


Generative artificial intelligence in plastic surgery: emerging applications in preoperative psychological screening and patient empowerment
 0
0 Abstract
Preoperative psychological screening in plastic surgery faces inconsistent implementation due to time constraints and patients’ reluctance to disclose distress. This narrative review explores the emerging roles of generative artificial intelligence (AI), particularly large language models (LLMs), in supporting preoperative psychological assessment and patient empowerment. This review synthesizes literature across four key domains: (1) psychological risk constructs; (2) conversational screening and language-based signal detection; (3) patient-facing psychoeducation and expectation management; and (4) system design, governance, and limitations. Current evidence suggests that LLM-enabled conversational agents can facilitate structured history-taking, elicit expectation-related cues, and deliver tailored psychoeducation in a low-stigma format. Hybrid approaches, combining validated psychometric instruments with free-text dialogue, may further improve contextualization for clinician review. Despite these potential benefits, key risks persist. These include hallucinations, demographic and aesthetic bias, privacy concerns, and a lack of standardized clinical validation. While generative AI can augment preoperative care by expanding access to screening-like interactions and expectation calibration, its deployment must be strictly bounded by a clearly defined scope, human oversight, and safety-by-design governance.To enable safer risk stratification and real-world implementation, future research should prioritize prospective clinical validation, robust escalation protocols, and multimodal approaches.
Keywords
INTRODUCTION
An important but inconsistently implemented component of aesthetic and reconstructive plastic surgery, preoperative psychological screening helps clinicians identify patients at elevated risk for postoperative dissatisfaction, emotional maladjustment, or decisional regret[1]. Psychological factors - including body image distortion, perfectionistic aesthetic ideals, subclinical body dysmorphic traits, and unrealistic expectations have been linked to lower satisfaction, reduced adherence during recovery, and increased postoperative conflicts[1]. In routine practice, however, structured psychological interviews and standardized psychometric scales are not consistently employed. Challenges include limited consultation time, restricted access to trained mental health professionals, and patients’ reluctance to disclose distress during brief, symptom-focused encounter[1]. At the same time, artificial intelligence (AI) is increasingly integrated into plastic and reconstructive surgery, aiding in tasks such as risk prediction, preoperative planning, and outcome assessment[2].
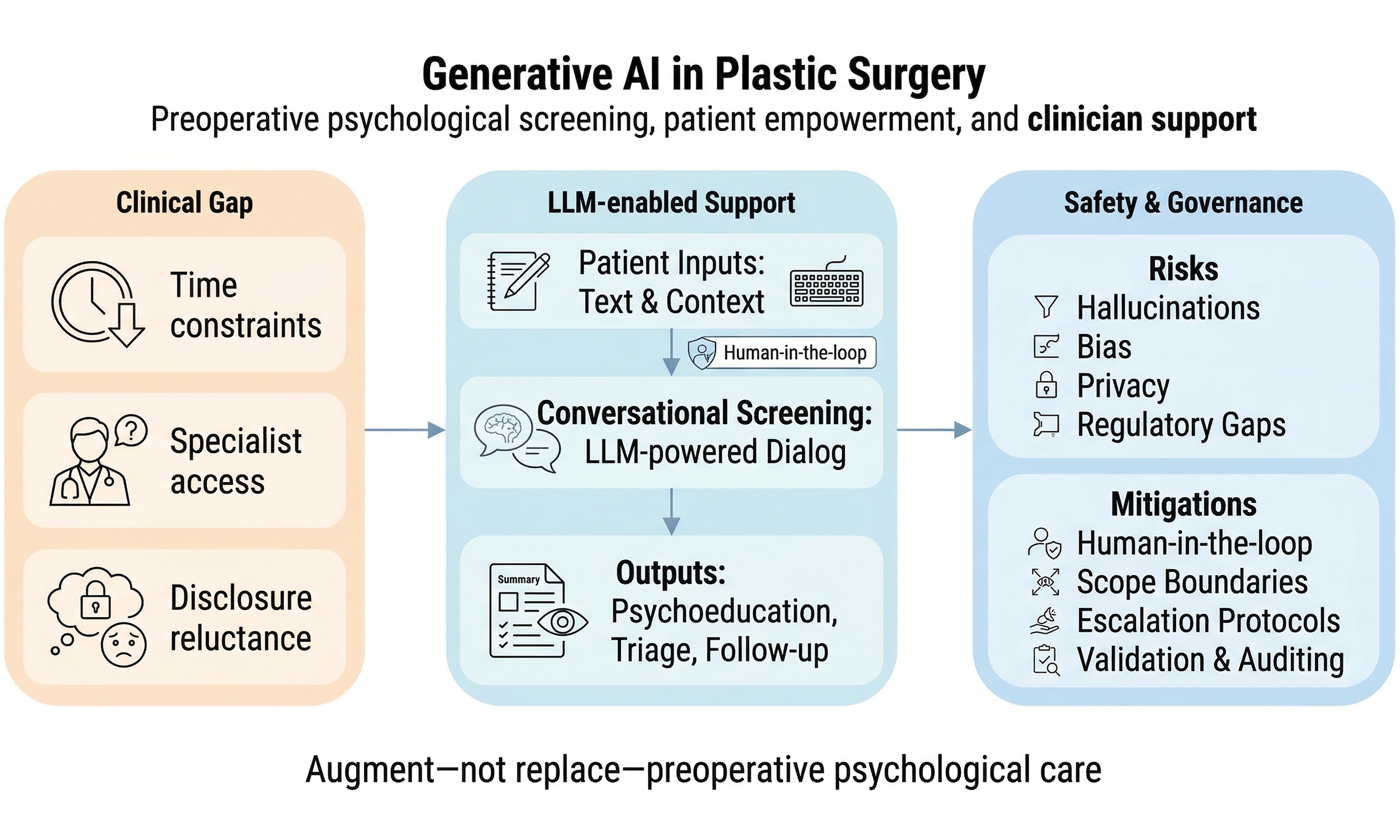
These workflow constraints necessitate scalable, individualized, and low-barrier tools to foster psychological readiness and align expectations before surgery. Generative AI - particularly LLM-enabled conversational systems - has exhibited good potential to sustain naturalistic, context-aware dialogue and may help elicit motivation-, expectation-, and affect-related cues from patient narratives. In the preoperative plastic surgery setting, these systems facilitate a structured workflow that integrates patient-reported concerns and questionnaire responses, free-text narratives, screening-like dialogue, patient-facing psychoeducation, clinician-facing summarization, and safety governance [Figure 1] - has demonstrated the ability to sustain naturalistic, context-aware dialogue, and may help elicit motivation-, expectation-, and affect-related cues from patient narratives[3]. Compared to static questionnaires, LLM-powered conversational interfaces can adapt follow-up questions in real time, effectively mimicking semi-structured interviews. This dynamic capability suggests a potential role for generative AI in augmenting preoperative counseling and supporting the early identification of patients who could benefit from more in-depth clinician review or specialized referral pathways[4]. Importantly, AI deployment in plastic surgery is no longer purely conceptual; instead, AI methods are actively being explored across subspecialties like breast reconstruction for applications such as preoperative planning, complication prediction, aesthetic outcome assessment, and patient education, thereby underscoring its broader trajectory toward patient-centered care[5].
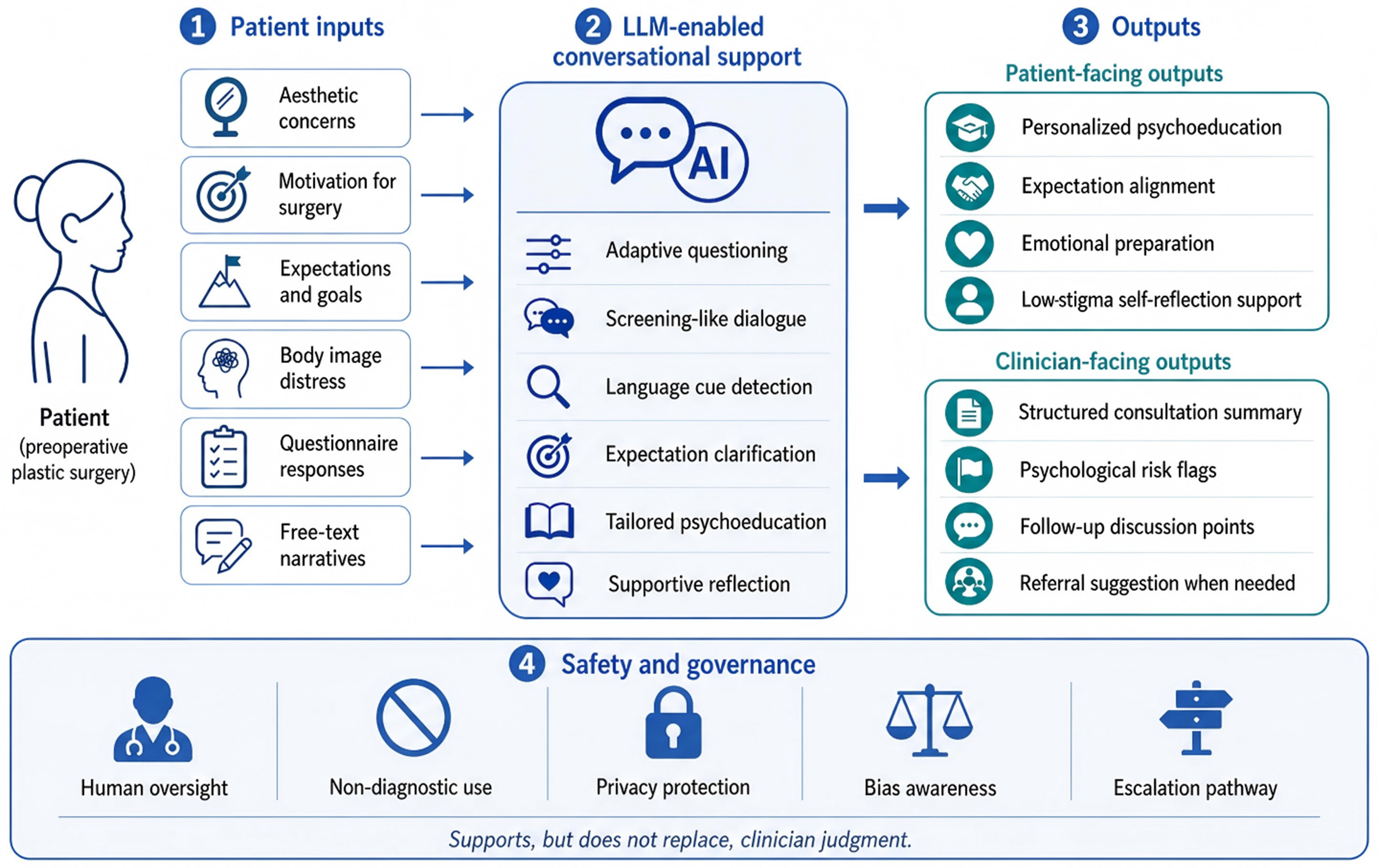
Figure 1. A conceptual overview of generative AI for preoperative psychological screening and patient empowerment in plastic surgery. AI: Artificial intelligence; LLM: large language model.
This schematic illustrates how an LLM-enabled conversational interface processes patient-reported information, including aesthetic concerns, motivations, expectations, questionnaire responses, and free-text narratives. The system supports screening-like intake, psychoeducation, expectation clarification, and clinician-facing summarization. It is designed to augment, rather than replace, clinician judgment, and operates within a governed framework that includes human oversight, non-diagnostic use, privacy protection, bias awareness, and escalation pathways.
Initial studies are evaluating LLM performance in patient-facing communication. In simulated consultations (e.g., rhinoplasty, abdominoplasty), LLM-generated responses have been rated as coherent and readable, potentially incorporating elements of motivational interviewing (MI)-style reflection and cognitive-behavioral psychoeducation[4,6]. However, the evidence base is nascent, with current evaluations often limited to vignette-based studies or focused on feasibility. Major challenges include the reliability of LLMs in recognizing nuanced psychological risks, the limited interpretability of their outputs, and safety concerns such as hallucinated content or demographic and cultural bias. Furthermore, few publications describe comprehensive, end-to-end architectures that integrate conversational screening, structured reporting for surgeons, and patient-facing educational or supportive modules within clinically governed workflows[7].
This narrative review synthesizes emerging concepts and early evidence on the application of generative AI for preoperative psychological screening and patient empowerment in plastic surgery. We first outline the psychological risks pertinent to aesthetic surgery candidates and summarize unmet needs in current practice[3]. We then examine generative AI’s potential to support conversational screening, expectation management, and scalable psychoeducation, while underscoring the critical need for human oversight and clear boundaries of use. Finally, we discuss its limitations and future directions - including multimodal sensing, federated learning, and ethical governance - to propose a pragmatic roadmap for safe and clinically meaningful translation.
To obtain the relevant literature for this narrative review, an extensive retrieval process was conducted in PubMed, Scopus, and Google Scholar, covering the period from January 2015 to March 2025. Search keywords included: generative AI, large language models (LLMs), ChatGPT, plastic surgery, aesthetic surgery, preoperative psychological screening, patient empowerment, and natural language processing (NLP). We prioritized peer-reviewed primary literature, including systematic reviews and clinical feasibility studies, that examined the application of AI technology in surgical decision-making, psychological risk evaluation, and patient education. Articles were screened for relevance to plastic and reconstructive surgery clinical situations, with a particular focus on novel conversational AI tools and their ethical or practical implications.
PSYCHOLOGICAL RISK LANDSCAPE IN PLASTIC SURGERY CANDIDATES
The psychological profile of aesthetic plastic surgery candidates is often more complex than their stated motivations imply. Although these procedures are elective and highly personal, requests for cosmetic change may stem less from objective deformity or functional impairment and more from perceived shortcomings in self-image, social standing, or emotional well-being[8]. With beauty ideals increasingly influenced by digitally curated content and algorithmic aesthetics, a patient’s preoperative psychological readiness and their ability to maintain stable expectations have become crucial for postoperative satisfaction and psychosocial resilience.
Body image-related psychopathology, particularly body dysmorphic disorder (BDD) and subclinical dysmorphic traits, is a significant concern within this population. Patients exhibiting dysmorphic preoccupation, cognitive rigidity, or externally contingent self-worth often report dissatisfaction even with objectively acceptable surgical outcomes. Clinically, this manifests as persistent fixation on minor imperfections, repeated reassurance-seeking, emotional volatility, and, at times, escalated conflict with providers. Consequently, studies have explored structured or technology-assisted screening approaches to facilitate earlier identification and referral of these higher-risk individuals. However, the strength and generalizability of the available evidence vary across different settings and instruments[9].
A complementary line of work examines language use as a proxy for psychological distress. NLP models, applied to patient-generated text - such as open-ended intake responses, clinical narratives, or interview transcripts - have shown promise in identifying linguistic markers associated with anxiety, depressive symptoms, rumination, and crisis-related content[10]. In preoperative plastic surgery, language signals should not be interpreted as standalone diagnostic outputs. Instead, their assessment requires privacy-preserving preprocessing, contextual review, and clinician-supervised thresholds [Figure 2]. However, applying such approaches to plastic surgery demands careful contextual consideration. This is because appearance-related narratives can be emotionally charged without necessarily reflecting a clinical disorder, and signals derived from social media or non-clinical text may not directly map onto surgical decision-making risk. These challenges underscore the need for domain-specific constructs and clinically governed thresholds when implementing language-based screening in aesthetic practice.
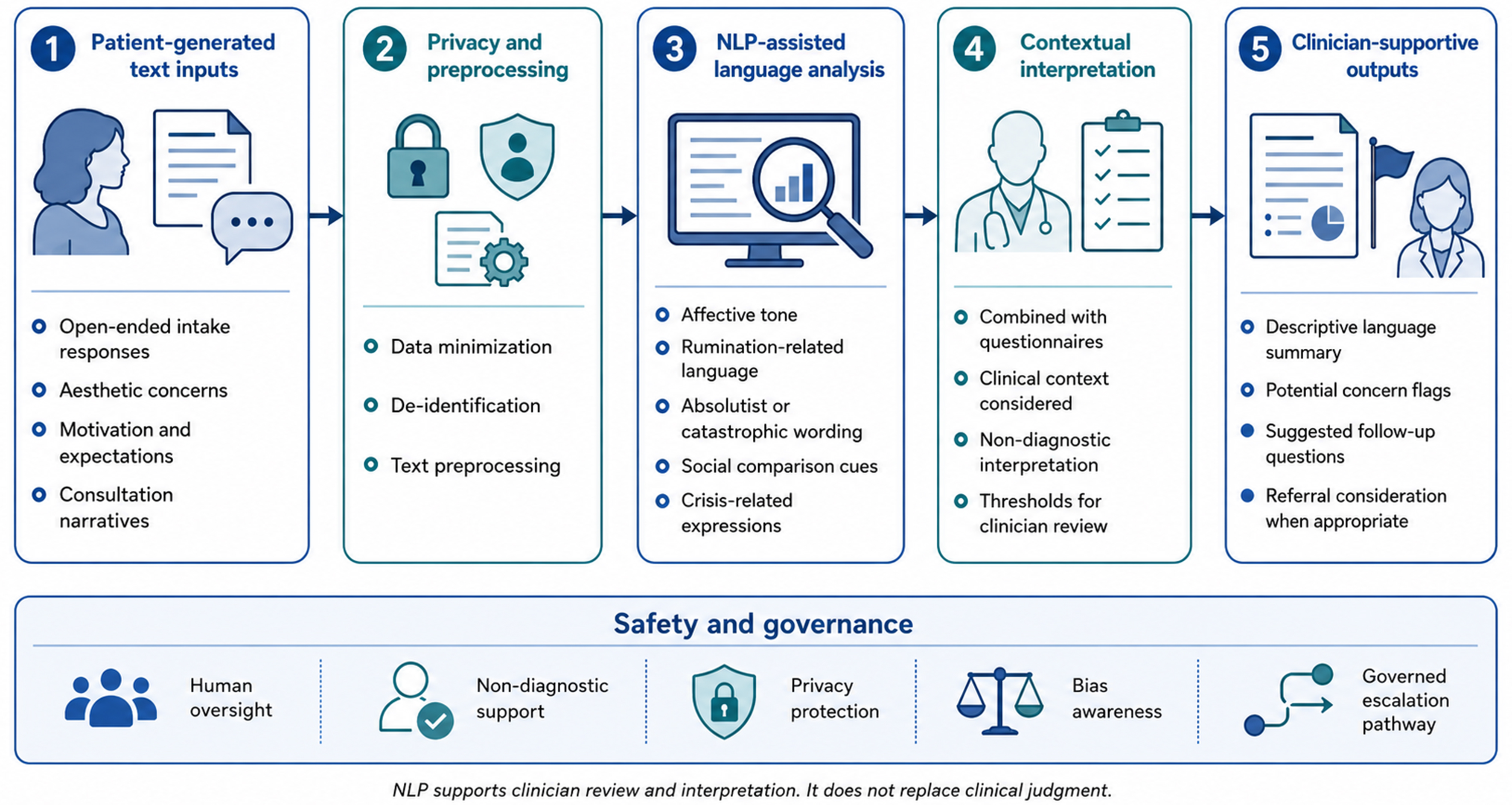
Figure 2. NLP-assisted workflow for preoperative psychological risk review in plastic surgery. NLP: Natural language processing.
This schematic illustrates how patient-generated text - including open-ended intake responses, aesthetic concerns, motivation-related statements, and consultation narratives - is processed using privacy-preserving preprocessing and NLP-assisted language analysis. The potential linguistic signals identified, such as affective tone, rumination-related language, catastrophic wording, social comparison cues, and crisis-related language cues, should be interpreted within a clinical context. These signals are meant to support descriptive summaries, follow-up questions, and clinician review, not automated diagnosis or definitive risk classification.
Despite broad agreement on the importance of psychological readiness, routine clinical workflows often lack systematic tools to capture relevant risk profiles. While common screening instruments like the Symptom Checklist-90 (SCL-90) or the Beck Depression Inventory (BDI) offer general measures of psychopathology, they often overlook constructs specific to surgery, such as aesthetic perfectionism, appearance-based social comparison, media-driven body dissatisfaction, and unstable or externally imposed expectations[1,11]. Moreover, plastic surgery consultations are typically brief, high-volume, and primarily focused on anatomical planning, which inherently limits the feasibility of in-depth psychological interviewing. Surgeons often lack the time and formal training for structured assessments, while patients may underreport distress due to stigma, minimization, or fear of being denied surgery.
Even when psychological risk is suspected, scalable and accessible support options are often limited. Consequently, many patients experiencing appearance-related anxiety or strong social pressures do not receive targeted, evidence-informed guidance prior to surgery. This leaves emotional vulnerabilities unaddressed and increases the likelihood of postoperative regret or maladjustment[12]. While educational innovations, such as AI-assisted simulation and individualized training in graduate medical education, can help bridge some clinician communication gaps, they do not fully address patients’ need for continuous, accessible preparation and expectation management[13].
These challenges underscore a two-fold unmet need: (1) practical mechanisms for early, structured identification of psychological risk signals in routine preoperative workflows; and (2) scalable support promoting readiness and realistic expectations without replacing clinical judgment. This justifies exploring generative AI as a patient-facing interface to facilitate structured dialogue, support psychoeducation, and triage higher-risk presentations for clinician review within a governed care pathway.
GENERATIVE AI AS A TOOL FOR PREOPERATIVE PSYCHOLOGICAL SCREENING
Psychological vulnerabilities in aesthetic surgery candidates are often subtle, context-dependent, and underreported. Consequently, traditional approaches - brief clinician-led interviews and fixed questionnaires - frequently overlook relevant cognitive-emotional patterns, including perfectionistic appearance ideals, externally driven motivation, and self-evaluation shaped by social media. Such assessment gaps have spurred interest in generative AI, particularly LLMs like ChatGPT, as a conversational interface capable of supporting structured preoperative assessment through adaptive questioning and patient-friendly psychoeducation. In contrast to static instruments, LLM-enabled dialogue offers a flexible way to explore motivations, expectations, and emotional cues. This approach can potentially reduce barriers to disclosure and help identify cases warranting clinician review, rather than functioning as a standalone diagnostic system. Evidence from adjacent surgical contexts further suggests that AI-enabled decision aids can improve shared decision-making and decision quality by providing individualized risk-benefit information and outcome estimates[14]. Leveraging these capabilities, generative AI applications in preoperative plastic surgery care encompass several clinically relevant domains: psychological screening, decision support, psychoeducation and consent support, expectation management, and self-guided supportive functions [Figure 3].
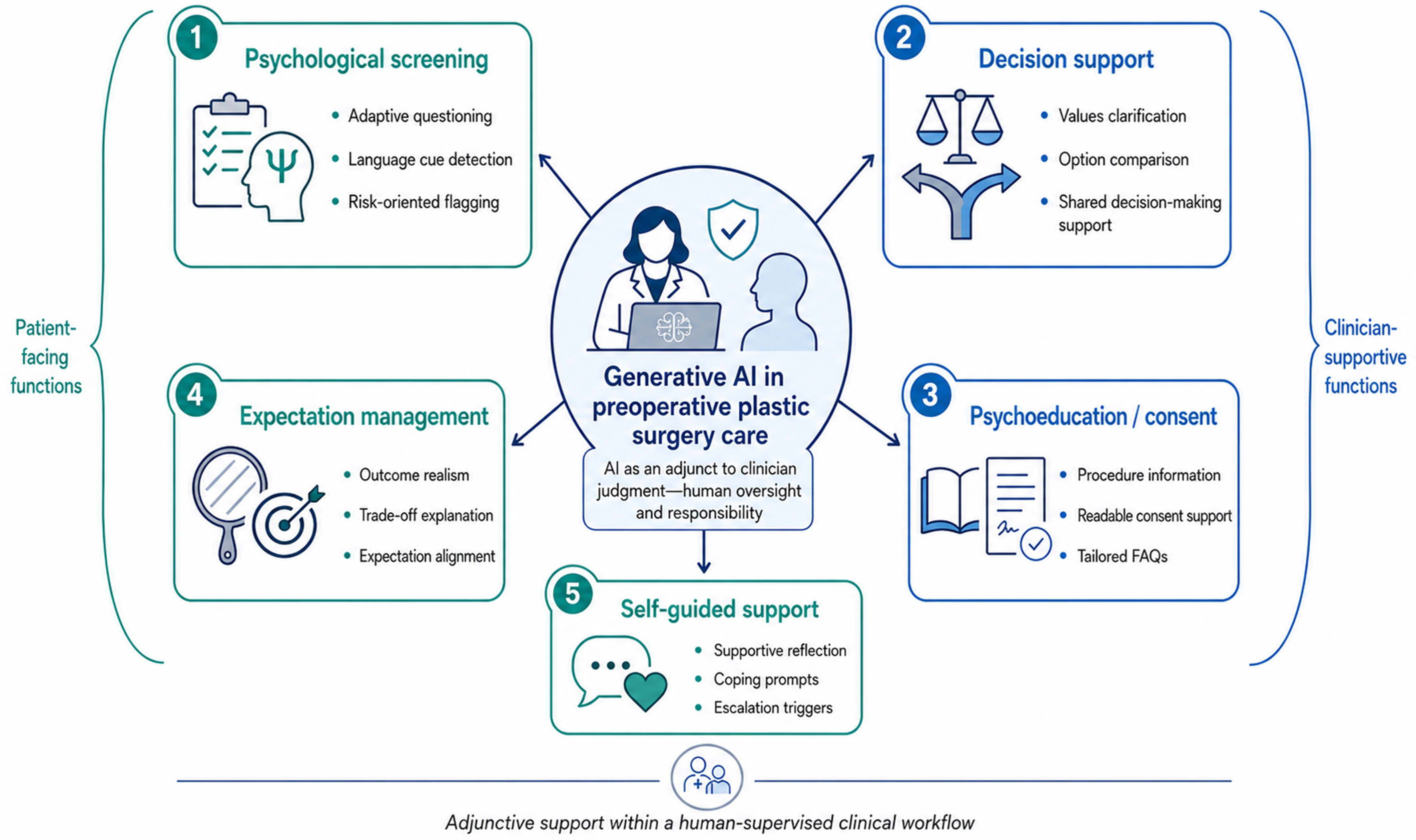
Figure 3. Major application domains of generative AI in preoperative plastic surgery care. AI: Artificial intelligence; FAQs: frequently asked questions.
This schematic summarizes the major application domains of generative AI in preoperative plastic surgery care: psychological screening, decision support, psychoeducation and consent support, expectation management, and self-guided supportive functions. These applications are designed to be adjunctive and human-supervised , facilitating patient empowerment and supporting clinicians in assessment, rather than serving as autonomous diagnostic or decision-making tools.
LANGUAGE-BASED PSYCHOLOGICAL ASSESSMENT POTENTIAL
Trained on vast corpora of human communication, LLMs can discern affective tone, semantic emphasis, and discourse patterns within patient narratives. Unlike fixed-response psychometric instruments, LLM-enabled interfaces can interpret unstructured free-text input and generate context-aware follow-up questions, thereby approximating elements of semi-structured interviewing. In preoperative aesthetic consultations, this capability could help identify risk-relevant cues regarding patient expectations, motivation, and distress.
For example, language that is absolutist (e.g., “I can’t live with this nose”), ruminative (e.g., “I think about it all day”), or comparison-focused (e.g., “everyone else looks better”) may signal heightened preoccupation or fragile self-evaluation and can be used to prompt clarification rather than to establish a diagnosis[15].
NLP research, from a broader perspective, suggests that unstructured patient-generated text can contain linguistic markers of psychological distress, while aesthetic surgery literature emphasizes assessing body image concerns and symptoms of BDD using validated screening tools[9,10]. Within this context, open-ended aesthetic narratives can offer valuable insights into motivation, expectations, and distress; however, such linguistic cues should serve as prompts for clinician review, not as standalone diagnostic evidence. These observations support the feasibility of integrating language-based screening workflows as an adjunct to traditional assessment Conversational systems could thereby (i) elicit more comprehensive contextual detail than brief checklists; (ii) identify patterns necessitating clinician review; and (iii) document expectation-related themes directly pertinent to surgical counseling. Nevertheless, given that emotionally intense appearance narratives can manifest in the absence of a clinical disorder, linguistic cues must be interpreted within a structured framework - ideally combined with validated instruments and clear escalation thresholds - rather than being utilized for standalone risk stratification.
SIMULATED MI-INFORMED DIALOGUE AND TRIAGE-ORIENTED SUMMARIZATION
Generative AI can also support preoperative counseling by incorporating elements of MI. MI is a validated communication approach designed to elicit patients’ values, strengthen autonomy, and resolve ambivalence in health-related decisions. Through techniques like reflective listening, affect labeling, and values clarification, AI-powered systems can prompt patients to express their motivations and expectations in greater detail. These systems can also gently challenge beliefs that are rigid or externally driven. For example, if a patient expresses a desire to “look like someone on Instagram”, an MI-informed prompt - such as “How do you think achieving that look would affect your day-to-day life?” - can encourage deeper elaboration. This process helps determine if their goals are stable, internally endorsed, and realistically linked to their well-being[16]. Importantly, in this setting, such dialogue should be framed as supportive communication and expectation clarification, distinct from psychotherapy.
This capability is especially pertinent in plastic surgery, where motivations can fluctuate between intrinsic drivers (e.g., self-confidence, identity congruence) and extrinsic pressures (e.g., peer approval, relationship dynamics, social media norms)[17]. Structured conversational prompts can help surgeons identify and document patient expectations during consultations. These prompts surface actionable themes - such as perceived social contingencies, appearance-based self-worth, or idealized outcome comparisons - which then support clinician review and enable targeted counseling. Furthermore, adjacent evidence indicates that LLM-based tools can improve patient-facing materials, including informed consent documents and educational content. Similarly, perioperative chatbots in other surgical specialties have shown high patient satisfaction and improved knowledge acquisition[17-19]. Together, these findings support the integration of MI-informed conversational modules into a structured, hybrid preoperative workflow that prioritizes education, expectation alignment, and clear escalation pathways for emerging concerns.
INTEGRATION WITH STANDARDIZED METRICS AND HYBRID APPROACHES
Importantly, LLM-enabled screening support does not need to function in isolation. A hybrid framework - combining validated psychometric screening instruments and patient-reported outcome measures with open-ended dialogue - can increase contextual depth while maintaining measurement structure. When scale results are ambiguous or borderline, the system can generate targeted follow-up questions to clarify motivation, expectations, and functional impairment. This supports clinician review, rather than enabling automated diagnosis[9]. For example, a patient might score low on a general anxiety measure but reveal persistent rumination or perfectionistic language in free-text responses. This discrepancy signals the need for an in-person discussion.
To operationalize these capabilities for perioperative use, we categorized current and emerging use-cases into distinct application domains, specifying patient-facing outputs, clinician-facing deliverables, and recommended evaluation metrics [Table 1].
Application domains of generative AI in preoperative plastic surgery care: screening, decision support, psychoeducation, expectation management, and self-guided support
| Domain | Specific use-case | Example tasks | Output to patient | Output to clinician | Suggested evaluation metrics |
| Psychological screening | e.g., BDD traits, unrealistic expectations | Adaptive questioning, language marker detection | Risk feedback, prompts for reflection | Risk summary, flags, recommended follow-up questions[9,10] | Sensitivity/specificity, agreement (kappa), AUC |
| Decision support | Shared decision-making | Option comparison, values clarification | Decisional conflict reduction | Patient preference summary[14] | Decisional Conflict Scale, knowledge scores |
| Psychoeducation/consent | Readability and completeness | Informed consent drafting, FAQs | Tailored education | Standardized consent artifact[17] | Readability (Flesch), completeness checklist |
| Expectation management | Outcome realism | Simulation explanation, trade-offs | Expectation calibration | Misalignment alerts | Satisfaction, expectation alignment scale |
| Self-guided support | CBT/MI-informed modules | Reframing, coping scripts | Micro-interventions | Escalation triggers[10,18] | Symptom scale change, adherence |
Moreover, text from AI-guided interactions can be analyzed using NLP pipelines to extract features like affective polarity, cognitive rigidity markers, and semantic themes (e.g., social comparison, externalized self-worth). These features could complement scale-based results, supporting descriptive risk characterization or triage summaries. However, their clinical validity, calibration, and fairness across populations require prospective evaluation.
CLINICAL FEASIBILITY AND INITIAL EVIDENCE
Early studies have investigated the potential of using ChatGPT and related LLMs for patient communication in surgical settings. In simulated consultations for procedures like rhinoplasty and abdominoplasty, blinded reviewers rated LLM-generated responses as comparable to, and in some aspects even more readable and comprehensive than, those written by humans[20]. Most available studies on LLMs in healthcare focus on general patient education and question-answering, rather than validated psychological assessment or outcome prediction. Nonetheless, these initial findings suggest LLMs can generate coherent, patient-friendly explanations and maintain an empathic tone. These foundational capabilities are crucial for more structured applications, such as clarifying preoperative expectations and creating triage-oriented summaries in aesthetic practice. While broader reviews of AI and machine learning in facial aesthetic surgery highlight growth in AI-supported diagnosis, prediction, and counseling, the specific contribution and clinical effectiveness of generative models remain inconsistently studied across procedures and endpoints[21].
Generative AI can be integrated into preoperative digital workflows as standalone chat interfaces or as modules within electronic intake systems, enabling patient engagement outside the time constraints of in-person consultations[22,23]. Asynchronous, conversational formats can make it easier for individuals to share information and reflect at their own pace on their motivations and expectations.
PATIENT EMPOWERMENT THROUGH AI-DRIVEN PSYCHOEDUCATION AND EXPECTATION MANAGEMENT
Preoperative psychological screening aims not only to identify elevated risk but also to promote emotional readiness and informed, preference-sensitive decision-making. In this context, generative AI can support patient empowerment by delivering tailored psychoeducation, structuring expectation clarification, and reinforcing shared decision-making in a scalable format. This is particularly relevant in aesthetic surgery, where outcomes are inherently subjective and heavily influenced by preoperative expectations, attribution styles, and perceived social factors. Patient-facing conversational systems can present educational content, prompt reflection on goals and trade-offs, and help patients articulate realistic success criteria - functions that complement, rather than replace, clinician counseling.
Expectation management is also facilitated by advances in outcome visualization. Specifically, in rhinoplasty, image-based simulation and deep learning approaches have been investigated for generating individualized postoperative appearance predictions and standardizing patient-surgeon communication regarding plausible outcomes[23]. Such tools could enhance preoperative understanding by reorienting discussions from idealized targets to anatomically and procedurally feasible ranges; however, their accuracy, generalizability, and impact on satisfaction necessitate rigorous validation. Concurrently, generative adversarial networks (GANs) and related generative imaging methods have been employed for synthetic data generation and the modeling of postoperative appearance, yet standardized development and evaluation frameworks are essential to ensure clinical validity, mitigate bias, and prevent the amplification of unrealistic expectations[24].
COGNITIVE REFRAMING AND STRUCTURED SELF-HELP SUPPORT
Beyond outcome visualization, generative AI can support preoperative preparation by providing structured psychoeducation and skills-focused self-help prompts, both grounded in cognitive-behavioral principles. In aesthetic surgery candidates, common maladaptive cognitions include all-or-nothing thinking (e.g., “If my nose isn’t perfect, the surgery was a failure”), catastrophizing (e.g., “Everyone will notice the scar”), and external validation dependency (e.g., “I need this surgery to be accepted”). Conversational systems, through guided reflection, Socratic-style questioning, and alternative appraisal prompts, can help patients articulate assumptions, consider more balanced interpretations, and define realistic success criteria. These capabilities support expectation alignment and emotional readiness during decision-making. Crucially, such modules must be framed as supportive educational and self-reflection tools, not psychotherapy, and must incorporate clear boundaries and escalation pathways for concerning symptoms or crisis signals.
This strategy aligns with patient-centered care, promoting informed participation and psychological preparedness alongside surgical planning. In practice, generative AI should function as an adjunct, extending access to standardized educational content and structured reflection beyond the clinic, while preserving clinician oversight for interpretation, risk discussion, and referral decisions. To minimize harm, implementation must prioritize safety-by-design measures, including conservative language, avoidance of diagnostic labeling, transparent disclosures, and clinician-facing summaries that highlight red-flag content needing follow-up.
DESIGN FRAMEWORK FOR AN INTEGRATED AI-POWERED PREOPERATIVE SYSTEM
While components of AI-assisted screening and education have been studied in broader contexts like mental health and general surgery, there is currently insufficient data to determine if these systems can be directly applied to aesthetic surgery patients with clearly defined efficacy or implementation boundaries. Therefore, the architecture presented here should be considered a proposed conceptual framework, not a clinically validated model.
As summarized in Figure 4, an effective future AI-enhanced preoperative system can be organized into three sequential and interlinked stages: (a) initial engagement and structured intake; (b) personalized psychoeducation and expectation clarification; and (c) clinician-facing summary and consultation support. Crucially, such a system should not function as an autonomous diagnostic or decision-making tool. Instead, it must operate within a governed clinical pathway, characterized by human oversight, non-diagnostic use, privacy protection, bias awareness, transparent clinical boundaries, and clearly defined escalation triggers for concerning signals [Figure 4].
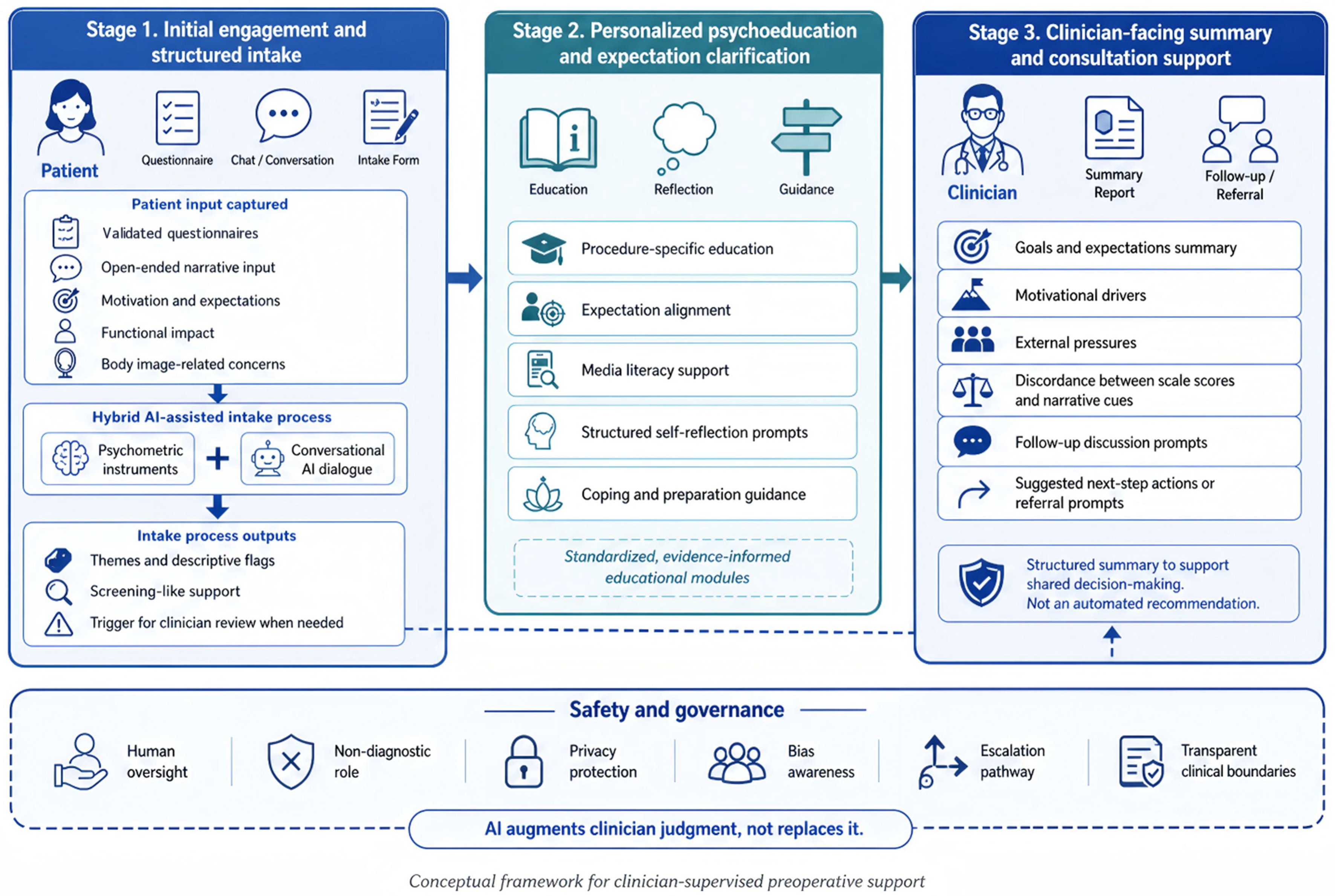
Figure 4. Conceptual framework of an integrated AI-powered preoperative system in plastic surgery. AI: Artificial intelligence.
This figure presents a proposed three-stage framework for integrating generative AI into preoperative plastic surgery care. Stage 1 involves hybrid intake, utilizing validated questionnaires and open-ended conversational input to capture patient motivations, expectations, functional impact, and body image-related concerns; Stage 2 delivers targeted psychoeducation and expectation clarification through standardized, evidence-informed support modules; Stage 3 provides clinician-facing summaries that highlight patient goals and expectations, motivational drivers, external pressures, discordance between structured scale scores and narrative cues, and prompts for follow-up discussion or referral when appropriate. The framework is conceptualized as a clinician-supervised support system, distinct from a clinically validated autonomous diagnostic or recommendation model. Its implementation must adhere to stringent safety and governance protocols, encompassing human oversight, non-diagnostic application, robust privacy protection, proactive bias awareness, clear escalation pathways, and transparent clinical boundaries.
A pragmatic architecture can be organized into three stages:
1. Initial engagement and structured intake (screening-like support): a conversational agent guides patients through a hybrid intake combining validated psychometric instruments (e.g., BDD and body image scales, as appropriate) with open-ended questions. The goal is to capture motivations, expectations, and functional impact while enabling patients to disclose sensitive concerns in a self-paced format. Outputs at this stage should be descriptive (e.g., “themes” or “flags”) rather than diagnostic labels. Predefined thresholds should trigger clinician review or referral pathways.
2. Personalized psychoeducation and expectation clarification: the system delivers targeted modules, informed by intake themes and questionnaire responses. These modules cover areas such as procedure-specific education, expectation alignment prompts, media literacy content, and structured self-help exercises grounded in cognitive-behavioral principles. For example, patients with elevated appearance-related anxiety may receive guided reflection prompts and coping skills education, while those with unrealistic expectations may be offered scenario-based trade-off explanations and visualization-guided counseling prompts. All module content must be standardized, evidence-informed, and carefully worded to avoid therapeutic claims or deterministic predictions.
3. Clinician-facing summary and consultation support: the platform generates a concise surgeon report from patient inputs, highlighting: (a) stated goals and expectations; (b) motivational drivers and external pressures; (c) discordance between scale scores and narrative cues; and (d) prompts for consultation discussion. For detected risks, the report recommends next steps (e.g., additional in-person assessment, shared decision-making aids, or mental health referral), supporting clinician judgment over automated decision-making.
PRACTICAL CLINICAL INTEGRATION AND MEDICO-LEGAL CONSIDERATIONS
To realistically incorporate such conceptual systems into everyday clinical practice, they must seamlessly align with existing preoperative workflows. Patients could interact with the AI screening tool via a secure mobile application at home or on a tablet in the waiting room before their initial consultation. This asynchronous approach saves valuable clinic time and allows patients to reflect on their motivations privately.
However, strict clinician oversight remains non-negotiable. The AI should function purely as a “triage and summary” assistant, flagging potential psychological vulnerabilities (e.g., body dysmorphic traits or unrealistic expectations) for the surgeon to explore during the face-to-face encounter. From a medico-legal perspective, integrating AI-generated outputs into patient counseling introduces novel liability risks. For instance, if an AI system fails to detect severe psychological distress, or if a surgeon overlooks an AI-generated red flag leading to postoperative psychological harm, the allocation of liability among the software developer, healthcare institution, and clinician becomes ambiguous. Therefore, clinical integration must include clear patient disclaimers: the AI is not a diagnostic tool, and ultimate responsibility for surgical clearance and psychological assessment always rests with the attending plastic surgeon.
LIMITATIONS AND ETHICAL CONSIDERATIONS
Notwithstanding its potential, the integration of generative AI into routine preoperative care presents substantial technical, ethical, and regulatory challenges, particularly in contexts involving psychologically sensitive and high-stakes decision-making. A principal concern is algorithmic bias: should training and validation data lack representativeness across demographic, cultural, and aesthetic-preference groups, model outputs may exhibit suboptimal performance for specific populations or inadvertently perpetuate existing disparities[25,26]. Both privacy and security are paramount, given that these systems may process highly sensitive narratives pertaining to body image, mental health symptoms, and social stressors. In addition, LLMs are prone to generating inaccurate or fabricated content (referred to as “hallucinations”), which is impermissible in clinical counseling contexts absent robust safeguards, rigorous validation, and comprehensive oversight[27,28]. Finally, the evolving regulatory landscape for AI-enabled tools - especially those used for screening, triage, or decision support - along with unclear accountability structures, may impede safe deployment[28].
Given that preoperative psychological assessment is a high-stakes application, it is essential to move beyond general concerns and concretely specify failure modes, potential harms, and mitigation pathways that encompass both technical controls and clinical governance [Table 2]. Crucially, these mitigations must be implemented as “safety-by-design” requirements rather than optional features.
Failure modes and safety-by-design mitigations for LLM-enabled psychological screening and patient support in plastic surgery
| Failure mode/Risk | Example in plastic surgery setting | Potential harm | Risk level (Low/Med/High) | Mitigation (technical) | Mitigation (Clinical workflow) | Monitoring/Audit |
| Hallucination | Incorrect advice about risks/contraindications | Unsafe decisions, misinformation | High | Retrieval-augmented generation, constrained templates | Clinician review for high-risk outputs | Log sampling, error reporting |
| False negative | Missed BDD/self-harm signals | Postop regret, disputes, harm | High | Red-flag classifier + thresholding | Mandatory escalation pathway | Periodic calibration vs. clinical outcomes |
| False positive | Over-flagging anxiety/BDD | Unnecessary referral, stigma | Med | Threshold tuning, explainable highlights | Confirmatory human interview | Audit FP rate |
| Bias | Beauty norms, demographic skews | Inequitable recommendations | High | Diverse training/validation, bias tests | Equity review committee | Subgroup performance dashboard |
| Privacy leakage | PHI in chat logs | Legal/ethical breach | High | Encryption, minimization, de-identification | Consent + Retention policy | Access logs, compliance audits |
| Overreliance | Patient treats AI as clinician | Delayed care | Med | Disclaimers, refusal policies | Clear handoff to clinicians | User behavior analytics |
Implicit bias warrants particular attention in aesthetic surgery, where concepts of “normality”, attractiveness, and ideal outcomes are shaped by cultural and societal norms[29]. When AI systems are trained predominantly on data reflecting a narrow demographic or aesthetic standard, they may embed biases, such as privileging certain facial proportions, skin tones, or beauty ideals. Consequently, their counseling or expectation-setting outputs might not align with diverse identities and preferences.
Addressing this challenge requires not only diverse datasets but also continuous auditing, including subgroup performance reporting and model recalibration. Furthermore, robust governance structures are essential to ensure an equity-focused review of both AI outputs and subsequent clinical actions.
In practice, fairness assessment should incorporate conservative scope boundaries, explicitly avoiding prescriptive beauty judgments. This, combined with essential clinician oversight, will help ensure that AI-mediated communication remains supportive, patient-centered, and culturally responsive.
FUTURE DIRECTIONS
To advance clinical translation, future work must transition from feasibility demonstrations to standardized validation and implementation science. We summarize key evidence gaps and propose corresponding study designs, comparators, and endpoints to support clinical validation, safety assessment, and regulatory readiness [Table 3].
Research gaps and recommended validation roadmap for generative AI in preoperative psychological care
| Gap | Why it matters | Recommended study design | Population and setting | Comparator | Primary endpoints | Secondary endpoints | Minimum reporting requirements |
| Lack of prospective validation | Current evidence mostly simulated | Prospective cohort/RCT | Pre-op clinic patients | Standard workflow | Postop satisfaction, regret | Decisional conflict, disputes | Model version, prompts, dataset, IRB |
| No gold-standard for “psych readiness” | Inconsistent outcome definition | Delphi consensus + Validation | Multi-center | Baseline tools | Validated readiness score | Adherence, dropout | Scale development reporting |
| Poor generalizability | Single-site/single language | External validation | Multi-cultural cohorts | Local screening | Subgroup performance | Fairness metrics | Demographics and subgroup results |
| Missing escalation governance | High-risk psych use-case | Implementation study | Real-world deployment | Usual care | Safety events | Triage accuracy | Escalation protocol transparency |
To achieve multimodal and context-aware assessment, future preoperative systems must move beyond text-only interaction, which often misses clinically relevant affective and behavioral signals. Such systems could therefore explore multimodal approaches, combining language-based input with additional patient-derived cues like voice or prosodic features, facial expression dynamics, response latency, and engagement patterns. As illustrated in Figure 5, integrating these signals into an AI-assisted workflow would enable exploratory multimodal fusion, analysis of affective and behavioral patterns, detection of expectation-instability cues, integration of distress-related signals, risk flagging, and clinician-supportive interpretation. These approaches would support a more contextual understanding of distress, expectation misalignment, and decisional conflict within psychologically sensitive preoperative settings. It is crucial to note, however, that these applications represent future research directions rather than clinically validated assessment systems. Their translation into plastic surgery practice will require careful calibration, privacy-preserving data capture, transparent thresholds, thorough bias assessment, robust human oversight, and clearly governed escalation pathways[30].
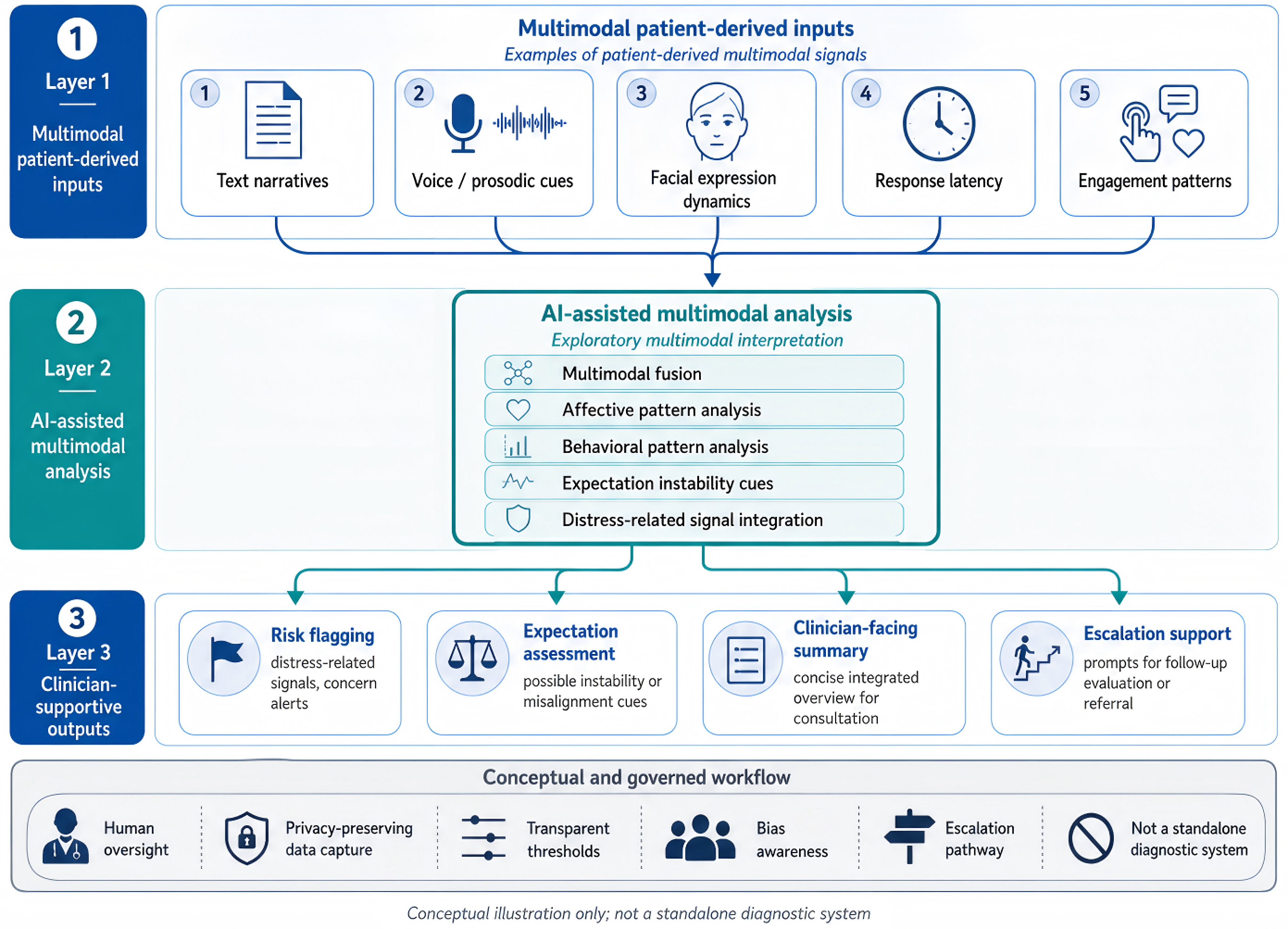
Figure 5. Conceptual framework for AI-supported multimodal preoperative assessment in plastic surgery. AI: Artificial intelligence.
This schematic illustrates a conceptual framework for future multimodal preoperative assessment support in plastic surgery. It proposes integrating various patient-derived signals - such as text narratives, voice/prosodic cues, facial expression dynamics, response latency, and engagement patterns - through exploratory AI-assisted multimodal analysis. This analysis aims to support risk flagging, expectation assessment, clinician-facing summarization, and escalation. Crucially, this framework is for conceptual illustration only; it does not represent a standalone diagnostic system, a validated psychological assessment tool, or a clinically validated autonomous platform. Any future implementation would require human oversight, privacy-preserving data capture, transparent thresholds, bias assessment, and clearly governed escalation pathways. The authors created this schematic using professional figure-preparation software based on their conceptual designs, without incorporating any third-party copyrighted material.
Privacy-preserving model development and multi-center generalizability
Federated learning and similar privacy-preserving approaches can address data-sharing limitations by training models across multiple institutions without centralizing sensitive patient data. However, deploying these federated models requires rigorous external validation, detailed subgroup performance reporting, and continuous monitoring for drift to ensure their reliability across diverse linguistic, cultural, and aesthetic contexts.
Workflow integration and longitudinal monitoring
For sustainable adoption, AI tools should be integrated modularly into existing workflows, rather than functioning as standalone chatbots. Embedding AI components within electronic medical record (EMR) intake systems, mobile preoperative guidance apps, or secure patient portals would allow for longitudinal monitoring from the initial consultation through surgery. This integration could track changes in patient expectation stability, decisional conflict, and emotional tone over time. Clinician-facing summaries would highlight meaningful changes, supporting timely follow-up without substituting for clinical judgment.
Next-generation interfaces for expectation management should combine LLM-based dialogue with validated visualization tools. Examples include 3D morphing, surgeon-guided simulation ranges, or GAN-assisted image generation constrained by anatomical plausibility. Such systems can improve patient understanding of realistic outcomes and trade-offs. Future designs must explicitly guard against “idealized output drift”, where excessively flattering or culturally narrow visuals inflate expectations. Their impact on decisional quality, satisfaction, and regret should be evaluated using predefined endpoints.
Governance, accountability, and standards
Finally, robust governance is paramount for applications involving psychologically sensitive patient interactions. This necessitates clear policies covering data use, transparency and disclosure, human oversight requirements, escalation thresholds (including crisis pathways), documentation practices, and patient rights within AI-mediated communication. Advancements will rely on standardized reporting frameworks for model versioning and prompt specifications, shared benchmarks for clinically meaningful endpoints, and alignment with evolving regulatory pathways for AI-enabled decision support[30].
CONCLUSION
AI is increasingly transforming plastic and reconstructive surgery, impacting not only technical planning and prediction but also communication and decision-making in elective aesthetic care. Generative AI, particularly LLMs, shows promise as a patient-facing interface, supporting preoperative conversations about motivation, expectations, and psychosocial readiness.
Despite the common occurrence of psychological risk factors linked to postoperative satisfaction and regret, routine practice consistently shows a gap: structured assessment and preparatory support are often inconsistently delivered. This inconsistency stems from time constraints, limited specialist availability, and barriers to patient disclosure. Existing tools, while valuable, may not adequately account for surgery-specific factors such as appearance-based perfectionism, social comparison, externally driven motivation, and unstable expectations.
Emerging evidence suggests that LLM-enabled systems can facilitate screening-like intake interactions, deliver tailored psychoeducation, and structure expectation clarification in an accessible, low-stigma format. Combining validated psychometric instruments with open-ended dialogue in hybrid designs may help contextualize patient concerns and generate clinician-facing summaries, guiding targeted discussion during consultation. These capabilities are especially relevant for high-volume settings, where asynchronous engagement can extend support beyond the clinic visit.
However, psychologically sensitive applications necessitate conservative scope boundaries and safety-by-design governance. Risks such as hallucinated content, bias (including aesthetic normativity), privacy exposure, and overreliance demand human oversight, clear escalation pathways, transparent disclosure, and ongoing auditing. Crucially, generative AI should serve as an adjunct that augments - rather than replaces - clinical judgment, empathy, and referral decision-making.
Future progress hinges on multidisciplinary collaboration to establish standardized validation endpoints, implementation protocols, and governance frameworks that align with evolving regulatory expectations. Through rigorous prospective evaluation and responsible deployment, generative AI can become a clinically meaningful component of preoperative care, supporting psychological preparedness and patient agency as integral contributors to positive aesthetic surgical outcomes[31].
DECLARATIONS
Authors’ contributions
Wrote and edited the manuscript: Li Z, Xiong T
Contributed to conceptualization and AI framework design: Chishti MNUH, Chen Y, Li W
Performed literature search and data collection: Zeng L, Yu T
Participated in manuscript revision: Li L
Wrote and edited the manuscript, supervised the study, and acquired funding: Liao J
Availability of data and materials
Not applicable.
AI and AI-assisted tools statement
During the preparation and revision of this manuscript, the AI tool ChatGPT (OpenAI; versions GPT-5.3 to GPT-5.5) was used solely for language editing and preliminary conceptual guidance for schematic figure design. The final figures were manually redrawn, edited, and finalized by the authors using professional figure-preparation software. The tool did not influence the study design, data collection, analysis, interpretation, or the scientific content of the work. All authors take full responsibility for the accuracy, integrity, and final content of the manuscript and figures.
Financial support and sponsorship
This work was supported by the Education Ministry’s Collaborative Education Program with Industry, China (No.220603565172212), and the School-level Educational Reform Project at the University of South China, China (No.2022CY009).
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Atiyeh B, Emsieh S, Hakim C, Chalhoub R. A narrative review of artificial intelligence (AI) for objective assessment of aesthetic endpoints in plastic surgery. Aesthetic Plast Surg. 2023;47:2862-73.
2. Mansoor M, Ibrahim AF. The transformative role of artificial intelligence in plastic and reconstructive surgery: challenges and opportunities. J Clin Med. 2025;14:2698.
3. Gomez-Cabello CA, Borna S, Pressman SM, et al. Artificial intelligence in postoperative care: assessing large language models for patient recommendations in plastic surgery. Healthcare. 2024;12:1083.
4. Barone M, De Bernardis R, Persichetti P. Artificial intelligence in plastic surgery: analysis of applications, perspectives, and psychological impact. Aesthetic Plast Surg. 2025;49:1637-9.
5. Peet BM, Sidoti A, Allen RJ Jr, Nelson JA, Graziano F. Artificial intelligence in breast reconstruction: enhancing surgical planning, aesthetic outcomes, and patient-centered care. J Clin Med. 2025;14:7821.
6. Xie Y, Seth I, Hunter-Smith DJ, Rozen WM, Ross R, Lee M. Aesthetic surgery advice and counseling from artificial intelligence: a rhinoplasty consultation with ChatGPT. Aesthetic Plast Surg. 2023;47:1985-93.
7. Hassan AM, Rajesh A, Asaad M, et al. Artificial intelligence and machine learning in prediction of surgical complications: current state, applications, and implications. Am Surg. 2023;89:25-30.
8. Spoer DL, Kiene JM, Dekker PK, et al. A systematic review of artificial intelligence applications in plastic surgery: looking to the future. Plast Reconstr Surg Glob Open. 2022;10:e4608.
9. Bukret WE. Prospective evaluation of an automated rule-based screening tool for body dysmorphic disorder in aesthetic surgery. Plast Reconstr Surg Glob Open. 2025;13:e7217.
10. Zhang T, Schoene AM, Ji S, Ananiadou S. Natural language processing applied to mental illness detection: a narrative review. NPJ Digit Med. 2022;5:46.
11. Choi E, Leonard KW, Jassal JS, Levin AM, Ramachandra V, Jones LR. Artificial intelligence in facial plastic surgery: a review of current applications, future applications, and ethical considerations. Facial Plast Surg. 2023;39:454-9.
12. Leypold T, Schäfer B, Boos A, Beier JP. Can AI think like a plastic surgeon? Evaluating GPT-4’s clinical judgment in reconstructive procedures of the upper extremity. Plast Reconstr Surg Glob Open. 2023;11:e5471.
13. Janumpally R, Nanua S, Ngo A, Youens K. Generative artificial intelligence in graduate medical education. Front Med. 2024;11:1525604.
14. Jayakumar P, Moore MG, Furlough KA, et al. Comparison of an artificial intelligence-enabled patient decision aid vs educational material on decision quality, shared decision-making, patient experience, and functional outcomes in adults with knee osteoarthritis: a randomized clinical trial. JAMA Netw Open. 2021;4:e2037107.
15. Liu HY, Alessandri-Bonetti M, Arellano JA, Egro FM. Can ChatGPT be the plastic surgeon’s new digital assistant? A bibliometric analysis and scoping review of ChatGPT in plastic surgery literature. Aesthetic Plast Surg. 2024;48:1644-52.
16. Copeland-Halperin LR, O’Brien L, Copeland M. Evaluation of artificial intelligence-generated responses to common plastic surgery questions. Plast Reconstr Surg Glob Open. 2023;11:e5226.
17. Decker H, Trang K, Ramirez J, et al. Large language model-based chatbot vs surgeon-generated informed consent documentation for common procedures. JAMA Netw Open. 2023;6:e2336997.
18. Lin SJ, Sun CY, Chen DN, et al. Perioperative application of chatbots: a systematic review and meta-analysis. BMJ Health Care Inform. 2024;31:e100985.
19. Vallurupalli M, Shah ND, Vyas RM. Validation of ChatGPT 3.5 as a tool to optimize readability of patient-facing craniofacial education materials. Plast Reconstr Surg Glob Open. 2024;12:e5575.
20. Kim YJ, Kelley BP, Nasser JS, Chung KC. Implementing precision medicine and artificial intelligence in plastic surgery: concepts and future prospects. Plast Reconstr Surg Glob Open. 2019;7:e2113.
21. Stephanian B, Karki S, Debnath K, et al. Role of artificial intelligence and machine learning in facial aesthetic surgery: a systematic review. Facial Plast Surg Aesthet Med. 2024;26:679-705.
22. Kania B, Montecinos K, Goldberg DJ. Artificial intelligence in cosmetic dermatology. J Cosmet Dermatol. 2024;23:3305-11.
23. Eldaly AS, Avila FR, Torres-Guzman RA, et al. Simulation and artificial intelligence in rhinoplasty: a systematic review. Aesthetic Plast Surg. 2022;46:2368-77.
24. Zargaran A, Sousi S, Glynou SP, Mortada H, Zargaran D, Mosahebi A. A systematic review of generative adversarial networks (GANs) in plastic surgery. J Plast Reconstr Aesthet Surg. 2024;95:377-85.
25. Kohli M, Geis R. Ethics, artificial intelligence, and radiology. J Am Coll Radiol. 2018;15:1317-9.
26. Leslie D, Mazumder A, Peppin A, Wolters MK, Hagerty A. Does “AI” stand for augmenting inequality in the era of covid-19 healthcare? BMJ. 2021;372:n304.
27. Warraich HJ, Tazbaz T, Califf RM. FDA perspective on the regulation of artificial intelligence in health care and biomedicine. JAMA. 2025;333:241-7.
28. Zaidi D, Miller T. Implicit bias and machine learning in health care. South Med J. 2023;116:62-4.
29. Taib BG, Karwath A, Wensley K, Minku L, Gkoutos GV, Moiemen N. Artificial intelligence in the management and treatment of burns: a systematic review and meta-analyses. J Plast Reconstr Aesthet Surg. 2023;77:133-61.
30. Carrión H, Jafari M, Bagood MD, Yang HY, Isseroff RR, Gomez M. Automatic wound detection and size estimation using deep learning algorithms. PLoS Comput Biol. 2022;18:e1009852.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].