Phase | Population | n | Design | Intervention | Primary endpoint | Findings |
| NCT03099564(2021) | I | Age ≥ 18 years and HCC with CP ≤ B7 and ECOG ≤ 1 | 27 | Prospective Single-arm | Y-90 + Pembrolizumab | PFS6 by RECIST | PFS6 of 55.6% (95% CI, 35.3-74.5) and OS of 27.30 months (95% CI, 10.15-39.52) |
| NCT03033446(2021) | II | Age ≥ 21 years and HCC with CP A and lesion > 20 mm | 40 | Prospective Single-arm | Y-90 + Nivolumab | ORR by RECIST | ORR of 30.6% (95% CI, 16.4-48.1)Most common AE: dermatologic |
| NCT02837029(2021) | I | Age ≥ 18 years and HCC with CP ≤ B8 | 27 | Prospective Single-arm | Y-90 + Nivolumab | Nivolumab MTD with Y-90 | Combination therapy was tolerable with MTD established and a CBR of 82% |
| NCT04124991 (2022) | I/II | Age ≥ 19 years and HCC with CP ≤ B7 | 24 | Prospective Single-arm | Y-90 + Durvalumab | TTP by mRECIST | Median TTP 15.2 months (95% CI, 6.1-not estimated) 2 (8.7%) grade 3 AE, no grade 4 |
Ongoing trials
Several prospective studies are in progress. NCT07059494 (phase IV) is evaluating Y-90 with atezolizumab plus bevacizumab in advanced HCC, with PFS and immune correlates as primary endpoints. Additional phase II trials (NCT05809869 and NCT06867432) are assessing Y-90-ICI combinations in advanced and unresectable disease [Table 3][40-42].
Ongoing Y-90 combination therapy trials
| Trial ID | Study phase | Population | Design | Intervention | Primary endpoint(s) | Status |
| NCT07059494 | IV | Age ≥ 18 years and HCC within MC OR HCC beyond MC | Parallel assignment | Y-90 + Atezolizumab + Bevacizumab | Within MC: RRT defined by CT/MRI and decrease in AFP by ≥ 50%ORBeyond MC: Rate of radiographic downstaging to within MC | Recruiting |
| NCT06867432 | II | Age 18-74 years and unresectable HCC | Single-arm | Y-90 + HAIC + Atezolizumab + Bevacizumab | ORR by mRECIST | Not yet recruiting |
| NCT05809869 | II | Age ≥18 years and HCC | Single-arm | Y-90 + Tremelimumab + Durvalumab | Best objective responseandobjective response rate | Recruiting |
Toxicity and safety profile
The combination of Y-90 radioembolization with systemic therapies generally demonstrates an acceptable and manageable safety profile, though careful attention to potential toxicities remains essential.
Hepatic toxicity
Transient elevations in liver enzymes such as alanine aminotransferase (ALT) and aspartate aminotransferase (AST) are common following Y-90 treatment due to localized radiation-induced hepatocyte injury and inflammation[43]. These enzyme elevations are typically self-resolving and peak within weeks of Y-90 treatment. Severe hepatic toxicity, including radiation-induced liver disease (RILD) or liver failure, is rare when patients with preserved hepatic function, generally Child-Pugh class A or early B7, are selected[43,44]. Therefore, combining Y-90 with systemic therapies, some of which have hepatotoxic potential, necessitates close monitoring of hepatic function to detect early signs of hepatic decompensation and manage accordingly.
Systemic toxicity of targeted agents
Targeted therapies such as sorafenib and lenvatinib present predictable systemic toxicities. Fatigue is among the most common adverse effects reported, alongside hypertension and dermatologic toxicities, including palmar-plantar erythrodysesthesia[45]. These side effects are typically dose-dependent and manageable through supportive care, dose adjustments, and patient education. Current evidence indicates that the addition of Y-90 radioembolization does not exacerbate these systemic toxicities, supporting the safety of combined regimens with appropriate monitoring[46].
Immune-related adverse events (irAEs) from ICIs
ICIs can induce immune-related adverse events (irAEs) due to nonspecific immune activation, with manifestations such as immune-mediated hepatitis, colitis, pneumonitis, endocrinopathies, and dermatologic reactions[47]. While these events can be severe, timely recognition and immunosuppressive treatment are often effective. Data suggest that combining ICIs with Y-90 radioembolization does not significantly increase the frequency or severity of irAEs[48]. The localized nature of radiation and judicious patient selection may mitigate additive toxicity risks.
Patient selection and monitoring
Ensuring patient safety requires stringent selection criteria, favoring those with preserved liver function (Child-Pugh A or selected B7) and good performance status (Eastern Cooperative Oncology Group, ECOG 0-1)[44,45]. Baseline evaluation of liver reserve, portal hypertension, and bilirubin levels informs candidacy and risk stratification. Serial monitoring of liver enzymes, hematologic parameters, blood pressure, and symptoms after treatment facilitates early detection of toxicities and guides timely interventions such as dose modifications or supportive care. This degree of monitoring is facilitated by a multidisciplinary approach.
TREATMENT SEQUENCING AND OPTIMIZATION
Determining the optimal sequencing and timing of Y-90 radioembolization in combination with systemic therapies remains a critical and actively investigated area in HCC management. The complexity of tumor biology, patient heterogeneity, and treatment-related toxicities necessitates a strategic approach to maximize therapeutic benefit while minimizing adverse effects.
Sequential therapy
One approach is to use Y-90 radioembolization as the initial locoregional intervention, followed by systemic therapy. This sequence allows for significant tumor debulking through localized radiation, potentially reducing tumor burden and vascularity, which may subsequently enhance the efficacy of systemic agents. Clinical studies frequently initiate systemic therapy approximately 2 to 4 weeks after Y-90 treatment, a window that balances sufficient recovery from procedure-related toxicities and early intervention against micro-metastatic or residual disease[49,50]. This approach aims to exploit the distinct mechanisms of action sequentially: radiation to induce direct tumor cytotoxicity and vascular disruption, followed by systemic inhibition of tumor proliferation and metastasis.
Concurrent therapy
Synchronous administration of Y-90 and systemic agents represents an appealing strategy to maximize potential synergy. The rationale centers on the ability of concurrent systemic agents to augment radiation-induced effects, such as preventing angiogenic rebound and enhancing immune-mediated tumor cell killing. However, the concomitant use of these treatments may increase the risk and severity of toxicities, including liver dysfunction, fatigue, and irAEs. Existing data on concurrent administration are limited, largely derived from small cohorts and early-phase trials, underscoring the need for well-designed prospective studies to evaluate safety profiles, optimal dosing, and clinical efficacy in this setting.
Personalized strategies
Personalized therapeutic approaches are becoming increasingly integrated into treatment sequencing decisions. Biomarkers such as alpha-fetoprotein (AFP) levels, which correlate with tumor burden and biological aggressiveness, can inform prognosis and response to therapy[31,51]. Radiological response assessments using modified Response Evaluation Criteria in Solid Tumors (mRECIST) provide early indicators of treatment efficacy and may guide subsequent therapy initiation or modification[52]. Moreover, advances in immune profiling - including tumor-infiltrating lymphocyte (TIL) characterization and circulating immune markers - hold promise for predicting responsiveness to immunotherapy and tailoring combination regimens[53]. Leveraging these biomarkers may enable clinicians to individualize timing and agent selection, potentially improving outcomes and reducing unnecessary toxicity.
REAL-WORLD EXPERIENCES AND FUTURE DIRECTIONS
Data derived from registries and retrospective analyses have provided invaluable insights into the practical application of Y-90 radioembolization combined with systemic therapies in diverse, heterogeneous patient populations. These data generally corroborate findings from controlled clinical trials, affirming the
Despite encouraging results, challenges remain in optimizing patient selection and therapeutic sequencing in the real-world setting. Variability in practice patterns, access to specialized care, and multidisciplinary collaboration can influence outcomes, emphasizing the importance of coordinated care pathways involving interventional radiologists, hepatologists, medical oncologists, and radiation oncologists. Enhanced communication and integrated treatment planning are vital to tailor therapies based on individual patient characteristics, tumor biology, and response dynamics.
Future research priorities
Biomarkers for precision medicine
A pressing priority is the identification and validation of robust molecular and immune biomarkers that predict response or resistance to Y-90 combination therapies. Beyond conventional clinical markers such as AFP, emerging genomic and transcriptomic signatures, immune cell infiltration patterns, and circulating tumor DNA profiles hold promise for refining patient stratification. Such biomarkers could facilitate early identification of responders, guide adaptive treatment modifications, and inform novel agent selection, ultimately enabling a more personalized therapeutic approach.
Integration of novel agents
The evolving landscape of systemic therapies presents opportunities to enhance Y-90 combinations by incorporating next-generation agents. Dual immune checkpoint blockade targeting PD-1/PD-L1 and CTLA-4 pathways, adoptive cell therapies such as chimeric antigen receptor (CAR) T cells or TILs, and agents targeting the fibrotic tumor microenvironment may act synergistically with radiation-induced immunogenic effects. Investigating these combinations could overcome immune evasion mechanisms and potentiate durable antitumor responses, particularly in immunologically “cold” tumors refractory to conventional immunotherapy.
Elucidation of resistance mechanisms
A deeper mechanistic understanding of intrinsic and acquired resistance to both Y-90 and systemic therapies is essential. Tumor heterogeneity, hypoxia-driven angiogenesis, immune suppressive microenvironments, and molecular escape pathways all contribute to treatment failure. Advanced preclinical models and translational studies focusing on tumor-stroma interactions, immune checkpoint dynamics, and angiogenic signaling would enable the design of combination regimens aimed at circumventing resistance.
Multidisciplinary care models
Future clinical success will hinge on the development and implementation of multidisciplinary care frameworks that integrate expertise across specialties. Streamlined coordination can optimize timing and sequencing, proactively manage adverse effects, and enhance patient adherence and quality of life. Additionally, embedding real-time biomarker monitoring and adaptive trial designs within clinical workflows may accelerate the translation of mechanistic insights into improved therapeutic outcomes.
CONCLUSION
Y-90 radioembolization combined with systemic therapies, particularly targeted agents and ICIs, represents an evolving and promising strategy in the management of HCC. These combination approaches harness synergistic mechanisms - radiation-induced tumor cytotoxicity and vascular disruption, suppression of angiogenic escape through tyrosine kinase inhibition, and reinvigoration of antitumor immunity via checkpoint blockade - to enhance both local control and systemic efficacy.
Current preclinical and clinical data suggest that selected combinations may improve PFS and OS while maintaining a manageable safety profile. Nonetheless, the integration of Y-90 with systemic therapies in routine practice remains limited by the heterogeneity of existing studies and the lack of integration into standardized treatment algorithms. Prospective randomized trials are needed to define the optimal regimens, sequencing, and patient selection criteria.
Preliminary data show acceptable safety, with common adverse events, including liver enzyme elevations and manageable immune-related events. This variability in patient liver function, tumor burden, and immune status underscores the need for biomarker-driven personalization of treatment. The optimal sequencing and timing of Y-90 and systemic therapies require a nuanced balance between maximizing antitumor synergy and managing patient-specific factors and toxicities. A multidisciplinary approach encompassing interventional radiology, medical oncology, hepatology, radiation oncology, and immunology will be critical to the successful implementation of these regimens. Future research should aim to incorporate molecular and immunological profiling to identify patients most likely to benefit from specific combinations. Integrating clinical, radiologic, and molecular biomarkers into prospective trials will refine treatment algorithms, generating precise approaches that, when combined with multidisciplinary care, will be pivotal in optimizing therapeutic outcomes for patients with HCC.
As mechanistic understanding deepens and precision medicine advances, Y-90-based combination therapies have the potential to transform the therapeutic landscape of HCC, offering improved survival and quality of life for patients with this complex and historically refractory disease.
DECLARATIONS
Acknowledgments
The graphical abstract was created with BioRender.com (Created in BioRender. Hall, B. (2025) https://BioRender.com/ukhr5po)
Authors’ contributions
Conducted a literature review and made substantial contributions to the composition of the summary: Hall B, Ohs Z, Dervishi M, Stevens M
Made contributions to the conception of the review and performed administrative, technical, and material support: Sutter C, Davidson J
Availability of data and materials
Not applicable.
AI and AI-assisted tools statement
During the preparation of this manuscript, the AI tools OpenEvidence (version 2.0, released 2024-12-16) and ChatGPT (version 5, released 2025-08-07) were used solely for language editing. The tools did not influence the study design, data collection, analysis, interpretation, or the scientific content of the work. All authors take full responsibility for the accuracy, integrity, and final content of the manuscript.
Financial support and sponsorship
None.
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
0.
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74:229-63.
2. Singal AG, Llovet JM, Yarchoan M, et al. AASLD Practice Guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023;78:1922-65.
3. Galle PR, Forner A, Llovet JM, et al. EASL Clinical Practice Guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69:182-236.
4. Brown AM, Kassab I, Massani M, et al. TACE versus TARE for patients with hepatocellular carcinoma: Overall and individual patient level meta analysis. Cancer Medicine. 2022;12:2590-9.
5. Makary MS, Khandpur U, Cloyd JM, Mumtaz K, Dowell JD. Locoregional therapy approaches for hepatocellular carcinoma: recent advances and management strategies. Cancers. 2020;12:1914.
6. Makary MS, Ramsell S, Miller E, Beal EW, Dowell JD. Hepatocellular carcinoma locoregional therapies: Outcomes and future horizons. World J Gastroenterol. 2021;27:7462-79.
7. Vilgrain V, Pereira H, Assenat E, et al. Efficacy and safety of selective internal radiotherapy with yttrium-90 resin microspheres compared with sorafenib in locally advanced and inoperable hepatocellular carcinoma (SARAH): an open-label randomised controlled phase 3 trial. Lancet Oncol. 2017;18:1624-36.
8. Lee YB, Nam JY, Cho EJ, et al. A Phase I/IIa Trial of Yttrium-90 radioembolization in combination with durvalumab for locally advanced unresectable hepatocellular carcinoma. Clin Cancer Res. 2023;29:3650-8.
9. Mandlik DS, Mandlik SK, Choudhary HB. Immunotherapy for hepatocellular carcinoma: Current status and future perspectives. World J Gastroenterol. 2023;29:1054-75.
10. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76:681-93.
11. Teo J, Goh BK. Contra-lateral liver lobe hypertrophy after unilobar Y90 radioembolization: an alternative to portal vein embolization? World J Gastroenterol. 2015;21:3170-3.
12. Molvar C, Lewandowski R. Yttrium-90 radioembolization of hepatocellular carcinoma-performance, technical advances, and future concepts. Semin intervent Radiol. 2015;32:388-97.
13. Lewandowski R, Salem R. Yttrium-90 radioembolization of hepatocellular carcinoma and metastatic disease to the liver. Semin intervent Radiol. 2006;23:064-72.
14. Riaz A, Gates VL, Atassi B, et al. Radiation segmentectomy: a novel approach to increase safety and efficacy of radioembolization. Int J Radiat Oncol Biol Phys. 2011;79:163-71.
15. Busse NC, Al‐ghazi MSAL, Abi‐Jaoudeh N, et al. AAPm medical physics practice guideline 14.a: yttrium-90 microsphere radioembolization. J Appl Clin Med Phys. 2023;25:e14157.
16. Boas FE, Bodei L, Sofocleous CT. Radioembolization of colorectal liver metastases: indications, technique, and outcomes. J Nucl Med. 2017;58 Suppl:104S-11S.
17. Wagemans ME, Kunnen B, Stella M, et al. Comparison of 3 different therapeutic particles in radioembolization of locally advanced intrahepatic cholangiocarcinoma. J Nucl Med. 2024;65:272-8.
18. Villalobos A, Arndt L, Cheng B, et al. Yttrium-90 radiation segmentectomy of hepatocellular carcinoma: a comparative study of the effectiveness, safety, and dosimetry of glass-based versus resin-based microspheres. J Vasc Interv Radiol. 2023;34:1226-34.
19. Gulec SA, Mcgoron AJ. Radiomicrosphere dosimetry: principles and current state of the art. Semin Nucl Med. 2022;52:215-28.
20. Garin E, Guiu B, Edeline J, Rolland Y, Palard X. Trans-arterial radioembolization dosimetry in 2022. Cardiovasc Intervent Radiol. 2022;45:1608-21.
21. Feely M, Tondon R, Gubbiotti M, et al. Gastrointestinal tract injury by yttrium-90 appears largely restricted to resin microspheres but can occur years after embolization. Am J Surg Pathol. 2022;46:1234-40.
22. Kis B, Gyano M. Radiation pneumonitis after yttrium-90 radioembolization: a systematic review. J Vasc Interv Radiol. 2025;36:207-18.
23. Hickey RM, Lewandowski RJ, Salem R. Yttrium-90 radioembolization for hepatocellular carcinoma. Semin Nucl Med. 2016;46:105-8.
24. Salem R, Mazzaferro V, Sangro B. Yttrium 90 radioembolization for the treatment of hepatocellular carcinoma: Biological lessons, current challenges, and clinical perspectives: Hepatology. Hepatology. 2013;58:2188-97.
25. Tong AKT, Kao YH, Too CW, Chin KFW, Ng DCE, Chow PKH. Yttrium-90 hepatic radioembolization: clinical review and current techniques in interventional radiology and personalized dosimetry. BJR. 2016;89:20150943.
26. Garin E, Tselikas L, Guiu B, et al. Long-term overall survival after selective internal radiation therapy for locally advanced hepatocellular carcinomas: updated analysis of DOSISPHERE-01 trial. J Nucl Med. 2024;65:264-9.
27. Zhang R, Yao Y, Gao H, Hu X. Mechanisms of angiogenesis in tumour. Front. Oncol. 2024;14:1359069.
28. Wang L, Geng H, Liu Y, et al. Hot and cold tumors: immunological features and the therapeutic strategies. MedComm. 2023;4:e343.
29. Gajewski TF, Schreiber H, Fu Y. Innate and adaptive immune cells in the tumor microenvironment. Nat Immunol. 2013;14:1014-22.
30. Tong J, Tan Y, Ouyang W, Chang H. Targeting immune checkpoints in hepatocellular carcinoma therapy: toward combination strategies with curative potential. Exp Hematol Oncol. 2025;14:65.
31. Ricke J, Klümpen HJ, Amthauer H, et al. Impact of combined selective internal radiation therapy and sorafenib on survival in advanced hepatocellular carcinoma. J Hepatol. 2019;71:1164-74.
32. Öcal O, Schütte K, Zech CJ, et al. Addition of Y-90 radioembolization increases tumor response and local disease control in hepatocellular carcinoma patients receiving sorafenib. Eur J Nucl Med Mol Imaging. 2022;49:4716-26.
33. Chow PK, Gandhi M, Tan S, et al. ; on behalf of Asia-Pacific Hepatocellular Carcinoma Trials Group. SIRveNIB: selective internal radiation therapy versus sorafenib in asia-pacific patients with hepatocellular carcinoma. J Clin Oncol. 2018;36:1913-21.
34. Facciorusso A, Bargellini I, Cela M, Cincione I, Sacco R. Comparison between Y90 radioembolization plus sorafenib and Y90 radioembolization alone in the treatment of hepatocellular carcinoma: a propensity score analysis. Cancers. 2020;12:897.
35. Qin S, Chen M, Cheng A, et al. Atezolizumab plus bevacizumab versus active surveillance in patients with resected or ablated high-risk hepatocellular carcinoma (IMbrave050): a randomised, open-label, multicentre, phase 3 trial. The Lancet. 2023;402:1835-47.
36. Hack SP, Spahn J, Chen M, et al. IMbrave 050: A phase III trial of atezolizumab plus bevacizumab in high-risk hepatocellular carcinoma after curative resection or ablation. Future Oncol. 2020;16:975-89.
37. Yu S, Yu M, Keane B, et al. A pilot study of pembrolizumab in combination with y90 radioembolization in subjects with poor prognosis hepatocellular carcinoma. The Oncologist. 2024;29:270-e413.
38. Tai D, Loke K, Gogna A, et al. Radioembolisation with Y90-resin microspheres followed by nivolumab for advanced hepatocellular carcinoma (CA 209-678): a single arm, single centre, phase 2 trial. Lancet Gastroenterol Hepatol. 2021;6:1025-35.
39. Fenton SE, Kircher SM, Mulcahy MF, et al. A phase I study of nivolumab (NIVO) in combination with TheraSphere (Yttrium-90) in patients with advanced hepatocellular cancer. J Clin Oncol. 2021;39:e16183.
40. Centers for Disease Control and Prevention. Study of [Atezolizumab and Bevacizumab in Combination With Y^90 Radioembolization in HCC for Liver Transplant]: NCT07059494. CDC. Updated November 4, 2025. https://clinicaltrials.gov/study/NCT07059494. [Accessed on 20 May 2026].
41. Centers for Disease Control and Prevention. Study of [Efficacy and Safety of Yttrium-90 Microspheres Selective Internal Radiotherapy Combined with Immune Checkpoint Inhibitors and Anti-angiogenesis Drugs Sequential HAIC for Hepatocellular Carcinoma]: NCT06867432. CDC. Updated March 10, 2025. https://clinicaltrials.gov/study/NCT06867432. [Accessed on 20 May 2026].
42. Centers for Disease Control and Prevention. Study of [Immunotherapy and Radioembolisation for Metastatic Hepatocellular Carcinoma]: NCT05809869. CDC. Updated April 12, 2024. https://clinicaltrials.gov/study/NCT05809869. [Accessed on 20 May 2026].
43. Salem R, Lewandowski RJ, Mulcahy MF, et al. Radioembolization for hepatocellular carcinoma using yttrium-90 microspheres: a comprehensive report of long-term outcomes. Gastroenterology. 2010;138:52-64.
44. Salem R, Lewandowski RJ, Kulik L, et al. Radioembolization results in longer time-to-progression and reduced toxicity compared with chemoembolization in patients with hepatocellular carcinoma. Gastroenterology. 2011;140:497-507.e2.
45. Jones A, Degregorio P, Sung MW, Ramji Z, Ren M, Baron AD. Characterization and management of adverse reactions in patients with unresectable hepatocellular carcinoma treated with lenvatinib. JADPRO. 2023;14:598-607.
46. Kulik L, Vouche M, Koppe S, et al. Prospective randomized pilot study of Y90 +/− sorafenib as bridge to transplantation in hepatocellular carcinoma. J Hepatol. 2014;61:309-17.
47. Ramos-casals M, Brahmer JR, Callahan MK, et al. Immune-related adverse events of checkpoint inhibitors. Nat Rev Dis Primers. 2020;6:38.
48. Zhan C, Ruohoniemi D, Shanbhogue KP, et al. Safety of combined yttrium-90 radioembolization and immune checkpoint inhibitor immunotherapy for hepatocellular carcinoma. J Vasc Interv Radiol. 2020;31:25-34.
49. Malone CD, Bajaj S, He A, et al. Combining radioembolization and immune checkpoint inhibitors for the treatment of hepatocellular carcinoma: the quest for synergy. J Vasc Interv Radiol. 2025;36:414-424.e2.
50. Vogel A, Cervantes A, Chau I, et al. Hepatocellular carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29:iv238-55.
51. Riaz A, Ryu RK, Kulik LM, et al. Alpha-fetoprotein response after locoregional therapy for hepatocellular carcinoma: oncologic marker of radiologic response, progression, and survival. J Clin Oncol. 2009;27:5734-42.
52. Llovet JM, Di Bisceglie AM, Bruix J, et al. ; for the panel of experts in HCC-Design Clinical Trials. Design and endpoints of clinical trials in hepatocellular carcinoma. JNCI: J Nat Cancer I. 2008;100:698-711.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Special Topic
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].