


Association between postoperative obesity and recurrence after radiofrequency catheter ablation in patients with atrial fibrillation
 0
0 Abstract
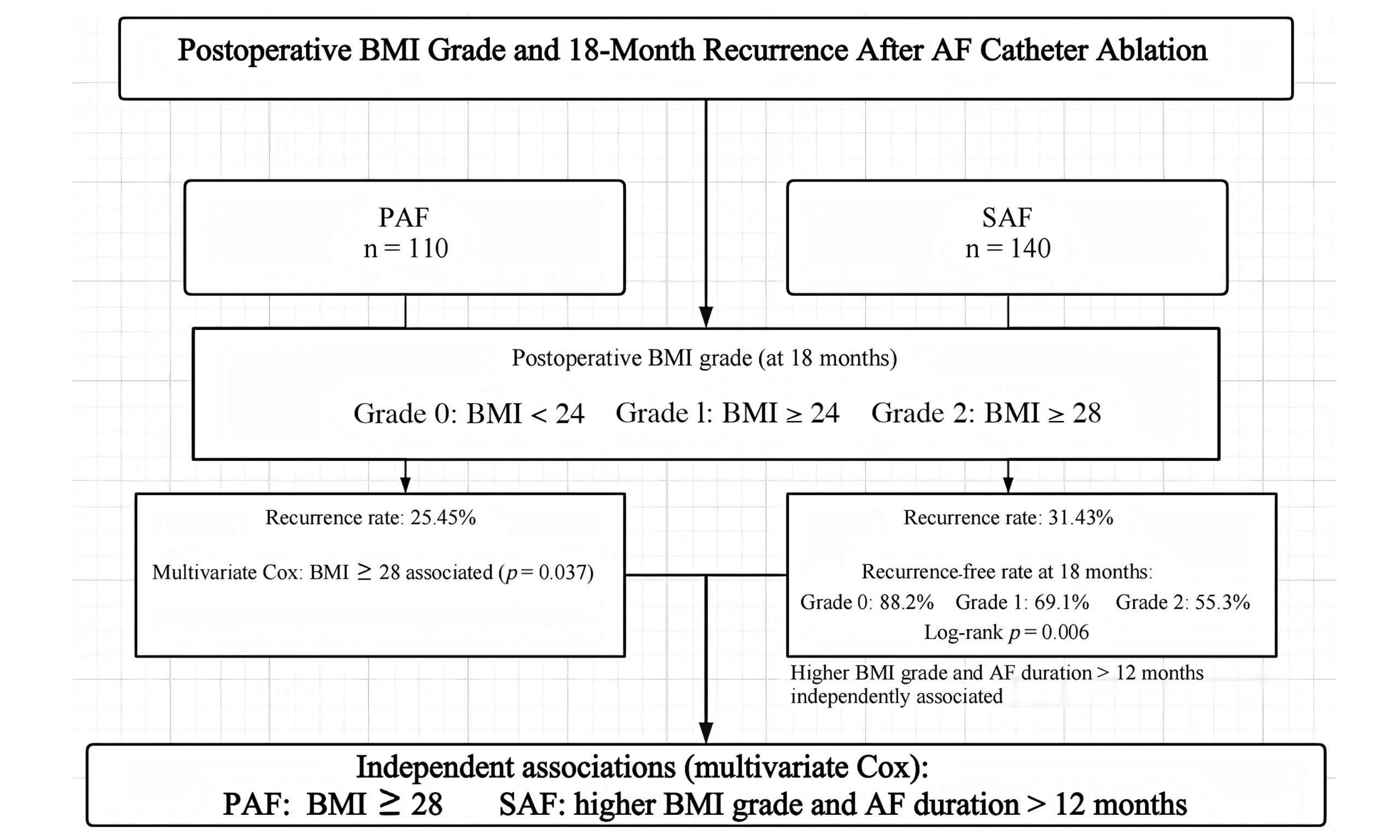
Aim: This study evaluated the association between postoperative body mass index (BMI) category at the 18 months postoperative follow-up and atrial fibrillation (AF) recurrence after radiofrequency catheter ablation (RCA).
Methods: From January to December 2023, 250 patients with AF who underwent single-operator RCA at the General Hospital of Northern Theater Command were enrolled. Baseline characteristics, BMI category at the 18 months postoperative follow-up (normal weight, overweight, obesity), and recurrence were collected. Kaplan-Meier survival analysis and multivariate Cox proportional hazards analysis were performed. The primary endpoint was AF recurrence confirmed by electrocardiogram (ECG) or Holter monitoring within 18 months.
Results: Among 110 patients with paroxysmal atrial fibrillation (PAF) and 140 patients with persistent atrial fibrillation (SAF). Multivariate Cox analysis showe
Conclusion: In this retrospective analysis, postoperative obesity was associated with a higher risk of recurrence after RCA for AF. Specifically, postoperative obesity was associated with recurrence in patients with PAF, whereas higher postoperative BMI grades and AF duration > 12 months were associated with recurrence in patients with SAF.
Keywords
INTRODUCTION
Atrial fibrillation (AF) is one of the most common clinical arrhythmias worldwide, and its prevalence continues to increase. AF substantially impairs patients’ quality of life and increases the risk of adverse cardiovascular events, including stroke and heart failure[1]. Obesity is a major global public health concern and has been identified in numerous studies as a substantial modifiable risk factor for the development and progression of AF. The underlying mechanisms encompass epicardial adipose tissue-mediated inflammation, atrial structural remodeling, and hemodynamic alterations[2,3]. Furthermore, obesity-related comorbidities, such as hypertension and obstructive sleep apnea, contribute to the initiation and maintenance of AF[4]. Radiofrequency catheter ablation (RCA) has become a cornerstone therapy for AF, with demonstrated benefits in improving quality of life, reducing hospitalization, and potentially improving cardiovascular outcomes[5]. Given the increasing number of patients with obesity undergoing this procedure[6], evaluating the impact of obesity on procedural safety, efficacy, and post-ablation recurrence is important. However, current evidence regarding the influence of obesity on AF recurrence after RCA remains inconsistent. Some studies have reported that obesity does not affect RCA success rates[7,8], whereas others have reported a higher recurrence risk in patients with obesity[9,10].
Previous research has predominantly focused on the prognostic impact of baseline body mass index (BMI), whereas the effect of postoperative BMI on AF recurrence remains unclear. Therefore, this study investigated the association between postoperative BMI and recurrence after RCA in patients with AF, to inform comprehensive postoperative management and individualized treatment strategies.
METHODS
Study design and participants
A retrospective analysis of 276 patients with AF who underwent single-operator RCA at the General Hospital of Northern Theater Command between January and December 2023 was conducted. The study population consisted of consecutive patients treated by the same operator in 2023. The inclusion criteria were as follows: (1) RCA was performed by a single operator, Ming Liang; (2) AF was confirmed by electrocardiogram (ECG) or Holter monitoring; and (3) patients met the indications for RCA and successfully underwent the procedure. Twenty-six patients were excluded for the following reasons: incomplete postoperative ECG or Holter monitoring (n = 0), missing baseline data (n = 20), missing 18 months postoperative BMI or recurrence data (n = 4), and severe valvular heart disease (n = 2). Paroxysmal atrial fibrillation (PAF) was defined as AF episodes lasting < 7 days with spontaneous conversion to sinus rhythm; persistent atrial fibrillation (SAF) was defined as episodes lasting ≥ 7 days or requiring medical intervention for conversion[11]. Patients were categorized by AF type into the SAF group (n = 140) and the PAF group (n = 110). The duration of persistent AF was assessed using ECG or 24 h Holter monitoring records. Pulmonary vein isolation was performed by a single operator in all patients. Clinical data were extracted from the hospital’s electronic medical record system.
Ethical approval and consent to participate
This study was conducted in accordance with the principles of the Declaration of Helsinki. The study protocol was reviewed and approved by the Ethics Committee of the General Hospital of Northern Theater Command [Approval No. Y (2025) 529]. The requirement for informed consent was waived by the institutional review board given the retrospective design and complete anonymization of all patient data.
Surgical procedure
Preoperative transesophageal echocardiography was routinely performed to assess for thrombus. Antiarrhythmic medications were discontinued for at least five half-lives before the procedure. Electrophysiological studies and ablation procedures were performed under fentanyl-assisted conscious sedation. In brief, two right femoral venous accesses with 8.5-F sheaths were used for transseptal puncture. After transseptal puncture, intraoperative heparinization was used to maintain an activated clotting time of 300-350 s. A 10-pole catheter was inserted into the coronary sinus via the left femoral or right jugular venous access. The left atrium was mapped using a 20 mm 10-pole circular or adjustable curved mapping catheter to establish a three-dimensional model of the left atrium. A 3.5 mm open-tip irrigated ablation catheter was used to ablate the right pulmonary vein antrum first, followed by the left pulmonary vein antrum. Radiofrequency energy was delivered in a wide-area circular pattern within 0.5-1.5 cm of the corresponding pulmonary vein ostium. Ablation parameters included radiofrequency energy of 35-40 W, contact force of 5-15 g, and impedance of 120-140 ohms. The target ablation index was 360-380 for the posterior wall and 400-420 for the anterior wall. A circular or PentaRay catheter was then placed in each of the four pulmonary veins to confirm isolation. If isolation was incomplete, additional ablation was performed as needed. Intravenous isoproterenol was administered to induce non-pulmonary vein triggers. The durability of pulmonary vein isolation was confirmed 30 min after initial documentation of isolation. If AF persisted after circumferential pulmonary vein ablation, direct current cardioversion was performed to restore sinus rhythm.
Follow-up and clinical outcomes
All patients were followed at 3, 6, 9, 12, and 18 months after the procedure by telephone or outpatient visits. An ECG was recorded at each follow-up visit, and 24 h Holter monitoring was performed at the 3 and
Data collection
The initial dataset included demographic and clinical characteristics, including age, sex, preoperative BMI, left atrial diameter, serum creatinine, N-terminal pro-B-type natriuretic peptide (NT-proBNP), AF duration, left ventricular ejection fraction, hypertension, diabetes, heart failure, obstructive sleep apnea, coronary artery disease, and history of stroke. Postoperative BMI was assessed only at the 18 months follow-up (a single time point); only 18 months BMI data were complete, and interim BMI data were not analyzed because of partial missingness. Postoperative BMI was categorized using predefined cutoffs as follows: normal weight, < 24 kg/m2; overweight, 24 ≤ BMI < 28 kg/m2; and obesity, ≥ 28 kg/m2. BMI was measured in the morning after an overnight fast.
Statistical analysis
Before formal analysis, data accuracy and outliers were verified through double-entry cross-checking and review of the original medical records to ensure data integrity. The normality of continuous variables was assessed using the Shapiro-Wilk test and Q-Q plots.
Data analysis was performed using SPSS version 29.0. Continuous variables are expressed as the mean ± standard deviation or median (interquartile range). Normally distributed variables were compared using Student’s t-test, and non-normally distributed variables were compared using the Mann-Whitney U test. Categorical variables are presented as frequencies (n) and percentages (%) and were analyzed using the chi-squared test or Fisher’s exact test, as appropriate. The Kaplan-Meier method was used to estimate recurrence-free survival during follow-up, and survival distributions were compared using the log-rank test. Multivariate Cox regression was performed to examine the association between postoperative BMI category and recurrence, with adjustment for potential confounders including age, sex, left atrial diameter, left ventricular ejection fraction (LVEF), AF duration > 12 months, and comorbidities (hypertension, diabetes, heart failure, obstructive sleep apnea, coronary artery disease, and stroke). Variables were selected for the multivariate model based on univariate analysis (P < 0.10) and clinical relevance. A two-sided P < 0.05 was considered statistically significant.
RESULTS
As shown in the flowchart [Figure 1], 250 patients diagnosed with AF between January and December 2023 were included in the final analysis; 110 were classified as PAF and 140 as SAF. Baseline characteristics are shown in Table 1 for patients with PAF and Table 2 for those with SAF. No significant differences in baseline characteristics were observed between the recurrence and non-recurrence groups among patients with either PAF or SAF.
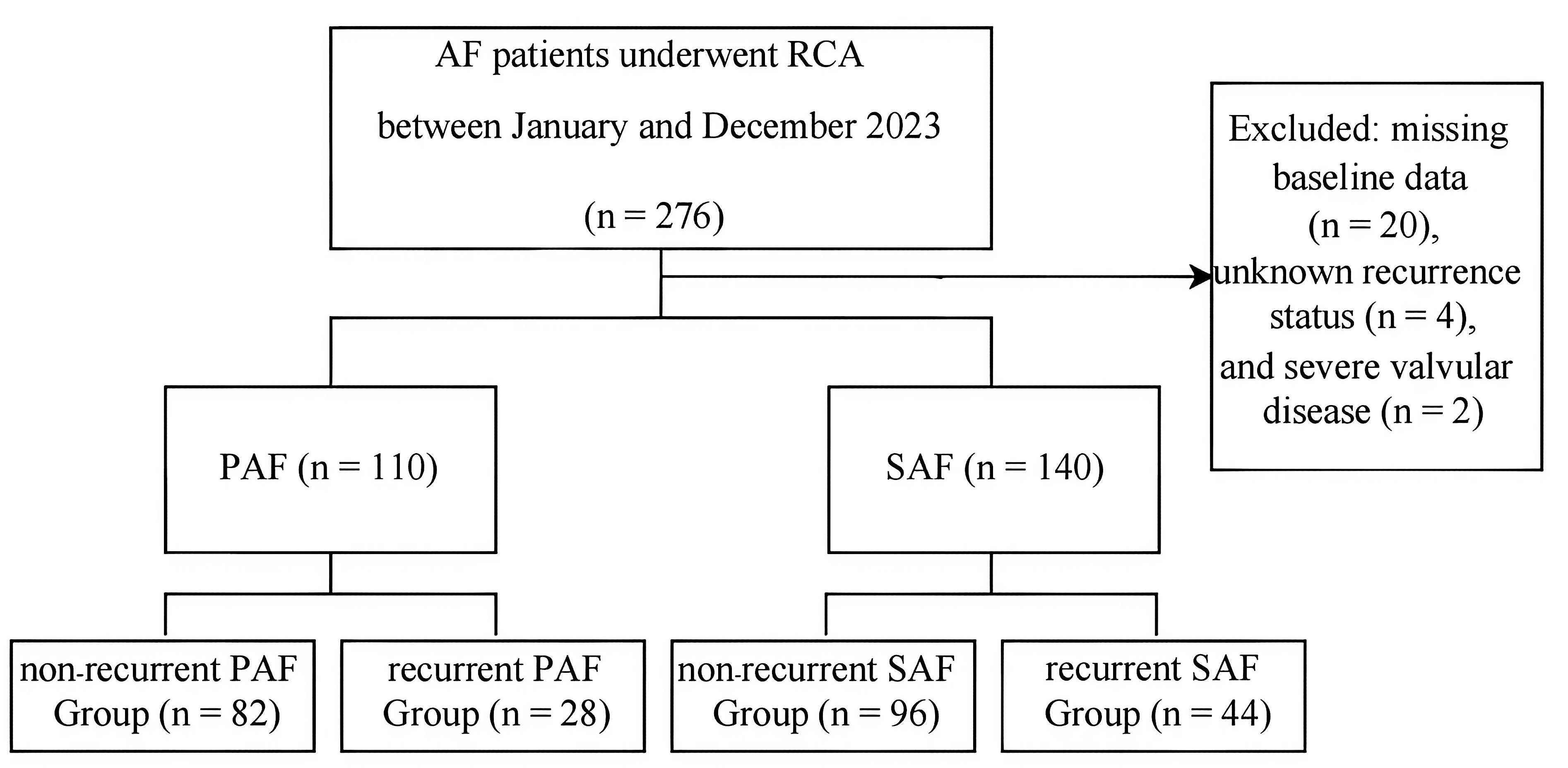
Figure 1. Flowchart of patient enrollment and inclusion in the analysis. PAF: Paroxysmal atrial fibrillation; AF: atrial fibrillation; SAF: persistent atrial fibrillation; RCA: radiofrequency catheter ablation.
Baseline characteristics of the PAF group
| Variables | Total (n = 110) | No recurrence (n = 82) | Recurrence (n = 28) | Statistic | P |
| Age, years | 62.50 (55.00, 67.75) | 63.00 (55.00, 67.75) | 60.00 (56.00, 67.25) | Z = -0.35 | 0.726 |
| Male | 71 (64.55) | 52 (63.41) | 19 (67.86) | χ2 = 0.18 | 0.671 |
| Preoperative BMI, kg/m2 | 25.70 ± 3.19 | 25.43 ± 3.08 | 26.50 ± 3.40 | t = -1.54 | 0.126 |
| Left atrial diameter, mm | 41.74 ± 5.57 | 41.91 ± 5.97 | 41.25 ± 4.29 | t = 0.54 | 0.592 |
| Serum creatinine, mg/dL | 69.30 ± 15.73 | 70.67 ± 15.83 | 65.31 ± 15.02 | t = 1.57 | 0.120 |
| NT-proBNP, pg/mL | 441.45 (170.47, 843.55) | 415.55 (170.47, 779.45) | 700.80 (206.60, 947.10) | Z = -1.10 | 0.271 |
| Duration of AF, months | 24.00 (10.25, 72.00) | 24.00 (10.50, 60.00) | 30.00 (10.50, 72.00) | Z = -0.55 | 0.584 |
| LVEF, % | 0.58 (0.51, 0.63) | 0.57 (0.50, 0.61) | 0.59 (0.53, 0.67) | Z = -1.72 | 0.085 |
| Hypertension | 50 (45.45) | 38 (46.34) | 12 (42.86) | χ2 =0.10 | 0.749 |
| Diabetes | 13 (11.82) | 8 (9.76) | 5 (17.86) | χ2 = 0.65 | 0.419 |
| Heart failure | 27 (24.55) | 20 (24.39) | 7 (25.00) | χ2 = 0.00 | 0.948 |
| Obstructive sleep apnea | 24 (21.82) | 17 (20.73) | 7 (25.00) | χ2 = 0.22 | 0.637 |
| Coronary artery disease | 15 (13.64) | 12 (14.63) | 3 (10.71) | χ2 = 0.04 | 0.839 |
| History of stroke | 11 (10.00) | 8 (9.76) | 3 (10.71) | χ2 = 0.00 | 1.000 |
Baseline characteristics of the SAF group
| Variables | Total (n = 140) | No recurrence (n = 96) | Recurrence (n = 44) | Statistic | P |
| Age, years | 60.00 (55.00, 67.00) | 61.50 (54.00, 68.25) | 59.00 (55.75, 65.25) | Z = -1.24 | 0.214 |
| Male | 109 (77.86) | 76 (79.17) | 33 (75.00) | χ2 = 0.30 | 0.581 |
| Preoperative BMI, kg/m2 | 26.52 ± 3.21 | 26.41 ± 3.28 | 26.76 ± 3.06 | t = -0.60 | 0.548 |
| Left atrial diameter, mm | 40.45 ± 5.61 | 40.11 ± 5.55 | 41.18 ± 5.74 | t = -1.04 | 0.298 |
| Serum creatinine, mg/dL | 71.66 ± 17.14 | 71.50 ± 17.45 | 72.01 ± 16.63 | t = -0.16 | 0.871 |
| NT-proBNP, pg/mL | 341.85 (103.75, 733.05) | 337.65 (99.86, 672.05) | 352.50 (128.20, 780.75) | Z = -0.02 | 0.987 |
| Duration of AF, months | 24.00 (8.75, 60.00) | 12.00 (6.00, 48.00) | 48.00 (24.00, 87.00) | Z = -2.81 | 0.005 |
| LVEF, % | 0.57 (0.49, 0.61) | 0.57 (0.49, 0.61) | 0.57 (0.50, 0.60) | Z = -0.02 | 0.987 |
| Hypertension | 67 (47.86) | 45 (46.88) | 22 (50.00) | χ2 = 0.12 | 0.731 |
| Diabetes | 31 (22.14) | 25 (26.04) | 6 (13.64) | χ2 = 2.69 | 0.101 |
| Heart failure | 28 (20.00) | 21 (21.88) | 7 (15.91) | χ2 = 0.67 | 0.413 |
| Obstructive sleep apnea | 25 (17.86) | 16 (16.67) | 9 (20.45) | χ2 = 0.30 | 0.587 |
| Coronary artery disease | 27 (19.29) | 17 (17.71) | 10 (22.73) | χ2= 0.49 | 0.485 |
| History of stroke | 20 (14.29) | 15 (15.62) | 5 (11.36) | χ2 = 0.45 | 0.504 |
The recurrence rate in the PAF group was 25.45%. Multivariate Cox analysis showed that BMI ≥ 28 kg/m2 was associated with an increased risk of AF recurrence in this group (P = 0.037; Figure 2).
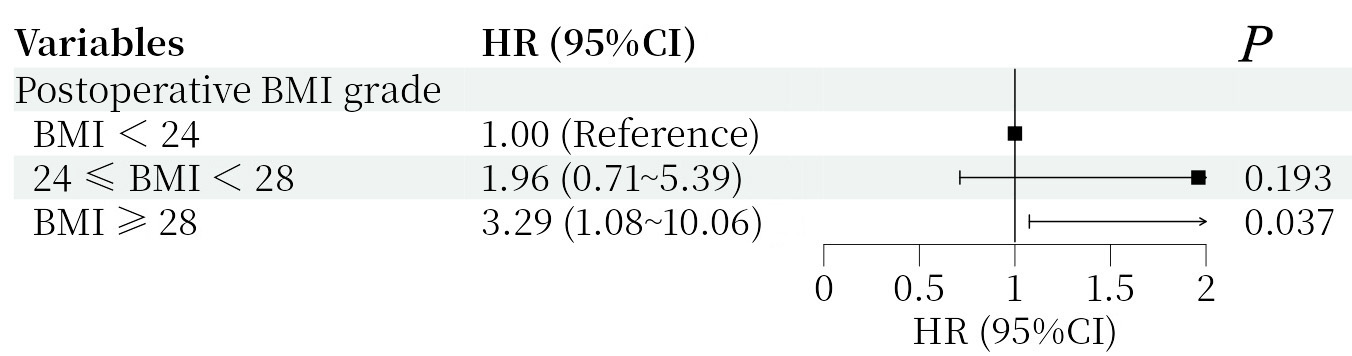
Figure 2. Forest plot of the multivariate Cox analysis for the PAF group. Hazard ratio (HR) with 95% confidence interval (CI) and P values are shown for postoperative BMI grade and AF duration. The reference group was BMI < 24 kg/m2. PAF: Paroxysmal atrial fibrillation; BMI: body mass index; AF: atrial fibrillation.
The recurrence rate in the SAF group was 31.43%. Multivariate Cox analysis showed that postoperative overweight [hazard ratio (HR) = 3.19, 95% confidence interval (CI): 1.10-9.27, P = 0.033], postoperative obesity (HR = 5.20, 95%CI: 1.76-15.40, P = 0.003), and AF duration > 12 months (HR = 3.04, 95%CI: 1.50-6.16, P = 0.002) were independently associated with SAF recurrence [Figure 3]. Kaplan-Meier estimates showed that, among patients with SAF, the 18 months AF recurrence-free rate was 69.1% in postoperative overweight and 55.3% in postoperative obesity, compared with 88.2% in postoperative normal weight (log-rank P = 0.006; Figure 4).
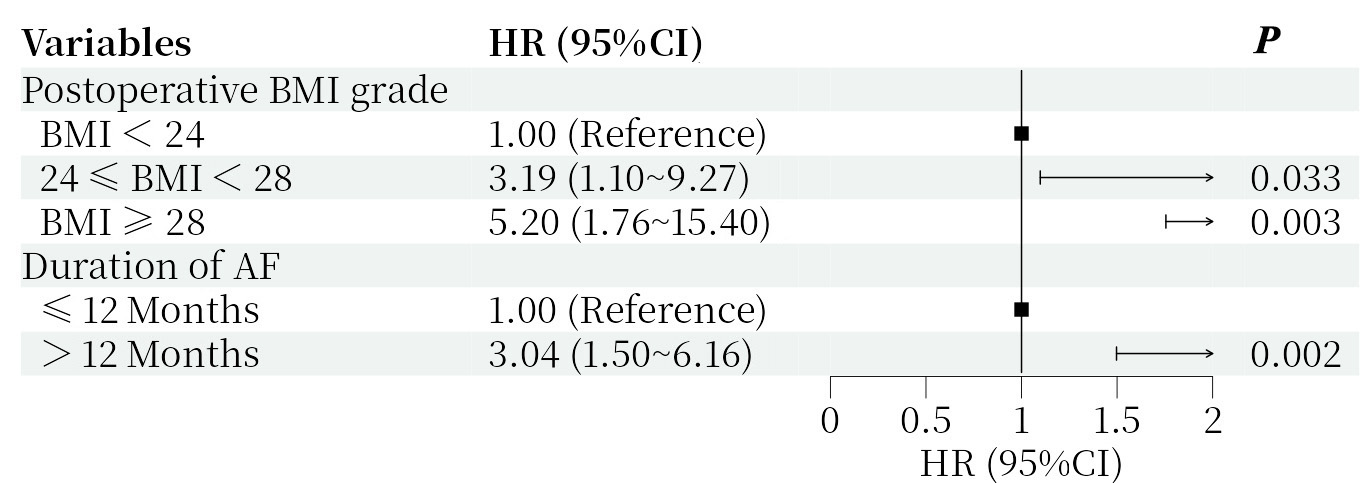
Figure 3. Forest plot of the multivariate Cox analysis for the SAF group. Hazard ratio (HR) with 95% confidence interval (CI) and P values are shown for postoperative BMI grade and AF duration. The reference groups were BMI < 24 kg/m2 and AF duration ≤ 12 months, respectively. SAF: Persistent atrial fibrillation; BMI: body mass index; AF: atrial fibrillation
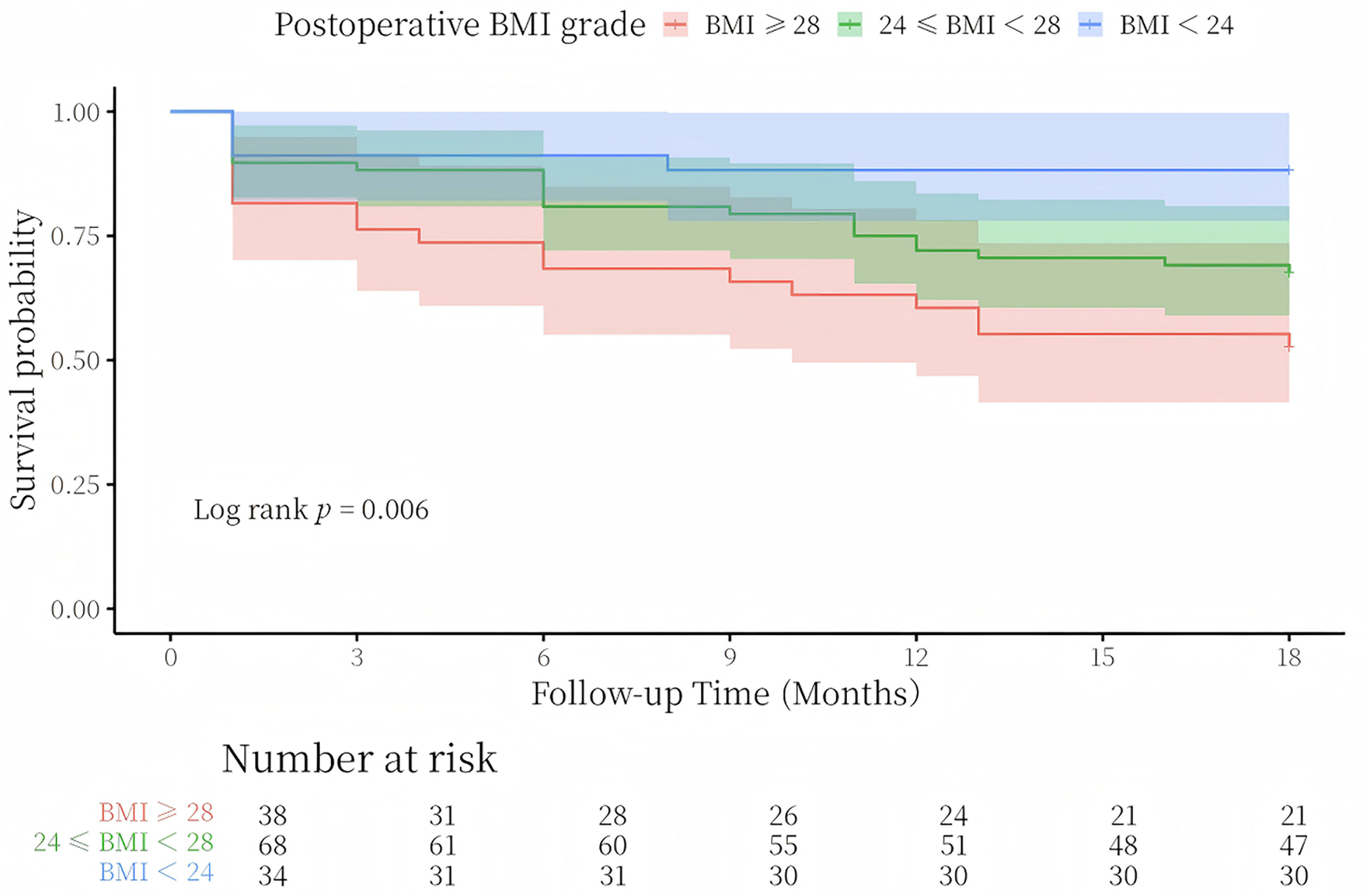
Figure 4. Kaplan-Meier analysis of freedom from AF recurrence in the SAF group. The plot shows recurrence-free survival over follow-up time (months) according to postoperative BMI grade (BMI ≥ 28 kg/m2, 24 ≤ BMI < 28 kg/m2, and BMI < 24 kg/m2). The log-rank test yielded P = 0.006. The number of patients at risk in each BMI category is displayed below the plot. SAF: Persistent atrial fibrillation; BMI: body mass index; AF: atrial fibrillation
No procedure-related complications, including left atrial appendage electrical isolation, pericardial effusion, cardiac tamponade, or left phrenic nerve injury, were observed. No stroke, transient ischemic attack, or death occurred during the 18 months follow-up period in the overall cohort.
DISCUSSION
This single-center retrospective analysis investigated factors independently associated with recurrence after ablation in different AF subtypes. The key findings were as follows: in patients with PAF, postoperative BMI ≥ 28 kg/m2 was associated with a higher recurrence risk; in patients with SAF, postoperative BMI category and longer AF duration (> 12 months) showed stronger independent associations with recurrence. Among patients with SAF, postoperative BMI showed a dose-response association with recurrence risk, and freedom from AF recurrence decreased with increasing postoperative BMI grade.
In this study, postoperative BMI was associated with different recurrence patterns after RCA among patients with PAF and SAF, suggesting pathophysiological heterogeneity between these two AF subtypes. In PAF, the main arrhythmogenic mechanism is typically pulmonary vein ectopy, with relatively mild atrial electrical remodeling and limited atrial substrate alteration. Thus, when postoperative BMI was ≥ 28 kg/m2, obesity-related systemic pathophysiological changes may have been sufficient to exceed the atrial compensatory capacity, thereby increasing the risk of PAF recurrence. This finding may be related to obesity-mediated systemic inflammation and increased sympathetic tone[12,13]. In obesity, epicardial adipose tissue accumulates and releases pro-inflammatory cytokines such as interleukin-1 beta (IL-1β), interleukin-6 (IL-6), and tumor necrosis factor-alpha (TNF-α). These cytokines may enter the circulation and affect the pulmonary vein myocardial sleeves, enhancing electrical excitability and increasing ectopic activity. Meanwhile, sympathetic activation, accelerated heart rate, and increased myocardial oxygen consumption may further reduce atrial electrical stability, ultimately contributing to recurrence in patients with PAF. In patients with PAF and postoperative BMI < 28 kg/m2, obesity-related pathophysiological effects may have been less pronounced and may not have reached a threshold sufficient to disrupt atrial electrophysiological stability; accordingly, this BMI category was not independently associated with recurrence.
In contrast, patients with SAF have a more complex pathophysiological substrate. Their atria may have undergone more advanced electrical and structural remodeling, characterized by more extensive atrial fibrosis, reduced conduction velocity, and greater conduction heterogeneity. These changes may promote the formation of multiple potential reentrant circuits, making the atrial substrate more susceptible to obesity-related effects. At this stage, obesity may exert a more sensitive and profound influence on the atrial substrate. Therefore, both postoperative overweight and postoperative obesity in patients with SAF emerged as factors independently associated with recurrence and were significantly correlated with recurrence-free survival. In patients with SAF and poor postoperative weight control, persistent obesity may maintain and exacerbate the proarrhythmic milieu through multiple mechanisms. First, epicardial adipose tissue may continue to exert paracrine effects by releasing pro-inflammatory cytokines and fibrotic mediators such as adipocytokines and transforming growth factor-beta 1 (TGF-β1), thereby promoting atrial fibrosis and stabilizing the reentrant substrate[14]. Second, obesity-related electrophysiological changes, including increased voltage heterogeneity and more fractionated potentials, may reduce cardiomyocyte electrical stability and provide a substrate for arrhythmogenesis[15]. Finally, increased circulating blood volume and cardiac load in obesity may contribute to passive atrial dilation and further atrial remodeling[16], potentially creating a self-reinforcing cycle of obesity-associated atrial remodeling and AF recurrence. Although RCA can isolate pulmonary vein triggers and modify the local atrial substrate, it may not fully reverse the systemic and epicardial proarrhythmic milieu associated with obesity, which may explain why postoperative BMI status was independently associated with recurrence.
Furthermore, AF duration exceeding 12 months was independently associated with SAF recurrence. This finding is consistent with the report by Calvert et al.[17] and supports the concept that atrial fibrosis may progress with longer AF duration. In patients with SAF and AF duration exceeding 12 months, atrial remodeling may have advanced substantially. Although RCA eliminated dominant triggers, the established fibrotic substrate may still facilitate the formation of new reentrant circuits. These findings suggest that, for patients with SAF, clinicians should emphasize not only postoperative weight management but also timely intervention.
Several earlier studies did not identify a significant association between BMI and AF recurrence[7,8]. However, many investigations have confirmed that obesity is associated with both AF onset and recurrence after ablation[9,10,18,19]. This study extends previous work in two main respects. First, it identified postoperative BMI, rather than baseline BMI alone, as a factor associated with SAF recurrence, providing direct evidence for dynamic postoperative management. Second, stratified analysis quantified the risk gradient across BMI categories, with recurrence-free survival decreasing from 88.2% in postoperative normal weight to 55.3% in postoperative obesity. This gradient may facilitate more precise risk communication.
The mechanisms outlined above highlight the important role of postoperative BMI management in the comprehensive treatment framework for AF ablation. RCA primarily eliminates localized pulmonary vein triggers and modifies the atrial electrophysiological substrate, whereas persistent obesity is associated with a sustained systemic proarrhythmic milieu. If this systemic proarrhythmic environment is not addressed after the procedure, it may continue to contribute to atrial structural and electrical remodeling and potentially reduce the therapeutic benefit of RCA. Therefore, postoperative BMI may function not only as a risk indicator but also as a modifiable therapeutic target. Systematic postoperative weight management should be considered an important component of ablation therapy because it targets systemic proarrhythmic factors that ablation alone cannot eliminate. This approach may be an important strategy for long-term AF management.
Strengths and limitations
The main strengths of this study are as follows. First, all procedures were performed by the same experienced operator, minimizing the potential impact of procedural variability and enhancing the reliability of the findings. Second, strict exclusion criteria, such as patients with missing baseline data, incomplete postoperative follow-up data, or severe valvular heart disease, improved the homogeneity of the study cohort.
This study has several limitations. First, because this was a single-center retrospective study with a relatively limited sample size (n = 250), selection bias may have been introduced, and generalizability may be limited. No a priori sample size calculation was performed, which may have affected the statistical power of subgroup analyses. The retrospective design also precludes causal inference. Second, postoperative BMI was assessed only at the 18 months follow-up; repeated BMI measurements during follow-up were not available. Therefore, potential weight fluctuations or trajectories could not be captured. Third, the limited sample size may have reduced the statistical power of subgroup analyses; for example, it was not possible to further analyze the association between postoperative BMI and AF recurrence in subgroups defined by AF duration, age, or comorbidities. Fourth, this study relied mainly on BMI to assess postoperative obesity. BMI reflects the ratio of weight to height but does not distinguish body fat distribution, whereas measures of abdominal obesity may better reflect visceral adiposity. Finally, although the multivariate Cox model adjusted for several clinically relevant confounders, residual confounding from unmeasured factors may remain, including changes in antihypertensive or antidiabetic medications after the blanking period and adherence to weight management.
Future studies should address these limitations by conducting multicenter prospective cohort studies with larger sample sizes and patients from different regions and hospitals to further evaluate the generalizability of these findings. Randomized controlled trials are also needed to compare conventional management plus intensive weight intervention with conventional management alone for reducing recurrence after AF RCA, with dynamic recording of weight changes to directly assess the clinical efficacy of weight intervention. Future studies should also incorporate more refined measures of obesity, such as waist circumference and body fat percentage, together with inflammatory and metabolic biomarkers, to establish multidimensional recurrence prediction models that integrate clinical and biomarker data. Finally, follow-up should be extended to 3-5 years to dynamically assess postoperative BMI and evaluate the impact of postoperative BMI changes on long-term recurrence and adverse cardiovascular events, thereby providing more comprehensive evidence for long-term management strategies.
Conclusion
In this retrospective analysis, postoperative obesity assessed at a single time point (18 months) was associated with a higher risk of recurrence after RCA for AF. Specifically, among patients with PAF, a BMI ≥ 28 kg/m2 at 18 months was associated with an increased recurrence risk. Among patients with SAF, higher postoperative BMI grades at 18 months and AF duration exceeding 12 months were also associated with recurrence.
DECLARATIONS
Authors’ contributions
Made substantial contributions to the conception and design of the study and performed data analysis and interpretation: Yang W, Zhang D, Li Y
Performed data acquisition: Yang W, Yan Y
Critical revision and supervision: Zhang Q, Zhang P, Zhang Y, Zhang J
Provided administrative, technical, and material support: Han Y, Wang Z, Liang M
Availability of data and materials
The datasets generated and analyzed during this retrospective study are not publicly available due to privacy protection requirements stipulated by the institutional ethical approval and the waiver of written informed consent for participants, aiming to strictly safeguard patient privacy and confidential medical information. Anonymized data that support the findings of this study may be made available from the corresponding author, Liang M, or from the Ethics Committee of the General Hospital of Northern Theater Command upon reasonable request. Any data sharing will be subject to a formal data use agreement in compliance with institutional regulations and applicable laws.
AI and AI-assisted tools statement
During the preparation of this manuscript, the AI tool ChatGPT (version 5.0, released 2025-08-07) was used solely for English language editing. The tool did not influence the study design, data collection, analysis, interpretation, or the scientific content of the work. All authors take full responsibility for the accuracy, integrity, and final content of the manuscript.
Financial support and sponsorship
This work was supported by the State Key Laboratory of Frigid Zone Cardiovascular Disease, Cardiovascular Research Institute and Department of Cardiology, General Hospital of Northern Theater Command, the Noncommunicable Chronic Diseases-National Science and Technology Major Project (2023ZD0504200), and the Liaoning Provincial Science and Technology Plan Project (2025JH2/101800025). The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
This study was conducted in accordance with the principles of the Declaration of Helsinki. The study protocol was reviewed and approved by the Ethics Committee of the General Hospital of Northern Theater Command [Approval No. Y (2025) 529]. The requirement for informed consent was waived by the institutional review board given the retrospective design and complete anonymization of all patient data.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Ataey A, Jafarvand E, Adham D, Moradi-Asl E. The relationship between obesity, overweight, and the human development index in world health organization eastern mediterranean region countries. J Prev Med Public Health. 2020;53:98-105.
2. Tabaja C, Younis A, Santageli P, et al. Impact of obesity on catheter ablation of atrial fibrillation: patient characteristics, procedural complications, outcomes, and quality of life. J Cardiovasc Electrophysiol. 2023;34:1648-57.
3. Lavie CJ, Pandey A, Lau DH, Alpert MA, Sanders P. Obesity and atrial fibrillation prevalence, pathogenesis, and prognosis: effects of weight loss and exercise. J Am Coll Cardiol. 2017;70:2022-35.
4. Huxley RR, Lopez FL, Folsom AR, et al. Absolute and attributable risks of atrial fibrillation in relation to optimal and borderline risk factors: the atherosclerosis risk in communities (ARIC) study. Circulation. 2011;123:1501-8.
5. Turagam MK, Musikantow D, Whang W, et al. Assessment of catheter ablation or antiarrhythmic drugs for first-line therapy of atrial fibrillation: a meta-analysis of randomized clinical trials. JAMA Cardiol. 2021;6:697-705.
6. Prasitlumkum N, Chokesuwattanaskul R, Kaewput W, et al. Utilization and in-hospital complications of catheter ablation for atrial fibrillation in patients with obesity and morbid obesity. Clin Cardiol. 2022;45:407-16.
7. Letsas KP, Siklódy CH, Korantzopoulos P, et al. The impact of body mass index on the efficacy and safety of catheter ablation of atrial fibrillation. Int J Cardiol. 2013;164:94-8.
8. Badheka AO, Rathod A, Kizilbash MA, et al. Influence of obesity on outcomes in atrial fibrillation: yet another obesity paradox. Am J Med. 2010;123:646-51.
9. Urbanek L, Bordignon S, Chen S, et al. Impact of body mass index on cryoablation of atrial fibrillation: Patient characteristics, procedural data, and long-term outcomes. J Cardiovasc Electrophysiol. 2022;33:1106-15.
10. Donnellan E, Wazni OM, Kanj M, et al. Impact of risk-factor modification on arrhythmia recurrence among morbidly obese patients undergoing atrial fibrillation ablation. J Cardiovasc Electrophysiol. 2020;31:1979-86.
11. Joglar JA, Chung MK, Armbruster AL, et al. ; Peer Review Committee Members. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2024;149:e1-e156.
12. Meulendijks ER, Krul SPJ, Baalman SW, et al. Circulating adipose tissue proteins involved in atrial fibrillation: an explorative scoping review. Trends Cardiovasc Med. 2024;34:148-58.
13. McCauley MD, Hong L, Sridhar A, et al. Ion channel and structural remodeling in obesity-mediated atrial fibrillation. Circ Arrhythm Electrophysiol. 2020;13:e008296.
14. Mahajan R, Lau DH, Brooks AG, et al. Atrial fibrillation and obesity: reverse remodeling of atrial substrate with weight reduction. JACC Clin Electrophysiol. 2021;7:630-41.
15. Sha R, Baines O, Hayes A, et al. Impact of obesity on atrial fibrillation pathogenesis and treatment options. J Am Heart Assoc. 2024;13:e032277.
16. Mangiafico V, Saberwal B, Lavalle C, et al. Impact of obesity on atrial fibrillation ablation. Arch Cardiovasc Dis. 2020;113:551-63.
17. Calvert P, Mills MT, Gupta D. Duration of atrial fibrillation: how much is too much? Heart Rhythm 2024;21:741-2.
18. Peigh G, Wasserlauf J, Vogel K, et al. Impact of pre-ablation weight loss on the success of catheter ablation for atrial fibrillation. J Cardiovasc Electrophysiol. 2021;32:2097-104.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Special Topic
Copyright

Data & Comments
Data
0











Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].