
SGLT2 inhibitors in patients with HFpEF: how old is too old?
 0
0
Heart failure with preserved ejection fraction (HFpEF) is increasingly recognized as a heterogeneous, systemic clinical syndrome. The complex nature of HFpEF makes it a diagnostic and therapeutic challenge. Recently, sodium-glucose cotransporter-2 (SGLT2) inhibitors have emerged as a promising therapy for HFpEF, as the EMPEROR-Preserved trial demonstrated that empagliflozin reduces the risk of the composite cardiovascular (CV) endpoint of death or heart failure (HF) hospitalization in HF patients with LVEF > 40%[1]. Therefore, SGLT2 inhibitors are listed in the 2022 AHA/ACC/HFSA HF guidelines as a class IIa recommendation for treating patients with HFpEF[2]. This marks a momentous and exciting advance in the management of HFpEF. However, many uncertainties remain while implementing this novel therapy into real-world clinical practice.
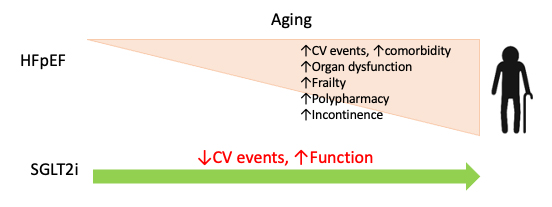
HFpEF is considered a geriatric syndrome, as most patients with HFpEF are ≥ 65 years old with multiple comorbidities and limited functional status[3]. Therefore, caring for HFpEF patients inevitably entails unique challenges. Given the increased burden of comorbidities and declining organ function associated with aging, will the benefits of SGLT2 inhibitors decline in the elderly? It is well known that older patients have poor tolerance to hypotension and hypoglycemia; will this make them particularly sensitive to side effects associated with SGLT2 inhibitors? Incontinence is common in the elderly and associated with an increased risk of urinary tract infection (UTI); will this pose a particular challenge for implementing SGLT2 inhibitors? Lastly, and perhaps most importantly, as HFpEF is associated with significant frailty and debilitation[4], it is critical to assess the impact of SGLT2 inhibitors on patient functional status. A recent study by Bohm et al. provided valuable insights into these issues[5].
In a post hoc analysis of the EMPEROR-Preserved trial, these investigators examined the treatment effect size of empagliflozin across pre-specified age subgroups. Participants were divided into four groups (age
Preservation of function and independence is one of the core values of geriatric care and an important goal for HFpEF management[3]. Empagliflozin has been shown to improve health-related quality of life (HRQoL) measured by Kansas City Cardiomyopathy Questionnaire (KCCQ) scores in HFpEF patients regardless of baseline functional status[7]. In the current study, the authors demonstrated that this beneficial effect is again maintained across all ages[5]. Numerically, the improvement in KCCQ score appeared particularly early in the very elderly group (≥ 80), as compared with other age groups, and was maintained throughout the study period. This is of particular importance as poor functional status is strongly associated with mortality in the elderly[8]. Of note, although the overall average improvement in KCCQ score is modest (1-2 points), the authors pointed out that a significant proportion of patients achieved changes of > 5 points, which reflect clinically meaningful improvements in functional status.
Polypharmacy is common in older patients, and the elderly are particularly susceptible to medication-associated side effects. The majority of participants in the EMPEROR-Preserved trial were concurrently taking commonly prescribed CV medications, including ARB/ACEi, beta-blockers, and statins, representing a typical population seen in clinical practice[1]. As SGLT2 inhibitors increase glucose excretion in the urine, there are concerns regarding the risk of UTI and infections in the genital area in the elderly, given the high prevalence of incontinence in this population. Of note, no significant increases in the profile and incidence of side effects were observed between treatment and placebo groups across all ages, suggesting a satisfactory safety profile. Furthermore, the beneficial effect of empagliflozin in mitigating eGFR decline was similarly maintained across all age groups.
In summary, the study by Bohm et al. provides evidence that empagliflozin is efficacious and safe in patients with HFpEF across all adult age groups, including the very elderly (≥ 80 years old)[5]. The benefits of SGLT2 inhibitors observed in patients with heart failure across a wide spectrum of LVEF, diabetes status, baseline functional status, and age group[5-7,9] suggest its wide and continuously expanding clinical indication and marks a significant achievement in cardiovascular medicine. Whereas the exact molecular mechanisms underlying the beneficial effects of SGLT2 inhibitors remain unclear, their wide-ranging benefits raise the possibility that they work via fundamental cellular pathways that benefit health and longevity. Consistent with this notion, recent studies have demonstrated that SGLT2 inhibitors are intimately connected with pathways such as cell energy, senescence, autophagy, etc.[10]. Additional in-depth mechanistic studies are needed to elucidate molecular mechanisms governing SGLT2 inhibition-dependent benefits to the cardiovascular system.
DECLARATIONS
Authors’ contributionsThe author contributed solely to the article.
Availability of data and materialsNot applicable.
Financial support and sponsorshipThis work was supported by American Heart Association, 851313 (Tong D.), and the NIH, K08HL157697 (Tong D.).
Conflicts of interestThe author declared that there are no conflicts of interest.
Ethical approval and consent to participateNot applicable.
Consent for publicationNot applicable.
Copyright© The Author(s) 2022.
REFERENCES
1. Anker SD, Butler J, Filippatos G, et al. Empagliflozin in heart failure with a preserved ejection fraction. N Engl J Med 2021;385:1451-61.
2. Committee Members. ACC/AHA joint committee members. 2022 AHA/ACC/HFSA guideline for the management of heart failure. J Card Fail 2022;28:e1-e167.
3. Upadhya B, Pisani B, Kitzman DW. Evolution of a geriatric syndrome: pathophysiology and treatment of heart failure with preserved ejection fraction. J Am Geriatr Soc 2017;65:2431-40.
4. Sanders NA, Supiano MA, Lewis EF, et al. The frailty syndrome and outcomes in the TOPCAT trial. Eur J Heart Fail 2018;20:1570-7.
5. Böhm M, Butler J, Filippatos G, et al. Empagliflozin improves outcomes in patients with heart failure and preserved ejection fraction irrespective of age. J Am Coll Cardiol 2022;80:1-18.
6. Butler J, Packer M, Filippatos G, et al. Effect of empagliflozin in patients with heart failure across the spectrum of left ventricular ejection fraction. Eur Heart J 2022;43:416-26.
7. Butler J, Filippatos G, Jamal Siddiqi T, et al. Empagliflozin, Health Status, and Quality of Life in Patients With Heart Failure and Preserved Ejection Fraction: The EMPEROR-Preserved Trial. Circulation 2022;145:184-93.
8. Goldfarb M, Sheppard R, Afilalo J. Prognostic and Therapeutic Implications of Frailty in Older Adults with Heart Failure. Curr Cardiol Rep 2015;17:92.
9. Filippatos G, Butler J, Farmakis D, et al. Empagliflozin for heart failure with preserved left ventricular ejection fraction with and without diabetes. Circulation 2022; doi: 10.1161/CIRCULATIONAHA.122.059785.
Cite This Article
Export citation file: BibTeX | RIS
OAE Style
Tong D. SGLT2 inhibitors in patients with HFpEF: how old is too old?. J Cardiovasc Aging 2022;2:41. http://dx.doi.org/10.20517/jca.2022.30
AMA Style
Tong D. SGLT2 inhibitors in patients with HFpEF: how old is too old?. The Journal of Cardiovascular Aging. 2022; 2(4): 41. http://dx.doi.org/10.20517/jca.2022.30
Chicago/Turabian Style
Tong, Dan. 2022. "SGLT2 inhibitors in patients with HFpEF: how old is too old?" The Journal of Cardiovascular Aging. 2, no.4: 41. http://dx.doi.org/10.20517/jca.2022.30
ACS Style
Tong, D. SGLT2 inhibitors in patients with HFpEF: how old is too old?. J. Cardiovasc. Aging. 2022, 2, 41. http://dx.doi.org/10.20517/jca.2022.30
About This Article
Copyright

Data & Comments
Data
0

 Cite This Article 3 clicks
Cite This Article 3 clicks

 Like This Article 5
likes
Like This Article 5
likes







Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.