


Fascial ball graft in Asian rhinoplasty: a tunable, non-translucent option for tip definition and augmentation
 0
0 Abstract
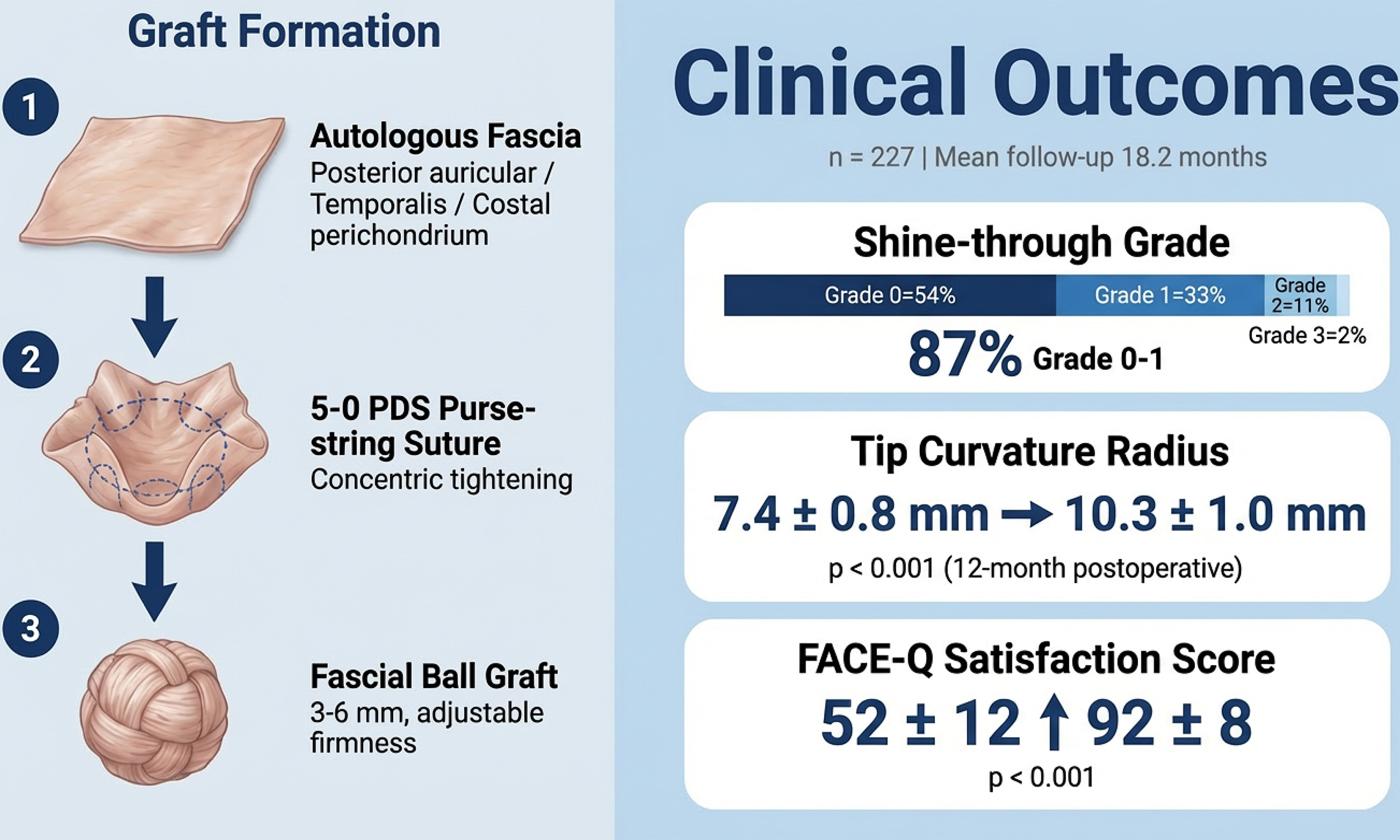
Thin-skinned Asian rhinoplasty is frequently complicated by cartilage visibility and oversharpening of the nasal tip. We introduce the fascial ball graft as a tunable on-lay technique for nasal tip augmentation and camouflage. A retrospective review was conducted of 227 patients (43 males, 184 females) who underwent fascial ball graft placement between 2020 and 2025 at a single rhinoplasty center. Patients were divided into two groups: Group A (n = 84), in which the fascial ball served as the sole on-lay augmentation graft; and Group B (n = 143), in which the fascial ball was placed over an auricular cartilage cap for layered augmentation. The fascial ball was constructed from autologous fascia (posterior auricular, temporalis, or costal perichondrium) using a 5-0 polydioxanone (PDS) purse-string suture, allowing intraoperative adjustment of thickness (3-6 mm) and firmness. Shine-through (0-3 scale), tip curvature radius, and FACE-Q (a validated patient-reported outcome measure for facial aesthetic procedures) “Satisfaction With Nose” scores were evaluated. Mean follow-up was 18.2 months (range 6-24 months). Shine-through was grade 0-1 in 87% of cases. Tip curvature radius significantly increased from 7.4 ± 0.8 mm preoperatively to 10.3 ± 1.0 mm at 12 months (P < 0.001), indicating improved roundness while avoiding bulbosity. FACE-Q scores increased from 52 ± 12 to 92 ± 8 (P < 0.001). No major complications were noted. The fascial ball on-lay graft provides tunable augmentation and non-translucent soft-tissue coverage, effectively achieving desired tip projection while preventing cartilage visibility in both primary and revision Asian rhinoplasty.
Keywords
INTRODUCTION
Asian rhinoplasty frequently requires structural enhancement due to thicker dermis, higher sebaceous content, and a comparatively weaker cartilaginous framework. These anatomical features, together with limited septal cartilage, make it challenging to maintain long-term projection and definition[1,2]. Furthermore, the thick soft-tissue envelope limits light transmission, making any irregularities or cartilage visibility more noticeable under certain lighting conditions[3,4].
In revision cases, fibrosis and adherence between skin and cartilage further complicate secondary dissection. Conventional techniques such as diced or crushed cartilage filler grafts often exhibit translucency, resorption, or palpable irregularity[1,4]. Park et al. introduced deep temporalis fascia for camouflage in Asians, and
To overcome these limitations, we have developed a technique using a fascial ball graft, in which autologous fascia is compacted into a spherical form and serves as an on-lay augmentation graft for the nasal tip. This graft not only prevents translucency of underlying cartilage grafts but also allows intraoperative adjustment of thickness (3-6 mm) and firmness, creating a natural, rounded tip contour. In cases requiring greater projection (> 4 mm), the fascial ball can be layered over a thin auricular cartilage cap, combining structural augmentation with soft-tissue camouflage. This tunable approach addresses both the aesthetic goal of a rounded, non-translucent tip and the functional need for individualized projection control. In this Technical Note, we describe the surgical technique, indications, and clinical outcomes of the fascial ball graft, with quantitative assessment of shine-through, tip curvature radius, and patient satisfaction.
METHODS
Study design and patient selection
This was a retrospective review of 227 consecutive patients (43 males, 184 females) who underwent rhinoplasty with fascial ball on-lay graft placement at WOM Clinic Ginza, Tokyo, between January 2020 and June 2025.
Inclusion criteria
· Patients undergoing primary or revision rhinoplasty requiring nasal tip modification or camouflage of actual or potential cartilage translucency
· Availability of standardized pre- and postoperative photographs
· A minimum follow-up period of 6 months
Exclusion criteria
· Active infection at the time of surgery
· Severe hypertrophic scarring or keloids of the nasal soft-tissue envelope
· History of nasal skin or soft-tissue radiation therapy
· Incomplete records or follow-up < 6 months
A total of 227 patients met these criteria. Mean follow-up was 18.2 months (range: 6-24 months). Outcome measures were assessed at the final available follow-up for each patient (minimum 6 months postoperatively).
Ethical approval and consent to participate
This retrospective study was granted an exemption from ethical approval by the Institutional Review Board of WOM Clinic Ginza (IRB No. WOM-IRB-2024-001; March 12, 2024).
The study was conducted in accordance with the Declaration of Helsinki.
Written informed consent for surgery, clinical photography, and academic publication was obtained from all patients.
Surgical technique
Fascia was harvested from posterior auricular fascia, deep temporalis fascia, or costal fascia/perichondrium. The average size of harvested fascia was 10-20 mm × 10-15 mm.
Harvesting technique
· Posterior auricular fascia: An incision was made behind the ear; dissection was limited to the superficial layer to minimize donor morbidity[6].
· Temporalis fascia: An incision along the hairline above the zygomatic arch was used, maintaining dissection above the superficial temporal fat pad to avoid injury to the frontal branch of the facial nerve[5].
· Costal perichondrium: Costal fascia/perichondrium was obtained through minimal subperichondrial dissection, preserving the deep layer to prevent depression deformity[2,8] [Figure 1].

Figure 1. Surgical formation and placement of the fascial ball graft. (Left) Harvested fascia (costal perichondrium, 10-20 mm × 10-15 mm); (Middle) The fascia compacted into a spherical graft using a 5-0 PDS purse-string suture; (Right) Intraoperative placement of the fascial ball graft between the domes after tip exposure. PDS: Polydioxanone suture.
Formation of the fascial ball
The fascia was compacted into a spherical shape using a circumferential 5-0 polydioxanone (PDS) purse-string suture, allowing intraoperative adjustment of graft thickness (3-6 mm) and firmness. Suture tension controlled the firmness: tighter for greater projection, looser for thin-skin camouflage. The resulting graft was soaked in saline with antibiotics until implantation.
Patient grouping based on augmentation requirements
Patients were divided into two groups based on the degree of nasal tip augmentation required:
Group A: Fascial ball as sole on-lay augmentation (n = 84)
Indications: Patients requiring moderate tip projection (2-4 mm) where the fascial ball alone could achieve the desired contour. This approach was preferred when:
· Underlying tip support structures (septal extension grafts or columellar struts) provided adequate foundational projection
· The primary goal was camouflage of potential cartilage translucency with soft-tissue coverage
· Minimal additional structural augmentation was needed
Technique: The fascial ball (3-6 mm thickness, adjusted intraoperatively) was placed directly over the underlying support structures as an on-lay graft. No cartilage cap was used in this group.
Group B: Layered augmentation with cartilage cap plus fascial ball (n = 143)
Indications: Patients requiring greater tip projection (> 4 mm) where the fascial ball alone was insufficient to achieve the desired height. This layered approach was used when:
· Greater structural augmentation was needed beyond the capacity of fascia alone
· The underlying framework required additional height and definition
· In revision cases where existing structures were depleted or fibrotic[9,10]
Technique: a thin auricular cartilage cap (0.5-1.0 mm thickness) was first shaped and placed on the underlying support framework to provide initial structural augmentation. The fascial ball (3-6 mm thickness, adjusted intraoperatively) was then placed over the cartilage cap as the superficial layer, serving dual purposes: (1) adding an additional 1-3 mm of projection; and (2) providing non-translucent soft-tissue coverage to prevent shine-through of the underlying cartilage.
Cartilage source rationale (Group B only)
Auricular cartilage was consistently selected for the cartilage cap in Group B because of its favorable pliability and natural curvature, which are well-suited for surface refinement in Asian rhinoplasty[1,2,11,12]. Although septal cartilage was harvested and used for deeper structural support - particularly as septal extension grafts - in primary cases[1,2,13,14], the surface cap itself was fashioned from auricular cartilage to maintain a natural, rounded tip contour. In revision rhinoplasty, septal cartilage was often depleted or fibrotic[9,10]; therefore, auricular cartilage served as the primary graft source. Costal cartilage was reserved for cases requiring stronger structural support or projection[8,15]. Even when costal cartilage was used for deeper support, the superficial cap graft remained auricular cartilage to avoid excessive rigidity and to maintain a natural tip contour appropriate for Asian noses.
Underlying tip support structures
Regardless of group assignment, all patients received appropriate underlying tip support structures (septal extension grafts, columellar struts, or shield grafts) tailored to individual anatomical needs. However, the focus of this Technical Note is on the on-lay augmentation and camouflage techniques (fascial ball with or without cartilage cap), rather than the deep support structures, which varied based on primary vs. revision status and preoperative anatomy.
Outcome assessment
Shine-through grading was assessed at final follow-up using standardized frontal and oblique photographs. Grading was based on a 0-3 scale according to criteria described by Daoud et al. and Chang et al.[3,4]:
· Grade 0: No visible translucency; cartilage contour cannot be detected under standard lighting.
· Grade 1: Minimal shine or glare detectable only by trained surgeons under strong lighting; patients are unaware.
· Grade 2: Definite translucency or contour visibility on standard photographs, noticeable to surgeons but usually not bothersome to patients.
· Grade 3: Strong glare and clearly visible cartilage contour; patients recognize it as a cosmetic concern.
Two board-certified plastic surgeons, blinded to patient group and surgical details, independently evaluated all images. Inter-rater agreement was excellent (Cohen’s κ = 0.88).
Tip curvature radius was measured using ImageJ software (National Institutes of Health, version 1.53)[11,12,16] on standardized frontal photographs obtained at final follow-up. A circle was fitted to the arc connecting the tip-defining points, and the radius was measured in millimeters. A smaller radius indicates a sharper tip; a larger radius indicates a softer, more rounded contour. Two blinded evaluators performed the measurements. To assess reliability, repeat measurements were performed on 15 randomly selected cases; the mean intra-observer error was 0.21 mm, and the inter-rater intraclass correlation coefficient (ICC) was 0.92, indicating excellent reliability. Preoperative curvature values showed a wider distribution reflecting natural variability in Asian nasal tips; postoperative values were expected to converge toward a physiologic rounded contour.
Patient-reported outcomes were assessed using the FACE-Q (a validated patient-reported outcome measure for facial aesthetic procedures) “Satisfaction With Nose” module[4,17], a validated 0-100 Rasch-transformed scale in which higher scores indicate greater satisfaction. Scores were collected preoperatively and at final follow-up (mean 18.2 months; range: 6-24 months).
Statistical analysis
Data were analyzed using SPSS version 28 (IBM Corp., Armonk, NY, USA). Continuous variables (tip curvature radius and FACE-Q scores) were compared using paired t-tests. Shine-through grades were analyzed using the Wilcoxon signed-rank test. Statistical significance was defined as P < 0.05.
RESULTS
Between 2020 and 2025, 227 patients underwent this procedure: 84 in Group A and 143 in Group B. Ages ranged from 18 to 55 years (43 males, 184 females). Among them, 41 had thin skin, and 108 were revision cases.
Shine-through
At final follow-up (mean: 18.2 months), most cases showed low-grade translucency:
· Grade 0: 54%
· Grade 1: 33%
· Grade 2: 11%
· Grade 3: 2%
Thus, 87% of cases were Grade 0-1, demonstrating adequate prevention of clinically appreciable shine-through[3,4]. No patient showed worsening of the shine-through grade during the follow-up period.
Tip curvature radius
At final follow-up, postoperative curvature radius significantly increased compared with preoperative values, indicating maintenance of projection with avoidance of oversharpening[11,12,16].
· Preoperative: 7.4 ± 0.8 mm
· 12-month postoperative: 10.3 ± 1.0 mm
(P < 0.001; paired t-test)
Despite the broader dispersion at baseline - due to a mixture of naturally rounded primary cases and overly sharp revision cases - the postoperative values consistently converged around 10 mm, which corresponds to a natural, non-bulbous tip contour in Asian rhinoplasty[1,2,16]. No patient experienced late deprojection during the follow-up period.
Representative cases
· Case 1 (thin skin): No translucency at 12 M [Figure 2]
· Case 2 (moderate skin): Projection preserved, smoother contour [Figure 3]
· Case 3 (revision): Adhesions mild, dissection easier [Figure 4]

Figure 2. Primary case using costal perichondrium. Preoperative and postoperative (12 months) comparisons show natural tip projection without cartilage translucency (shine-through). (Left) Lateral view; (Middle) Frontal view; (Right) Oblique view. Postoperative images demonstrate smooth contour, balanced curvature, and soft tip definition achieved by the fascial ball graft technique.

Figure 3. Primary case using posterior auricular fascia. Preoperative and postoperative (12 months) comparisons demonstrate improved tip definition and natural projection without oversharpening. (Left) Lateral view; (Middle) Frontal view; (Right) Oblique view. Postoperative images show a balanced curvature of the nasal tip and smooth contour achieved with the fascial ball graft using posterior auricular fascia.
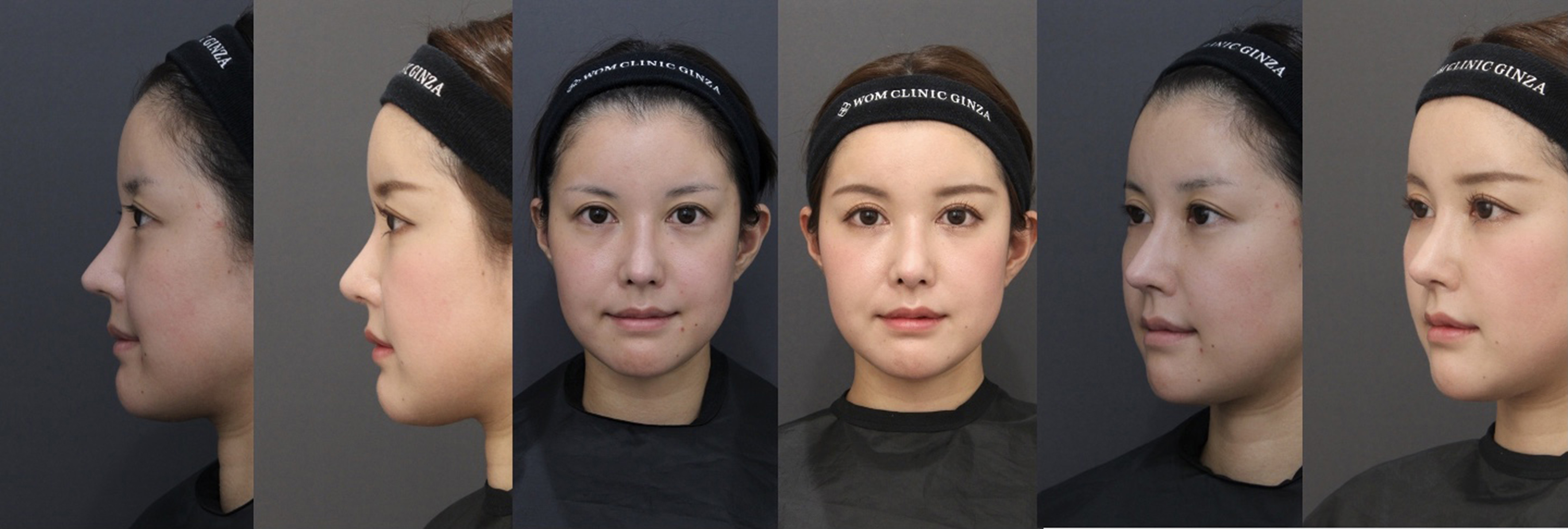
Figure 4. Revision case using temporalis fascia. Preoperative and postoperative (12 months) comparisons show elimination of cartilage visibility and improved nasal tip contour. (Left) Lateral view; (Middle) Frontal view; (Right) Oblique view. Postoperative images illustrate the effectiveness of temporalis fascia in camouflaging thin skin, achieving soft projection and natural definition while maintaining long-term stability.
FACE-Q
Patient-reported satisfaction with the nose improved markedly at final follow-up
· Preoperative FACE-Q: 52 ± 12
· Postoperative FACE-Q: 92 ± 8
(P < 0.001)
High satisfaction was maintained throughout the follow-up period, with no patients reporting delayed dissatisfaction.
Complications
No infection, graft displacement, hematoma, or major complications occurred during the follow-up period. Palpability was favorable in all cases, and there were no instances of clinically problematic stiffness. No patient required revision surgery for complications related to the fascial ball graft.
DISCUSSION
Fascia has long been used for camouflage in rhinoplasty, including posterior auricular fascia, temporalis fascia, and fascia lata[3,5-7]. Crushed or diced cartilage fillers can provide volume but carry risks of translucency, surface irregularities, and palpable edges[1,4]. The fascial ball graft represents a structural evolution. Its spherical, purse-string design distributes tension evenly, reduces focal stress on the overlying skin, and allows intraoperative adjustment of stiffness.
Clinically, the fascial ball graft acts as a biologic spacer that minimizes skin-cartilage adhesion, particularly advantageous in revision rhinoplasty where scar tissue and graft irregularities are common[9,10]. The graft integrates gradually with the surrounding tissue without calcification or significant distortion. Long-term stability has been reported in follow-ups up to 4 years[17].
In our series, outcomes were favorable in both primary (n = 119) and revision (n = 108) cases. Revision cases generally presented with more complex anatomical conditions - including scar tissue and reduced cartilage availability - reflecting the inherent challenges of secondary rhinoplasty. Despite this complexity, overall clinical outcomes and patient-reported satisfaction were comparable between the two subgroups.
Because this study was not specifically designed or statistically powered to perform formal subgroup comparisons, these observations should be interpreted descriptively rather than as definitive comparative conclusions. Dedicated prospective studies are warranted to further evaluate subgroup-specific outcomes.
Auricular cartilage was intentionally selected as the cartilage cap material in Group B (n = 143, requiring
In revision cases, septal cartilage is often depleted, scarred, or mechanically compromised; auricular cartilage therefore provides a reliable alternative[9,10]. Even when costal cartilage was required for deeper structural reinforcement or projection[8,15], the cap remained auricular to avoid “overly hard” tips and to maintain a natural rounded profile.
Our quantitative curvature analysis demonstrated that the fascial ball graft can soften overly sharp tips while preserving definition in naturally round Asian tips. Preoperative curvature radius varied because our cohort included both primary Asian noses - typically more rounded - and revision noses that had become excessively sharp due to prior surgeries. Despite this heterogeneity, postoperative curvature values converged toward a physiologically ideal range around 10 mm, consistent with an aesthetically pleasing, non-bulbous contour[1,2,16]. This suggests that the fascial ball graft allows surgeons to “normalize” tip shape across a broad spectrum of preoperative presentations.
Shine-through grading further supports the technique’s effectiveness. The low frequency of Grade 2-3 translucency, combined with the high proportion of Grade 0-1 outcomes, indicates robust camouflage of underlying cartilage[3,4]. In addition, FACE-Q data confirmed that patients perceived meaningful aesthetic improvement, aligning objective photometric findings with subjective satisfaction[4,17].
From a soft-tissue preservation perspective, fascial ball grafts and auricular caps are compatible with modern preservation rhinoplasty principles, which seek to maintain the soft-tissue envelope and nasal dynamics[18-21]. The fascial layer restores a gliding interface between skin and cartilage, facilitating expressive tip motion and improving revision dissection when necessary.
Patients were evaluated at their final available follow-up (minimum 6 months; mean 18.2 months; range 6-
Shine-through grades remained stable (87% Grade 0-1), and tip curvature radius converged toward approximately 10 mm by 6 months without evidence of late deprojection. FACE-Q scores remained high, with no cases of delayed dissatisfaction or graft-related revision.
While the present follow-up duration supports early- to mid-term stability, longer-term observation beyond 24 months is necessary to fully evaluate potential late fascial volume changes. Although fascia grafts may undergo gradual resorption in some settings, no progressive contour change was identified within our cohort. Prospective studies with standardized long-term follow-up are warranted.
Limitations
This study has several limitations. First, it is a retrospective, single-center analysis without randomization. Group allocation (Group A vs. Group B) was determined according to predefined augmentation thresholds (2-4 mm for Group A; > 4 mm for Group B) and individualized anatomical requirements rather than random assignment. As such, direct causal inference between techniques is limited, and the findings should be interpreted as descriptive technical outcomes rather than results of a comparative trial.
Second, the cohort included a heterogeneous population of both primary and revision rhinoplasty cases. Although subgroup characteristics were reported, the study was not designed or statistically powered to perform definitive comparative analyses between primary and revision cases or between Group A and Group B techniques. Future investigations should address these comparisons prospectively with balanced allocation.
Third, follow-up duration varied (6-24 months; mean 18.2 months). While clinical practice guidelines recommend a minimum 12-month follow-up for rhinoplasty outcome assessment[22], longer-term data beyond 24 months are necessary to more fully evaluate potential late fascial volume changes and exclude delayed resorption.
Fourth, underlying structural support techniques (e.g., septal extension grafts, columellar struts, alar batten grafts) were individualized based on patient anatomy and surgical indication. Although this reflects real-world clinical practice, it may confound precise attribution of tip projection and contour changes solely to the fascial ball graft.
Finally, no direct comparison was performed against other established camouflage techniques, such as diced cartilage fascia grafts[8,15] or fascia-lata-based augmentation. Prospective, controlled studies with standardized long-term follow-up intervals are warranted to further validate durability and enable direct comparison with alternative techniques.
CONCLUSION
The fascial ball graft represents a tunable on-lay augmentation technique that provides non-translucent soft-tissue coverage for nasal tip refinement in Asian rhinoplasty. When applied alone or layered over a thin auricular cartilage cap according to augmentation requirements, it enables controlled projection while preserving a natural, rounded contour.
In this 227-patient series, quantitative evaluation demonstrated convergence of tip curvature toward approximately 10 mm, reduced shine-through (87% Grade 0-1), and high patient-reported satisfaction at early-to-mid-term follow-up (mean 18.2 months; range 6-24 months). No progressive contour deterioration or graft-related complications were observed within the follow-up period.
Although longer-term data and direct comparative studies are warranted, the fascial ball graft appears to be a practical and versatile camouflage strategy for both primary and revision Asian rhinoplasty requiring precise control of projection and translucency.
DECLARATIONS
Authors’ contributions
Concept, study design, data analysis, manuscript writing: Nakai T
Surgical supervision, data verification, manuscript review: Sasaki K
All authors read and approved the final manuscript.
Availability of data and materials
All data analyzed during this study are available from the corresponding author upon reasonable request.
AI and AI-assisted tools statement
Not applicable.
Financial support and sponsorship
None.
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
This retrospective study was granted an exemption from ethical approval by the Institutional Review Board of WOM Clinic Ginza (IRB No. WOM-IRB-2024-001; March 12, 2024). The study was conducted in accordance with the Declaration of Helsinki. Written informed consent to participate was obtained from all patients included in this study.
Consent for publication
Explicit written informed consent for publication of clinical images was obtained from all patients, including those whose images were partially anonymized with mosaic masking of the eye region and those shown in full-face format.
Copyright
© The Author(s) 2026.
REFERENCES
1. Kim TK, Jeong JY. Surgical anatomy for Asian rhinoplasty: Part III. Arch Craniofac Surg. 2023;24:1-9.
2. Jang YJ, Alfanta EM. Rhinoplasty in the Asian nose. Facial Plast Surg Clin North Am. 2014;22:357-77.
3. Daoud RM, Alelyani AA, Bakhamees BH, et al. Thin skin in rhinoplasty: considerations for camouflaging dorsal nasal irregularities. Cureus. 2024;16:e66595.
4. Chang BL, Cho WK, Jang YJ. Free crushed cartilage filler graft to optimize tip aesthetics in Asian rhinoplasty. Aesthetic Plast Surg. 2025;49:2735-45.
5. Park SW, Kim JH, Choi CY, Jung KH, Song JW. Various applications of deep temporal fascia in rhinoplasty. Yonsei Med J. 2015;56:167-74.
6. La Padula S, Pensato R, Pizza C, et al. The use of posterior auricular fascia graft (PAFG) for slight dorsal augmentation and irregular dorsum coverage in primary and revision rhinoplasty: a prospective study. Aesthetic Plast Surg. 2024;48:862-71.
7. Mohebbi A, Hamidian R, Poosti SB, Hosseini SS. CenoDerm vs. fascia lata for the prevention of dorsal nasal irregularities in rhinoplasty. Iran J Otorhinolaryngol. 2016;28:241-8.
8. Toriumi DM, Bared A. Revision of the surgically overshortened nose. Facial Plast Surg. 2012;28:407-16.
9. Gunter JP, Rohrich RJ. External approach for secondary rhinoplasty. Plast Reconstr Surg. 1987;80:161-74.
10. Park P, Jin HR. Diced cartilage in fascia for major nasal dorsal augmentation in Asians: a review of 15 consecutive cases. Aesthetic Plast Surg. 2016;40:832-9.
11. Savetsky IL, Avashia YJ, Rohrich RJ. Nasal tip shaping finesse in rhinoplasty. Plast Reconstr Surg. 2021;148:1278-9.
12. Daniel RK, Palhazi P. The nasal ligaments and tip support in rhinoplasty: an anatomical study. Aesthet Surg J. 2018;38:357-68.
13. Boccieri A, Macro C. Septal considerations in revision rhinoplasty. Facial Plast Surg Clin North Am. 2006;14:357-71.
14. Chao JW, Malyavko A. The utility of diced cartilage fascia graft augmentation of the nasal dorsum in transgender feminizing rhinoplasty. Plast Reconstr Surg. 2020;146:697e-8.
15. Chao JW, Malyavko A. The utility of diced cartilage fascia graft augmentation of the nasal dorsum in transgender feminizing rhinoplasty. Plast Reconstr Surg. 2020;146:697e-8.
16. Mattos D, Hanna SA, Datta S, Reish RG. Positioning the nasal tip in rhinoplasty. Plast Reconstr Surg. 2025;156:606e-15.
17. Mun SJ, Choi YS, Kim JH, Shim WS, Jung HJ. Evaluation of the esthetic and functional outcomes of extracorporeal septoplasty for rhinoplasty in Asian patients. Clin Exp Otorhinolaryngol. 2021;14:100-7.
18. Kovacevic M, Kosins AM, Göksel A, et al. Optimization of the soft tissue envelope of the nose in rhinoplasty utilizing fat transfer combined with platelet-rich fibrin. Facial Plast Surg. 2021;37:590-8.
19. Cakir B, Oreroğlu AR, Doğan T, Akan M. A complete subperichondrial dissection technique for rhinoplasty with management of the nasal ligaments. Aesthet Surg J. 2012;32:564-74.
20. Toriumi DM, Patel AB, DeRosa J. Correcting the short nose in revision rhinoplasty. Facial Plast Surg Clin North Am. 2006;14:343-55.
21. Gonçalves Ferreira M, Ishida LC, Ishida LH, Santos M. Ferreira-ishida technique: spare roof technique B. step-by-step guide to preserving the bony cap while dehumping. Plast Reconstr Surg. 2022;149:901e-4.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].