


Rare disease preparedness: the time is now
 0
0 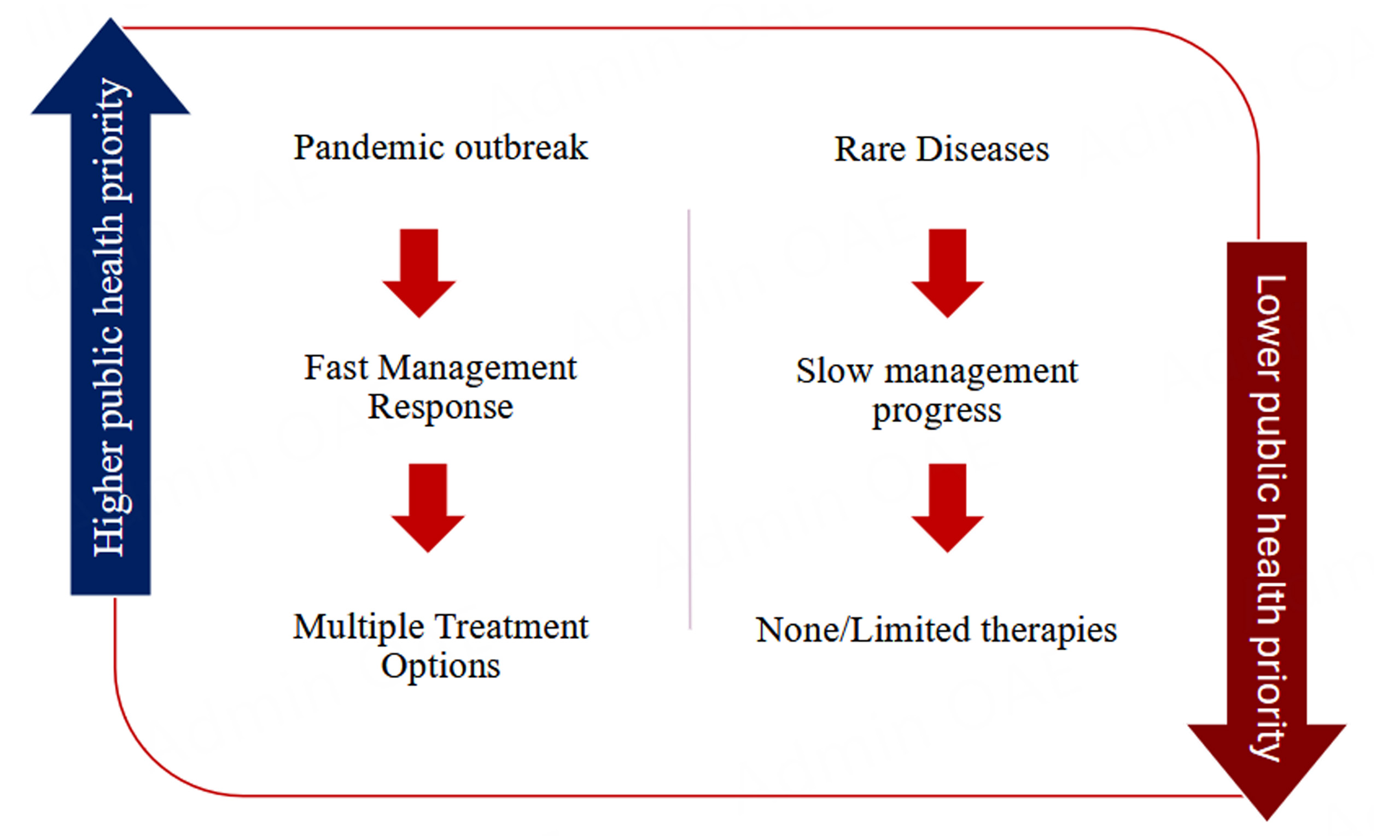
INTRODUCTION
Rare diseases (RDs) affect 1 in 2,000 individuals or fewer in the general population, with 80% having a genetic basis. With 70% of RDs starting in childhood, it is estimated that 300-400 million individuals are living with a RD globally[1]. A patient’s journey is arduous, with reports indicating that approximately 73% of RD patients experience at least one misdiagnosis and an average delay of 8 years to receive a correct diagnosis. The USA considers a disease rare if it affects fewer than 200,000 individuals[2], while the European Union (EU)[3] or Australia defines rare as affecting fewer than 1 in 2,000 persons. In other geographies, it is reported anywhere from 5-76 per 100,000 people[4]. The complex, heterogeneous nature of RDs makes them difficult to assess in aggregates; however, based on incidence, some more commonly known RDs are Duchenne Muscular Dystrophy (DMD), sickle cell disease, cystic fibrosis, haemophilia, and Huntington’s disease[5].
The recent coronavirus (COVID-19) pandemic, a global disruptive event, had a major negative impact on health and the global economy; however, disparities were felt more strongly by vulnerable communities, particularly those from lower socioeconomic backgrounds and those in Low- and Middle-Income Countries (LMIC). An important question raised was which elements undermine equity, a key factor that also limits health care access and the management of RD patients, who are structurally neglected by health systems[6].
Analysing what went wrong in the management of earlier global outbreaks in terms of equity could help craft an instrument to address these inequalities, prevent them from occurring in the first place, and inform the steps needed to prioritise PLWRD. Lastly, there must be political will to strengthen health care systems and address the challenges faced by RD patients. The pandemic proved that there is still a critical need for global collaboration to align and advocate for policies and programmes to increase awareness in line with national priorities, while also expanding programmes that combat marginalisation and address inconsistent and inequitable access to funding, resources, diagnosis, and treatment. Globally, addressing gaps in health care accessibility and services is a priority for PLWRD, who are often constrained not only by reduced budgets, resources and shortage of experts but also by stigma and societal exclusion.
The demand for universal health coverage policies for RDs has been endorsed in recent years by patient advocacy groups, consortia, and public and private institutions as an essential step in reducing widespread disparities for PLWRD. Early identification of RDs could prevent the onset of disease symptoms or delay progression, thereby reducing child mortality and improving the quality of life of PLWRD, while also decreasing the total cost to society. The landmark decision of the United Nations (UN), during the Seventy-eighth World Health Assembly (24 May 2025), to declare RDs as a global health priority, in alignment with the UN commitment to achieve the 2030 Sustainable Development Goals of “Leaving no one behind,” represents a crucial moment of awareness. It highlights the urgency for quality, affordable, and equitable health care for RD patients[7].
In this perspective article, we reflect on where RDs fit in global health challenges, care pathways, risk factor interventions and population screening.
Collective burden
Approximately 8,000 different RDs exist across the globe. Such diseases are not “rare” when viewed from a population perspective; however, public health systems are not designed to detect, track and respond to low-incidence conditions in real time. It is interesting to note that, in response to the threat of future global pandemics, both public and private sectors developed a set of commitments to improve equitable access to essential medical resources. These include commitments to rapidly scale up production and distribution capabilities, in collaboration with relevant programmes. In this context, it is worth acknowledging that several learnings from the management of pandemics could be used as inspiration for the development of a Rare Disease Preparedness Roadmap [Figure 1].
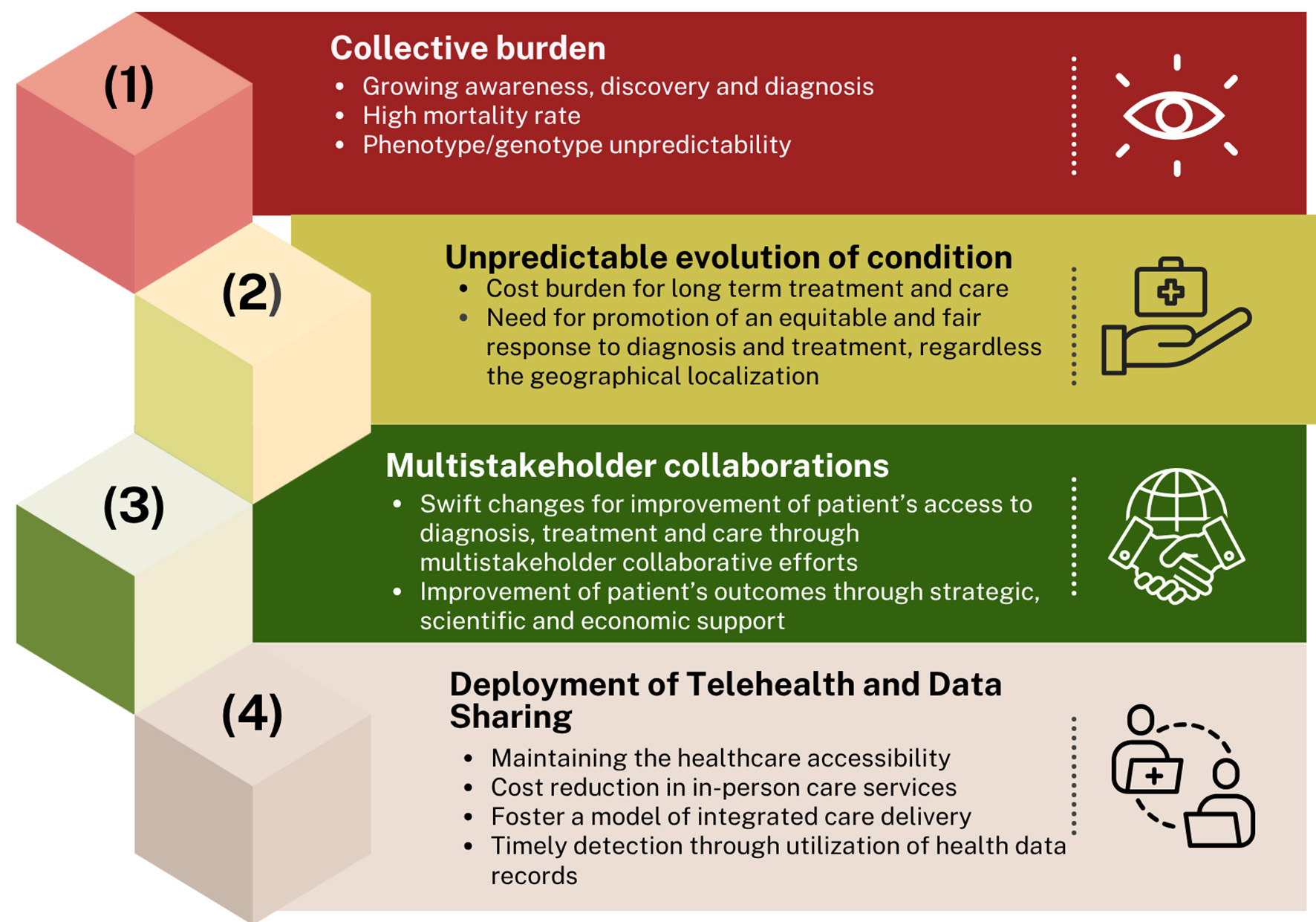
Figure 1. Rare Disease Preparedness Roadmap. Reasons for acknowledging rare diseases as a health priority.
Growing awareness, discovery and diagnosis
Despite growing advances in research, diagnosis, and treatment, including adjustments in policy and many health care frameworks, RDs are still at a standstill in certain regions of the world. However, it should be noted that multiple initiatives heavily contributed to enhancing recognition and knowledge, such as (1) the establishment of European Reference Networks (ERNs), by aligning resources available in centres of expertise for better access to clinical evaluation and support[8]; (2) the creation of “Rare Disease Day”, a global awareness campaign launched by EURORDIS-Rare Disease Europe in 2008 to raise awareness and advocate for the rights of PLWRD, celebrated every last day of February[9]; and (3) the creation of the Undiagnosed Diseases Network, facilitating research into the etiology of undiagnosed diseases[10].
High mortality rate
The prognosis for patients with RDs is variable, even in individuals with the same condition. Recent studies show a higher mortality rate in RD patients compared with the general population, with variations influenced by gender, age, and disease group. This is further complicated by the under-representation of specific RD characteristics in coding systems used to capture mortality and morbidity data, which are often designed to collect data on a specific disease or group of related diseases, thereby limiting the availability of information on unrelated RDs.
Economically, the burden of RDs is approximately 10-fold higher compared with common diseases on a per-patient-per-year basis (PPPY), driven by direct costs (medical and non-medical costs such as hospitalisation, professional visits, palliative care, medical products, etc.) and mortality costs[11]. RDs have been reported to have a poor prognosis due to their complexity and limited knowledge of underlying mechanisms, with mortality rates being up to 13 times higher in RD patients compared with individuals with common diseases[12,13]. PLWRD are likely to die earlier than the general population, mainly in the first years of life. The mortality rate reaches a peak in the paediatric population in the 1-4 years age group[14].
Phenotype/genotype unpredictability
For RDs, correlations between genotype and phenotype are not fully elucidated, and a clear explanation for clinical heterogeneity remains lacking. In the case of PLWRD in particular, complex mutations are frequently reported, where the genotype fails to express many of the features of the disease. While a single gene can be associated with significant phenotypic heterogeneity, the reverse is rarely applicable—namely, a distinct phenotype linked to different genes[15]. Reduced penetrance can be caused by the specific mutation involved in the allele dosage, and it can be variable on unlinked modifier genes, epigenetic changes and environmental determinants. Therefore, the variant either does not fully explain the patient’s phenotype or its pathogenicity cannot be conclusively determined[16]. Recent advances in multi-omics and functional genomics suggest that phenotypically distinct RDs may share an underlying pathophysiology at the cellular level, leaving space for platform-based therapeutic development[17]. Some examples of analyses on the genotype-phenotype relationship and their challenges were performed by the Solve-Rare Diseases (SOLVE-RD) consortium[18].
Unpredictable evolution of rare diseases
RDs have a limited documentation of underlying pathophysiology and understanding of disease progression patterns. A general RD feature is that it relies on precise genetic characterisation, such as genetic variant identification. Undiagnosed and under-researched RDs have a high mortality rate, often increased by the absence of common advanced genetic sequencing diagnostic techniques or relevant therapies. The scarcity of the affected RD population makes it difficult to conduct traditional large-scale clinical trials that could validate the efficacy and safety of new treatments. This has demonstrated that RDs constitute a public health emergency, highlighting the urgent need for regulatory action, and for the development of novel alternative approaches for prevention and treatment[19]. Once a delivery platform has been made available for one gene therapy, it might be rapidly used for a newly discovered RD or emerging virus. A paradigm illustration is the lengthy development, for treating RD hereditary transthyretin amyloidosis, of lipid nanoparticles (LNPs) used as delivery vehicles of small interfering RNAs (siRNAs) or antisense oligonucleotides. This delivery platform took more than 10 years to develop, but it represented a “ready-to-use” formulation solution for other RNA drugs, such as messenger RNA (mRNA) genetic vaccines against emerging viruses. Thus, common technological platforms utilised for both newly discovered RDs and emerging viruses represent an integral aspect of timely medical intervention in each case[13].
It warrants special mention, however, that the LNP formulation used for hereditary transthyretin amyloidosis may be valid only for genetic diseases that primarily affect the liver and whose pathophysiological mechanisms make them susceptible to RNA interference or gene editing using CRISPR/Cas9 (clustered regularly interspaced short palindromic repeats/CRISPR-associated protein 9). These include diseases caused by a dominant-negative mutation in a liver gene. Different vector technologies and routes of administration for specific target tissues and cells should be standardised and validated to address the diversity of genetic diseases. This leads to the important concept of establishing international alliances and funding programmes, not only for vector design, but also for validation of the thousands of different gene-specific products that are needed to offer a solution to the patients in need.
Multistakeholder collaborations
One trend that the recent coronavirus pandemic demonstrated is the interconnectedness and interdependence of the multi-sectoral collaborations for the implementation and coordination of an effective systemic response. Often referred to as collaborative health emergency preparedness, this approach combines political actions with a multistakeholder alliance for achieving the health outcomes and strengthens the response capabilities[20].
One such model that centrally drove the development of medical countermeasures during the coronavirus pandemic was Operation Warp Speed (OWS), launched by the US federal government in May 2020—an initiative that helped accelerate the manufacturing scale-up of vaccines, ensuring they were widely available shortly after receiving emergency use authorisation[21].
A warp speed initiative for rare diseases?
An OWS-like initiative could represent an essential step forward in addressing RDs as a public health emergency. As approximately 95% of RDs do not benefit from an approved treatment protocol, the diagnostic process is generally delayed or focused only on symptomatic care, consequently deepening the challenges and pressure on health care services[1]. While several initiatives have analysed areas of action where funding can add the most value (e.g., optimising translational research infrastructures, modernising clinical trial design, or creating databases that ensure interoperability, data quality, and robustness), barriers still exist when moving from recommendations to real-world implementation, as well as in ensuring long-term sustainability and reliability. These challenges are particularly evident when faced with lower investor interest or an unclear commercialisation pathway. In this context, raising community awareness, complemented by open and transparent communication with policymakers on the advantages of reducing overall treatment and care expenditure by investing in next-generation diagnostic technologies and additional profiling methods, represents a critical step. This is essential for prioritising RDs on the global health agenda.
Other models of collaborations for drug development
The rapid development of therapies during pandemics demonstrated what could be achieved in a short timespan when faced with a health crisis. The accelerated growth of effective medicines when a public-private partnership is initiated by the governments and industry, doubled by coordinated efforts to enable faster production and approval of treatments, remains a viable model for application in real-world settings. Developing a public-private partnership similar to OWS could have a profound effect on accelerating RDs' diagnostic and therapeutic development[22]. Despite the adoption of legislative frameworks for action in several countries intended to stimulate orphan drug development, further efforts are required to accelerate therapeutic innovation. These include providing greater regulatory flexibility during the approval process, as demonstrated by the US Food and Drug Administration (FDA) Rare Diseases Innovation Hub, which has called for global regulatory action.
In 2023, over half of all novel drugs and biologics approved by the FDA’s Center for Drug Evaluation and Research (CDER) and Center for Biologics Evaluation and Research (CBER) were intended to prevent, diagnose, or treat RD conditions. As stated above, the success of the RD drug discovery paradigm is poised to move forward by capitalising on the unprecedented opportunity from advances in a range of approaches from RNA therapeutics, to gene therapy, genome editing, and other technologies. When combined with the urgent drive and needs of PLWRD and their families, this creates a powerful nexus for change[23,24].
In the case of RDs, the regulatory flexibility could include a greater utilisation and adaptation of therapeutic platforms such as oligonucleotide therapies, gene therapy, and genome editing. In this context, the FDA’s CDER and CBER are piloting an OWS approach to novel drugs and biologics for RDs, dubbed Support for clinical Trials Advancing Rare disease Therapeutics (START), reflecting an appreciation of the urgent need for a more flexible regulation of RD treatment[25,26]. While the START pilot programme is an important milestone in accelerating the pace of therapeutic development, it is currently limited to rare neurological conditions (CDER) and gene or cellular therapy (CBER). It addresses unmet medical needs for serious conditions that are likely to lead to disability or death within the first decade of life. The START programme also incorporates elements of OWS, namely, enhanced communication between participating companies or sponsors and the FDA regarding clinical development, clinical study design, study populations, and the approval process. However, it does not provide financial assistance to partners to cover costs associated with the development of new therapies.
Furthermore, the Rare Disease Moonshot[27], with partners including the Critical Path Institute (C-Path) in the USA and Rare Disease Moonshot Australia, is driving forward RD drug development through public–private partnerships and, similarly to the 5-Voices collaboration representing the patient community, sponsors, funders, regulators, and payers, it is working towards coordinated and integrated processes to optimise the product lifecycle for greater efficiency, speed, and scale.
Development of telehealth and data sharing
Addressing a grand global health challenge
Undoubtedly, addressing the global grand challenge of RDs requires a response covering the full range of intervention points, from prevention to screening, diagnosis, physical, mental, and social care, medical and cross-sector care coordination, trials, and treatments. The therapeutic enablers and accelerators applied when addressing public health priorities, coupled with the nature and collective magnitude of RDs, could provide unique opportunities for therapeutic transformation. The time is now—set of recommendations [Table 1].
Time is now. Set of recommendations
| A warp speed initiative for rare diseases is required | • Flexibility applied to COVID-19 highly relevant to RDs • RDs are a public health emergency |
| The time is now | • Building on the RD Moonshot in the EU and now Australia, and calls for a concerted approach in the US, we should go to a Global Warp Speed initiative |
| What is needed | • Community awareness, political will, adequate funding, regulatory flexibility |
| Tools accelerated by COVID-19 | • Data sharing (privacy preserving) through record linkage • Global clinical trial networks • Distributed/regional manufacturing • Delivery platform for n-of-1 therapies |
| Tools we didn’t have before | • Advanced therapeutics • Therapeutic platforms |
In response to persistent gaps, an important step is to enhance evidence-based health systems and highlight key context-specific barriers that prevent equitable health access. A global framework and action plan could build on trans-border cooperation and support the development of local research capacities, improve access to existing treatments, and promote innovative service delivery models (based on examples from other regions/countries) and digital tools.
Noting that awareness and knowledge of RDs is generally low across all social sectors, the availability of treatments does not guarantee accessibility for all.
A RD-focused strategy, backed up by new technologies, platforms, and policy and regulatory approaches inspired by those developed at a faster pace during pandemics, can address some of the unmet needs of RDs globally[19]. In recent years, there has been growing concern about resource allocation for people living with RDs, and about what mechanisms are in place to ensure equitable and fair distribution between rare and common diseases. Faced with persistent coverage gaps, particularly in LMICs, the use of digital health applications and services promises improved effectiveness, equity, and reach. Artificial intelligence applications, mobile tools, virtual consultations, and teleconsulting could help deliver faster and more equitable services, opening new frontiers for expanding access to health support for PLWRD and reducing administrative burden[28] [Table 2].
Recommendations on the management of RD as a public health priority through coordinated actions
| Start by using what is ready available locally – A formal declaration should be adopted to legitimize the use of existing regulatory flexibility; creation of a governing structure, responsible for coordinated and equitable execution |
| Global and national health prioritization like other high burden conditions, e.g. cancer, COVID-19, Alzheimer’s |
| Large scale, sustained funding to build and maintain infrastructure, from diagnostics to clinical trial networks |
| Addressing the invisibility of PLWRD – patients need to benefit from an easier identification system through shared infrastructures |
| Education and training for physicians, nurses, public / patient academy, combating stigma and disinformation - telemedicine for spreading expertise - “care across borders” |
In the context of pandemics, health injustice becomes more visible and is usually amplified through pre-existing social, economic, racial, and ethnic disparities. The World Health Organisation (WHO) defines access to health and care as a human right, essential for people living with RDs[29]. The COVID-19 pandemic highlighted how all the elements of care are intrinsically intertwined [Table 3]. Nonetheless, there are big differences when comparing worldwide epidemics and RD conditions, e.g., in terms of achieving a diagnostic, appropriate disease management and treatment. While COVID-19 is easily diagnosed through a simple, accessible kit, available almost everywhere in the world, for RDs, diagnostic assessments usually require in-depth testing by a team of expert medical providers. The therapeutic management for COVID-19 usually follows panel recommendations based on the disease severity and factors such as comorbidities and age, but in general, mild or moderate cases recover with minimal interventions[30]. Compared to RDs, despite significant progress in recent years, it is estimated that only 5% of RDs have approved treatments. Under current paradigms, these could be improved through insights, platforms and process improvements surfaced and accelerated by pandemic responses.
What we learned from COVID-19 (and COVID-19 from RDs) - similarities between responding to the COVID-19 pandemic and the needs of PLWRDs, based on the 10 essential elements of public health[24]
| Essential element | COVID-19 response | Rare disease response |
| Monitor health status | Track cases, deaths, hospitalizations, and variants. Use of GIS (e.g. ArcGIS) technology to spatially map COVID-19.[24] | Collect data on prevalence, incidence, diagnosis, and outcomes. Use of ArcGIS to map rare diseases. Note also ArcGIS processes have also been adapted to support genomic data sharing for RD diagnosis |
| Diagnose and investigate | Test, trace, and isolate cases and contacts | Improve access to genetic testing, counseling and family and cascade testing |
| Inform, educate, and empower | Provide clear and consistent communication and guidance | Raise awareness and advocate for the rights and needs of PLWRD |
| Mobilize community partnerships | Engage with civil society, private sector, and media | Connect with patient organizations, expert centers, and researchers |
| Develop policies and plans | Implement public health measures and vaccination strategies | Develop national plans and policies for rare diseases |
| Enforce laws and regulations | Ensure compliance with health protocols and restrictions | Protect the interests and privacy of PLWRD |
| Link to/provide care | Ensure access to health services and social support | Establish care pathways and referral systems |
| Assure competent workforce | Train and equip health workers and volunteers | Build capacity and expertise among health professionals |
| Evaluate health services | Monitor and evaluate the effectiveness and impact of interventions | Assess the quality and outcomes of care and services |
| Research for new insights | Support innovation and collaboration for new diagnostics, treatments, and vaccines | Promote research and development for rare diseases |
SUMMARY
Recent actions have sought to improve the quality of life of PLWRD and their families, but despite this, inequalities are still globally pervasive in terms of early and precise diagnosis and care. Optimised diagnostics methods can provide a portal to strengthen disease management strategies and care pathways, reducing the burden on health care systems and society, thus enabling better health outcomes. While the RD drug development market remains less economically attractive compared with other diseases, several lessons from public health measures could be prioritised to improve the recognition and visibility of RDs and support the creation of a strategic development plan that reduces global fragmentation and inequality. The COVID-19 pandemic has shown the world the multifaceted challenges experienced by RD patients when faced with a lack of diagnostic methods, medications, and care; however, it has also inspired the adoption of several measures, such as the rapid adoption of telemedicine, expedited drug approvals, data-sharing paradigms, and strengthened international collaboration for priority setting and risk management. These considerations could promote research and global coalitions as an action model for addressing the needs and challenges of the RD population.
DECLARATIONS
Author’s contributions
Made substantial contributions to conception and design of the study and performed data analysis and interpretation, wrote the first draft of the paper and contributed to the revision and finalisation of the paper: Baynam G, Akli RD, Pariser AR, Chan CH, Tataru EA, Scherman D, Pearce DA
Availability of data and materials
Not applicable.
AI and AI-assisted tools statement
Not applicable.
Financial support and sponsorship
The IRDiRC Working Group on Parallels between COVID-19 and Rare Diseases was supported by the Scientific Secretariat of IRDiRC. The Scientific Secretariat is funded by the European Union’s Horizon Europe research and innovation programme through the European Rare Diseases Research Alliance (ERDERA), under grant agreement No. 101156595. The Scientific Secretariat is hosted by the Foundation for Rare Diseases (FFRD) in Paris, France.
Conflicts of interest
Scherman D is Editor-in-Chief of the journal Rare Disease and Orphan Drugs Journal. Pearce DA is an Editorial Board Member of the journal Rare Disease and Orphan Drugs Journal. Scherman D and Pearce DA were not involved in any steps of editorial processing, notably including reviewers' selection, manuscript handling or decision-making; Akli RD is an independent consultant based in Bryn Mawr, USA. Tataru EA and Scherman D are associated with the Fondation Maladies Rares, Paris, France. All authors are associated with the International Rare Diseases Research Consortium (IRDiRC), Paris, France.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
The Author(s) 2026
REFERENCES
2. Rare Diseases at FDA 2024. Available from: https://www.fda.gov/patients/rare-diseases-fda#whatisraredis [Last accessed on 22 Apr 2026].
3. What is a rare disease. Available from: https://www.eurordis.org/fr/what-is-a-rare-disease/ [Last accessed on 22 Apr 2026].
4. KEI briefing note 2020: 4 selected governament definitions of orphan or rare diseases. Available from: https://www.keionline.org/bn-2020-4 [Last accessed on 22 Apr 2026].
5. Rare Diseases. Available from: https://www.sciensano.be/en/health-topics/rare-diseases [Last accessed on 22 Apr 2026].
6. Ali S, Archer L, Jensen EL. COVID-19 and health equity: lessons learned from the pandemic. 2024. Available from: https://scholarsarchive.byu.edu/cgi/viewcontent.cgi?article=1126&context=joni [Last accessed on 22 Apr 2026].
7. World Health Organization. Seventy-eighth World Health Assembly - Daily update: 24 May 2025. Available from: https://www.who.int/news/item/24-05-2025-seventy-eighth-world-health-assembly---daily-update--24-may-2025 [Last accessed on 26 May 2026].
8. European Reference Networks. Available from: https://health.ec.europa.eu/rare-diseases-and-european-reference-networks/european-reference-networks_en [Last accessed on 22 Apr 2026].
9. What is rare disease day? Available from: https://www.rarediseaseday.org/what-is-rare-disease-day/ [Last accessed on 22 Apr 2026].
10. Undiagnosed Diseases Network. Available from: https://undiagnosed.hms.harvard.edu/ [Last accessed on 22 Apr 2026].
11. Andreu P, Karam J, Child C, Chiesi G, Cioffi C. The burden of rare diseases: an economic evaluation. Available from: https://chiesirarediseases.com/assets/pdf/chiesiglobalrarediseases.whitepaper-feb.-2022_production-proof.pdf [Last accessed on 22 Apr 2026].
12. Navarrete-Opazo AA, Singh M, Tisdale A, Cutillo CM, Garrison SR. Can you hear us now? The impact of health-care utilization by rare disease patients in the United States. Genet Med. 2021;23:2194-201.
13. van Doorn HR. The epidemiology of emerging infectious diseases and pandemics. Medicine. 2021;49:659-62.
14. Mazzucato M, Visonà Dalla Pozza L, Minichiello C, Toto E, Vianello A, Facchin P. Estimating mortality in rare diseases using a population-based registry, 2002 through 2019. Orphanet J Rare Dis. 2023;18:362.
15. McNeill A. Good genotype-phenotype relationships in rare disease are hard to find. Eur J Hum Genet. 2022;30:251.
16. Cooper DN, Krawczak M, Polychronakos C, Tyler-Smith C, Kehrer-Sawatzki H. Where genotype is not predictive of phenotype: towards an understanding of the molecular basis of reduced penetrance in human inherited disease. Hum Genet. 2013;132:1077-130.
17. Rao A, Yabumoto M, Ward-Lev E, et al. Health-related quality of life in patients with diverse rare diseases: an online survey. Genet Med Open. 2024;2:101889.
18. Laurie S, Steyaert W, de Boer E, et al. Genomic reanalysis of a pan-European rare-disease resource yields new diagnoses. Nat Med. 2025;31:478-89.
19. Gu Y, Wang A, Tang H, et al. Comparison of rare and common diseases in the setting of healthcare priorities: evidence of social preferences based on a systematic review. Patient Prefer Adher. 2023;17:1783-97.
20. Gillmore JD, Gane E, Taubel J, et al. CRISPR-Cas9 in vivo gene editing for transthyretin amyloidosis. N Engl J Med. 2021;385:493-502.
21. Akenroye TO, Abubakre A, Elbaz J, et al. Modeling the barriers to multistakeholder collaboration for COVID-19 pandemic response: evidence from Sub-Saharan Africa. Int Public Manag J. 2021;25:192-216.
22. O'Leary CN, Barnes-Weise J, Hoyt K, Bourdeaux M. Maintaining warp speed: policy requirements for a just-in-time, capability-based, scalable medical countermeasure research and development enterprise. Health Secur. 2023;21:272-9.
23. FDA rare disease innovation hub to enhance and advance outcomes of patients. Available from: https://www.fda.gov/news-events/fda-voices/fda-rare-disease-innovation-hub-enhance-and-advance-outcomes-patients [Last accessed on 22 Apr 2026].
24. Gahl WA. The battlefield of rare diseases: where uncommon insights are common. Sci Transl Med. 2012;4:154ed7.
25. Kokudo N, Sugiyama H. Call for international cooperation and collaboration to effectively tackle the COVID-19 pandemic. Glob Health Med. 2020;2:60-2.
26. U.S. Food and Drug Administration. Support for clinical trials advancing rare disease therapeutics (START) pilot program. Available from: https://www.fda.gov/science-research/clinical-trials-and-human-subject-protection/support-clinical-trials-advancing-rare-disease-therapeutics-start-pilot-program [Last accessed on 22 Apr 2026].
27. The Rare Disease Moonshot 2024. Available from: https://www.rarediseasemoonshot.eu [Last accessed on 22 Apr 2026].
28. Tumienė B, Juozapavičiūtė A, Andriukaitis V. Rare diseases: still on the fringes of universal health coverage in Europe. Lancet Reg Health Eur. 2024;37:100783.
29. Jonker AH, Cavaller-Bellaubi M, Nishimura Y, Pearce DA. Access in the rare diseases landscape. Lancet Global Health. 2024;12:e1587.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].