


Volume 2 (2015) – 72 articles
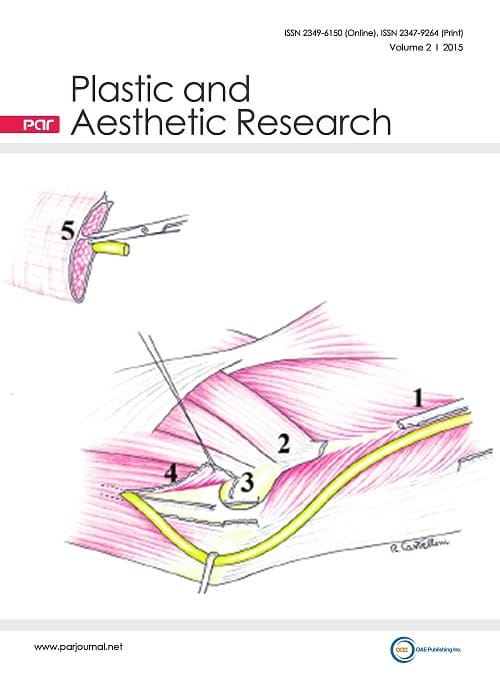
Cover Picture: Ulnar nerve neuropathy at the elbow represents the second most frequent compression neuropathy of the upper extremity. Of the five different anatomical areas responsible for ulnar nerve compression at the elbow region, the epitrochlear-olecranon channel and Osborne's arcade are the most common. An additional cause of nerve damage is a dynamic process in which the ulnar nerve dislocates anteriorly at the epitrochlear-olecranon level during elbow flexion, partially or completely, causing nerve friction and constriction leading to chronic neuropathic pain. Failure after primary surgery is generally secondary to procedural errors or technical omissions, frequently represented by incomplete nerve decompression, failure to recognize nerve instability after nerve decompression, loosening of the nerve anchor after superficial nerve transposition with consequent spontaneous nerve relocation in the epitrochlear-olecranon channel, perineural fibrosis and neurodesis, which creates new nerve compression. In association with the clinical evaluation, electromyography studies, magnetic resonance imaging and ultrasound are useful tools that may aid in the decision-making process when considering revision surgery. Superficial anterior transposition is the most commonly employed technique but also has a high failure rate, as opposed to anterior deep transposition that is the method of choice for many surgeons despite being more technically demanding. The results of revision surgery following recalcitrant ulnar nerve compression at the elbow are inferior to those obtained after primary surgery. Nonetheless, the clinical advantages remain relevant provided that the revision surgery is performed by an expert surgeon. To avoid misinterpretation, the patient is completely informed of the quality of results.
view this paper
Read Online Viewed:
Download This Volume Viewed:




