


A look from a distance on patent foramen ovale closure
 0
0 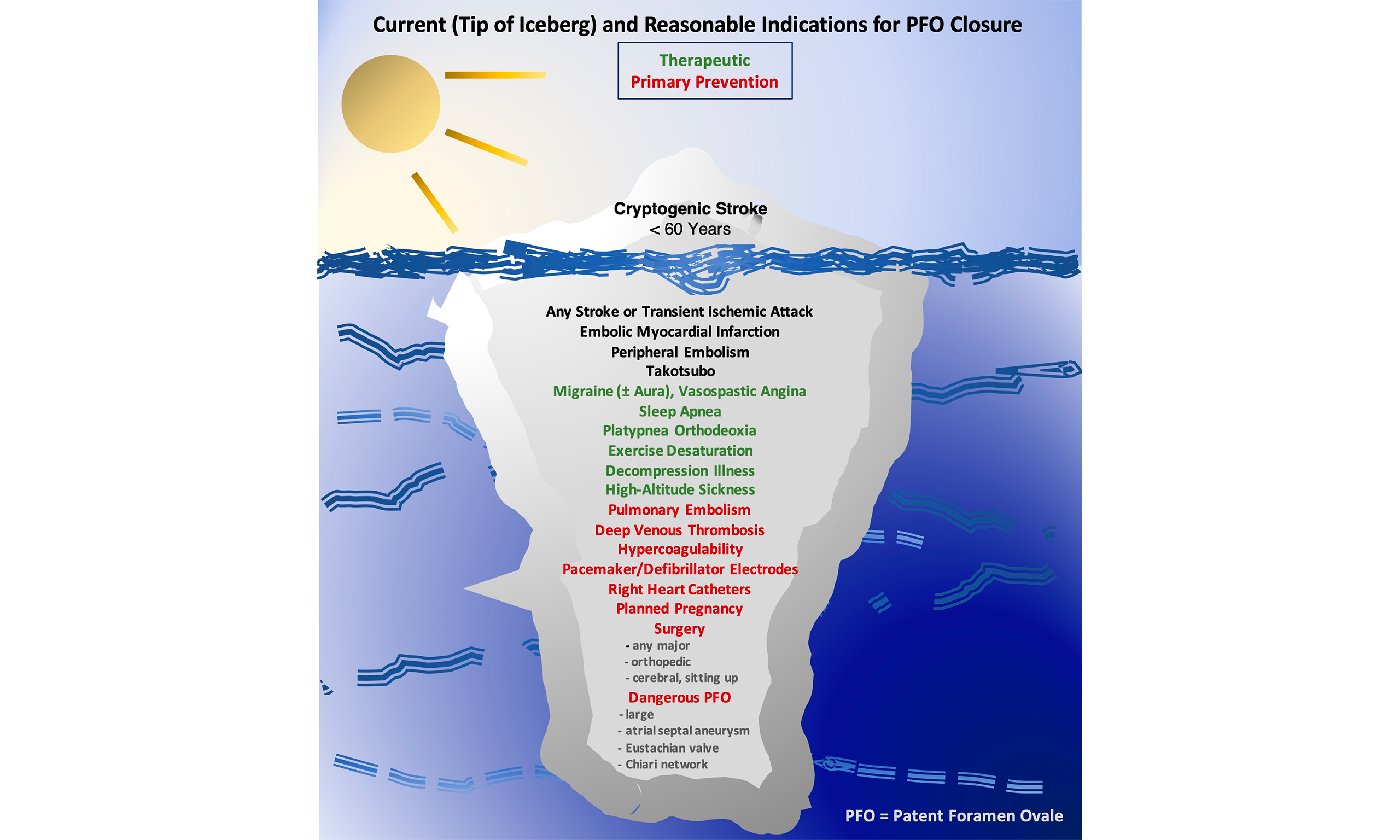
Current situation of patent foramen ovale closure
Device closure of the patent foramen ovale (PFO) has been around but highly underused for over 30 years. It likely represents the catheter-based procedure in interventional cardiology with the best overall yield regarding benefit and adverse events[1].
It is easier to perform and safer than all other therapeutic or preventive nonsurgical cardiac interventions. It prevents death, ischemic cerebral events, myocardial infarction (MI), peripheral ischemic problems, Takotsubo episodes, and coronary spasm[1]. It ameliorates or cures migraine, sleep apnea, platypnea orthodeoxia, and exercise desaturation. It eliminates an aggravating factor for decompression illness and high altitude pulmonary or cerebral edema. Most notably, you close a PFO for one reason and, as a collateral benefit, you harvest all the other protective and therapeutic effects with no further ado.
Indications for PFO closure
Currently, published guidelines limit the indication for PFO closure to patients with a prior ischemic cerebral event who are younger than 60 years (graphic abstract). Evidence-based medicine is the background of this likely unfavorable restriction. Only for such patients there are irrevocable data from randomized trials proving a statistically significant benefit in preventing further ischemic cerebral events. Randomized trials in older patients (particularly those with-high-risk anatomical features[2]), regarding primary prevention[3], or for all other indications mentioned above (migraine excepted) are lacking. Keep in mind, the absolute risk of the PFO in old people is particularly high[4] because age and disease beget venous thrombosis[5], the major prerequisite for the PFO to do harm.
The randomized trials of PFO closure for migraine missed the statistical significance in their individual primary endpoints. They all showed a numerical benefit of PFO closure regarding persistence or frequency of migraine, and practically all their secondary endpoints were statistically significant[1]. Yet, evidence-based medicine irrationally concluded that PFO closure should not be performed for migraine treatment. This blatantly ignores that PFO closure clearly improves migraine in comparison with continuation of medical treatment and that PFO closure for migraine automatically vaccinates people mechanically for life against paradoxical embolism causing death, stroke, or MI, etc. By the way, the blood distribution defines that for every 3 strokes by paradoxical embolism, there will be 1 MI. In China, the importance of the direct and collateral benefit of PFO closure for migraine has been recognized, and PFO closure for migraine has been established as an indication for PFO closure. The rest of the world has yet to follow that laudable example.
Many arguments have been raised against a more widespread application of PFO closure. The concern that a cardiac intervention is always perilous and should only be performed with a sound reason can be easily annihilated. PFO closure may be performed in less than 15 min in an awake patient who can leave the hospital a couple of hours later and engage in sports or any other activity the very same day. The only medication routinely prescribed is a platelet inhibitor for a few months until the device is endocardialized. Even that has not been proved to be really necessary. Device thromboses with the market leader devices under platelet inhibitors are extremely rare (less than 0.5% and most of them clinically silent). Perhaps, they would be equally infrequent without any treatment, as was the common approach 30 years ago. Endocarditis because of the device has yet to be reported. Prophylaxis against endocarditis is recommended by some operators but only for the initial months after implantation. The only relevant complication is erosion of a free atrial wall by the device. However, its occurrence is so rare that it is not a significant concern. The device will not block transseptal access for later left atrial intervention. The device is a fluoroscopic marker for transseptal puncture at its lower rim for a caudal left atrial access (ideal for ablation for atrial fibrillation (AF) or closure of the left atrial appendage (LAA) for stroke prevention in AF) or alongside its border for a postero-cranial access (required for mitral clipping). AF may be triggered initially by the device, but persisting AF requiring stroke prevention only happens because of PFO closure in patients already at the brink of AF before the procedure.
PFO closure represents a mechanical vaccination for life
The paper of a Canadian group of interventional cardiologists, “Twenty-year follow-up after patent foramen ovale closure in patients with paradoxical embolism”[6] is welcome to prove once and for all that, at least up to 20 years, there are no late problems to be feared with PFO closure, entailing a permanent implant of an only partially resorbable device that is constructed with nitinol containing nickel. For what happens after 20 years, age is much more important than any 20-year-old so far silent implant.
The paper reports on 130 patients (67 women and 63 men, mean age 46 years) with PFO closure at least 20 years ago and a 96% follow-up rate. With about 30 PFO closures per year during the inclusion period, the reporting centers were not high-volume centers. Their results should be reproducible by any reasonably experienced operator. The only periprocedural problems were 1 paroxysmal AF and 1 esophageal hematoma due to the intraoperative transesophageal echocardiography (TEE, used in all patients). No patient died acutely or during follow-up because of PFO closure. One stroke, due to documented vertebral artery dissection (0.04% per year), and 6 transient ischemic attacks (0.25% per year) occurred, predominantly in patients with thrombophilia that was screened for in 82% and present in 6%, i.e., 33% in patients with ischemic events and 5% in those without.
The authors learned from their study that the only significant procedural complication occurred due to the, according to the vast experience in fluoroscopy-only procedures[1], unnecessary guidance with TEE. They do not divulge whether they subsequently abandoned TEE guidance, which prolonged their procedures, created the only relevant complication, and subjected an additional person (TEE operator) to an X-ray exposure higher than that of the operator[7].
The authors learned from their study that their recommendation to permanently pursue some kind of blood thinning (mostly antiplatelets) may not be recommendable. Neurologists generally recommend lifelong antiplatelets (and statins) in patients with a stroke but no obvious nonatherosclerotic reason other than a PFO. They argue that the PFO can only be surmised as a culprit. They appear to forget that this also holds true for patients with a stroke in the realm of AF. They also overlook that a young and otherwise healthy person with a stroke and a PFO simply does not have atherosclerosis, the target of antiplatelets and statins. None of the 13% bleedings during follow-up occurred in the 20% of patients who had stopped blood thinners against advice. The authors have initiated a welcome randomized trial on anticoagulation management after PFO closure to complement the scarce respective literature.
AF during follow-up occurred in about 4% of the patients, half paroxysmal and half persistent. That appears to correlate with the incidence of new-onset AF over 20 years in the general population around 50 years of age and cannot be blamed on the PFO closure. Even if such patients will require permanent oral anticoagulation, the PFO had not been closed in vain. Prior to the occurrence of AF, it replaced blood thinners as prevention against recurrent ischemic events. Thereafter, it protects against paradoxical embolism during periods of suboptimal anticoagulation (compliance) or imposed pauses. And then, there is the option of device closure of the LAA to obviate the need for oral anticoagulation.
The authors observed that the prevalence of migraine was 29% before PFO closure and 8% at the end of follow-up. The high initial percentage proves that migraine and PFO are connected. The low prevalence after 20 years cannot be sufficiently explained by the fact that migraine typically abates at older age. It must mainly be a collateral benefit of the PFO closure, in the study exclusively performed for prevention of additional ischemic events.
DECLARATIONS
Authors’ contributions
The author contributed solely to the article.
Availability of data and materials
Not applicable.
AI and AI-assisted tools statement
Not applicable.
Financial support and sponsorship
None.
Conflicts of interest
The author declared that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Meier B. A cardiologist’s perspective on patent foramen ovale-associated conditions. Cardiol Clin. 2024;42:547-57.
2. Vidal-Calés P, Llull L, Lanthier S, et al. Patent foramen ovale closure in older patients with cryptogenic stroke: current evidence and next steps. Structural Heart. 2025;9:100699.
3. Ibrahim R, Pathangey G, Pham HN, et al. Patent foramen ovale closure for primary prevention of stroke. CJC Open. 2026;8:493-7.
4. Mazzucco S, Li L, Rothwell PM. Prognosis of cryptogenic stroke with patent foramen ovale at older ages and implications for trials: a population-based study and systematic review. JAMA Neurol. 2020;77:1279.
5. Martinez C, Cohen AT, Bamber L, Rietbrock S. Epidemiology of first and recurrent venous thromboembolism: a population-based cohort study in patients without active cancer. Thromb Haemostasis. 2014;112:255-63.
6. Vidal-Calés P, Houde C, Battistolo Q, et al. Twenty-year follow-up after patent foramen ovale closure in patients with paradoxical embolism. JAMA Cardiol. 2026;11:383.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0











Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].