


fig2
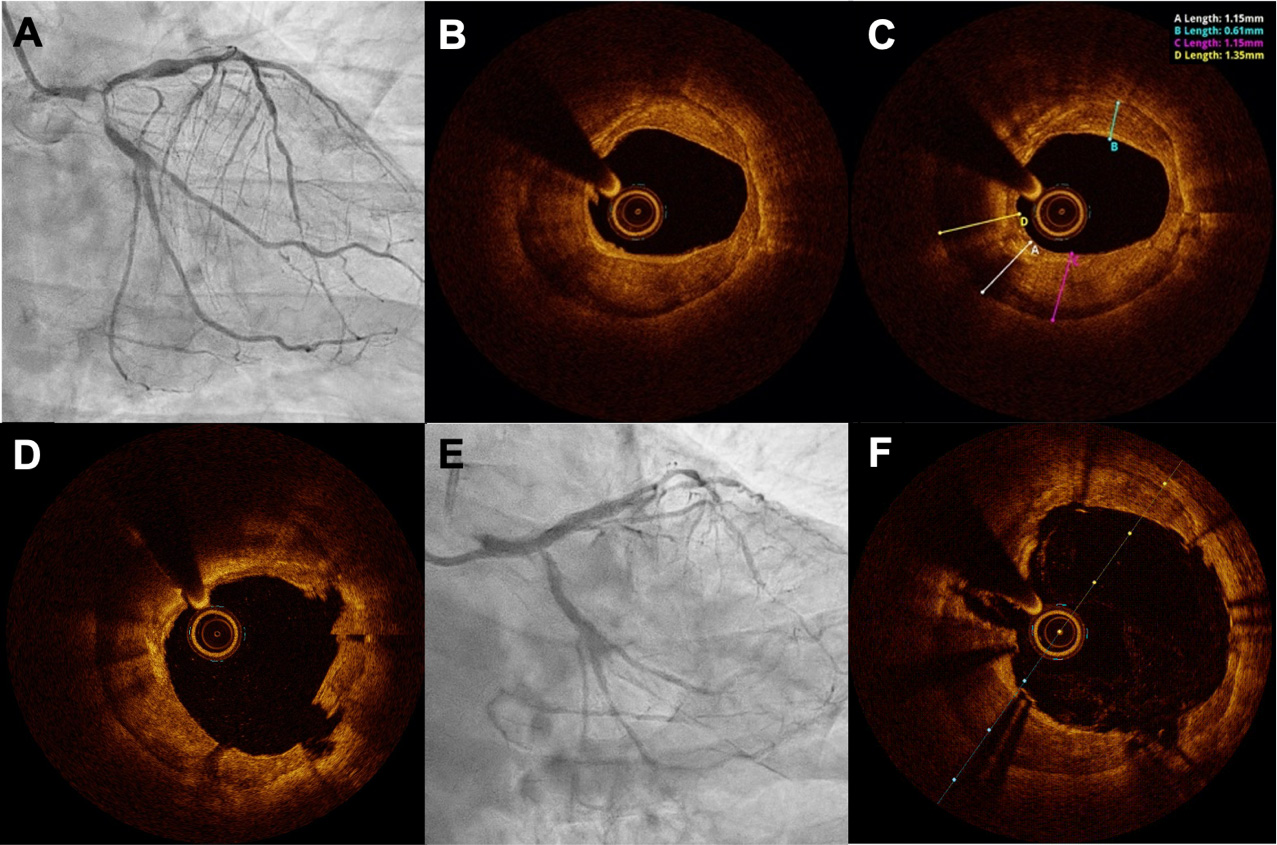
Figure 2. A 74-year-old male patient with severe calcific three-vessel disease presented with critical stenosis at the left main bifurcation (Medina 1,1,1), proximal LAD, OM2, and CTO of the mid RCA (A), who refused cardiac surgery. As the first step,



