


Predictive modeling and external validation of late atrial fibrillation recurrence following catheter ablation
 0
0 Abstract
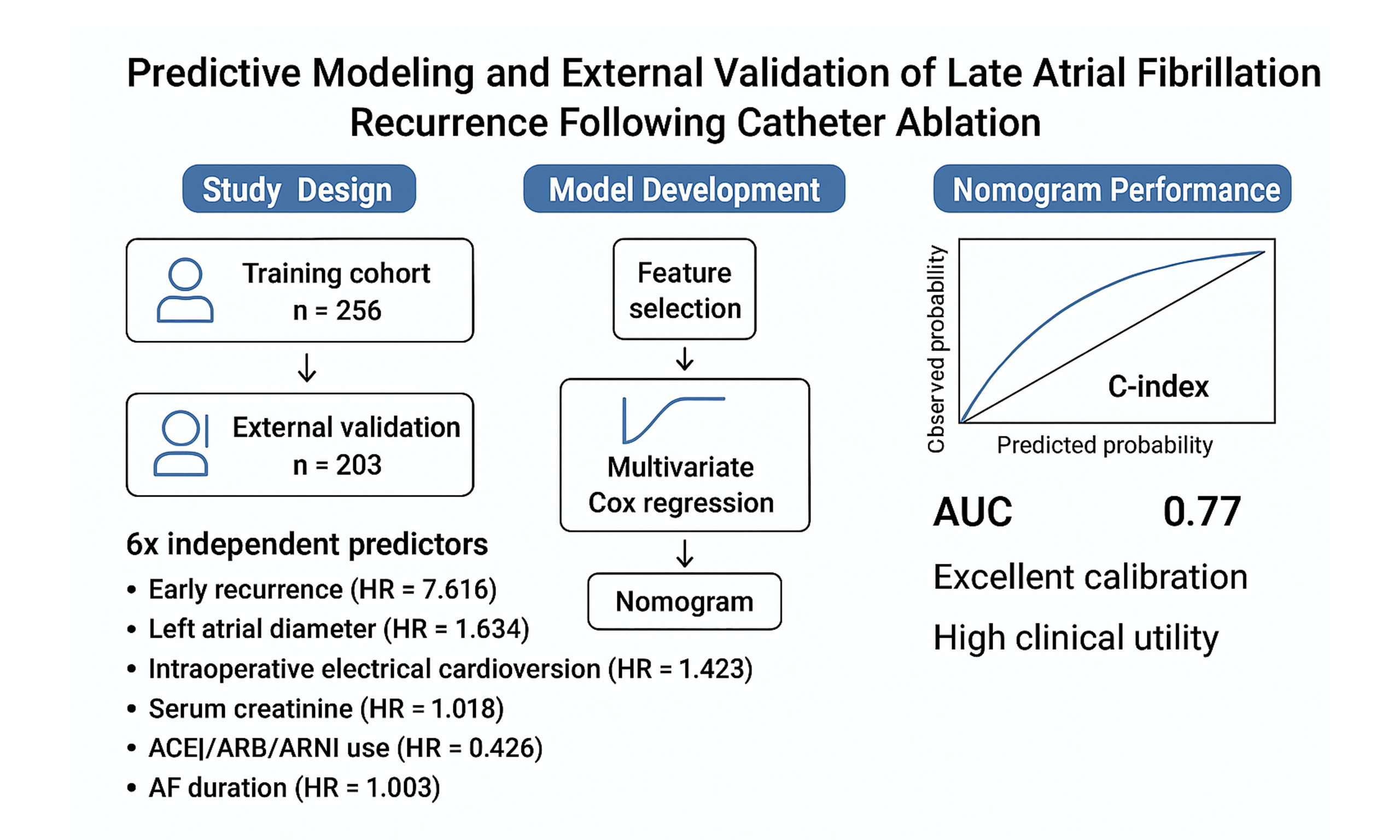
Aim: To identify factors associated with late atrial fibrillation (AF) recurrence after radiofrequency catheter ablation and to develop a nomogram for individualized risk prediction, followed by external validation in an independent cohort.
Methods: We conducted a retrospective cohort study of patients with AF who underwent catheter ablation at Tongji Hospital (training cohort, January 2020-December 2022) and the Second Hospital of Lanzhou University (validation cohort, June 2020-June 2023). Follow-up visits were scheduled at 1, 3, 6, 12, and 18 months after the procedure. Candidate predictors were identified using the Boruta algorithm and the least absolute shrinkage and selection operator. Selected variables were then entered into multivariable Cox proportional hazards models. Model performance was evaluated using Harrell’s C-index, time-dependent area under the receiver operating characteristic curve, calibration plots, and decision curve analysis.
Results: A total of 256 patients in the training cohort and 203 in the validation cohort were included, with a median follow-up of 12 months. Late AF recurrence occurred in 21.9% and 21.2% of patients, respectively. Six variables were included in the final model: early recurrence (HR = 7.616), left atrial diameter (HR = 1.684), intraoperative electrical cardioversion (HR = 1.423), serum creatinine (HR = 1.018), use of angiotensin-converting enzyme inhibitor (ACEI)/angiotensin receptor blocker (ARB)/angiotensin receptor-neprilysin inhibitor (ARNI) (HR = 0.426), and AF duration (HR = 1.003). The nomogram showed good discrimination, calibration, and clinical usefulness in both cohorts.
Conclusion: We developed and externally validated a six-variable nomogram for predicting late AF recurrence after catheter ablation. This model may support individualized risk stratification and guide post-ablation management.
Keywords
INTRODUCTION
Atrial fibrillation (AF) is one of the most common cardiac arrhythmias worldwide. Recent epidemiological data estimate a global adult prevalence of approximately 0.5%, representing a marked increase over the past two decades[1]. AF is associated with an elevated risk of thromboembolic stroke, heart failure, and premature mortality, imposing a substantial burden on both patients and healthcare systems[2].
In addition to anticoagulation and rate control, rhythm control has emerged as an important therapeutic strategy to maintain sinus rhythm and improve long-term outcomes[3]. Among rhythm-control interventions, radiofrequency catheter ablation (RFCA) is widely recognized as an effective treatment option[4-6].
Despite advances in ablation techniques, AF recurrence remains common after RFCA. Approximately 20%-40% of patients experience recurrence within the first year[7]. Long-term follow-up studies indicate that recurrence rates vary according to AF type and duration of follow-up. For example, recurrence ranges from 11%-29% over five years in patients with paroxysmal AF, and may reach up to 70% in those with persistent AF[8,9]. These findings underscore the need for improved risk stratification to optimize procedural outcomes and guide post-ablation management.
Several studies have explored predictors of AF recurrence and atrial remodeling, leading to the development of risk scores such as MB-LATER, APPLE, CAAP-AF, and ATLAS[10-13]. However, these scores are based on a limited number of clinical variables and generally demonstrate only moderate predictive performance across different populations. Therefore, there is still a need for more comprehensive models with robust external validation.
This study aimed to identify factors associated with late AF recurrence after catheter ablation and to develop and externally validate a nomogram for individualized risk prediction. We also evaluated the prognostic value of intraoperative electrical cardioversion (ECV), a relatively underexplored procedural variable, within a multivariable prediction model.
METHODS
Patient population
We conducted a retrospective study of consecutive patients with AF who underwent RFCA at two tertiary centers. The cohort from Tongji Hospital (January 2020-December 2022) was used as the training set, while the cohort from the Second Hospital of Lanzhou University (June 2020-June 2023) served as the external validation set.
Inclusion criteria were as follows: (i) a diagnosis of AF according to the 2020 European Society of Cardiology (ESC) guidelines; (ii) eligibility for RFCA based on standard clinical indications; and (iii) a minimum follow-up duration of 6 months. Exclusion criteria were as follows: (i) severe pulmonary disease, hepatic or renal insufficiency, coagulation disorders, or advanced heart failure that precluded ablation; (ii) missing key baseline or outcome data; (iii) significant bradyarrhythmias (e.g., sick sinus syndrome or third-degree atrioventricular block); (iv) left atrial appendage or mural thrombus detected by transesophageal echocardiography; and (v) valvular AF.
Baseline clinical, laboratory, imaging, and electrophysiological data were extracted from electronic medical records. Data collection was performed by trained investigators and verified for accuracy.
AF was classified as paroxysmal if episodes terminated spontaneously or with intervention within 7 days. Non-paroxysmal AF included persistent AF (lasting > 7 days) and long-standing persistent AF (lasting > 12 months in patients undergoing a rhythm control strategy)[14].
Antiarrhythmic drugs, except for amiodarone, were discontinued at least five half-lives before ablation. All patients received guideline-directed anticoagulation prior to the procedure. Transesophageal echocardiography was performed before ablation to exclude left atrial thrombus. After ablation, patients with non-paroxysmal AF routinely received short-term antiarrhythmic therapy (amiodarone or propafenone) during the blanking period, whereas in patients with paroxysmal AF, therapy was prescribed at the discretion of the treating physician.
The study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committees of Tongji Hospital (TJ-IRB202404056) and the Second Hospital of Lanzhou University (2024A-1246). Given the retrospective study design, the requirement for informed consent was waived by the institutional review boards. This study was designed and reported in accordance with the TRIPOD guidelines for multivariable prediction models to enhance transparency and reproducibility[15]. A total of 459 eligible patients were included. The participant selection process is shown in Figure 1.
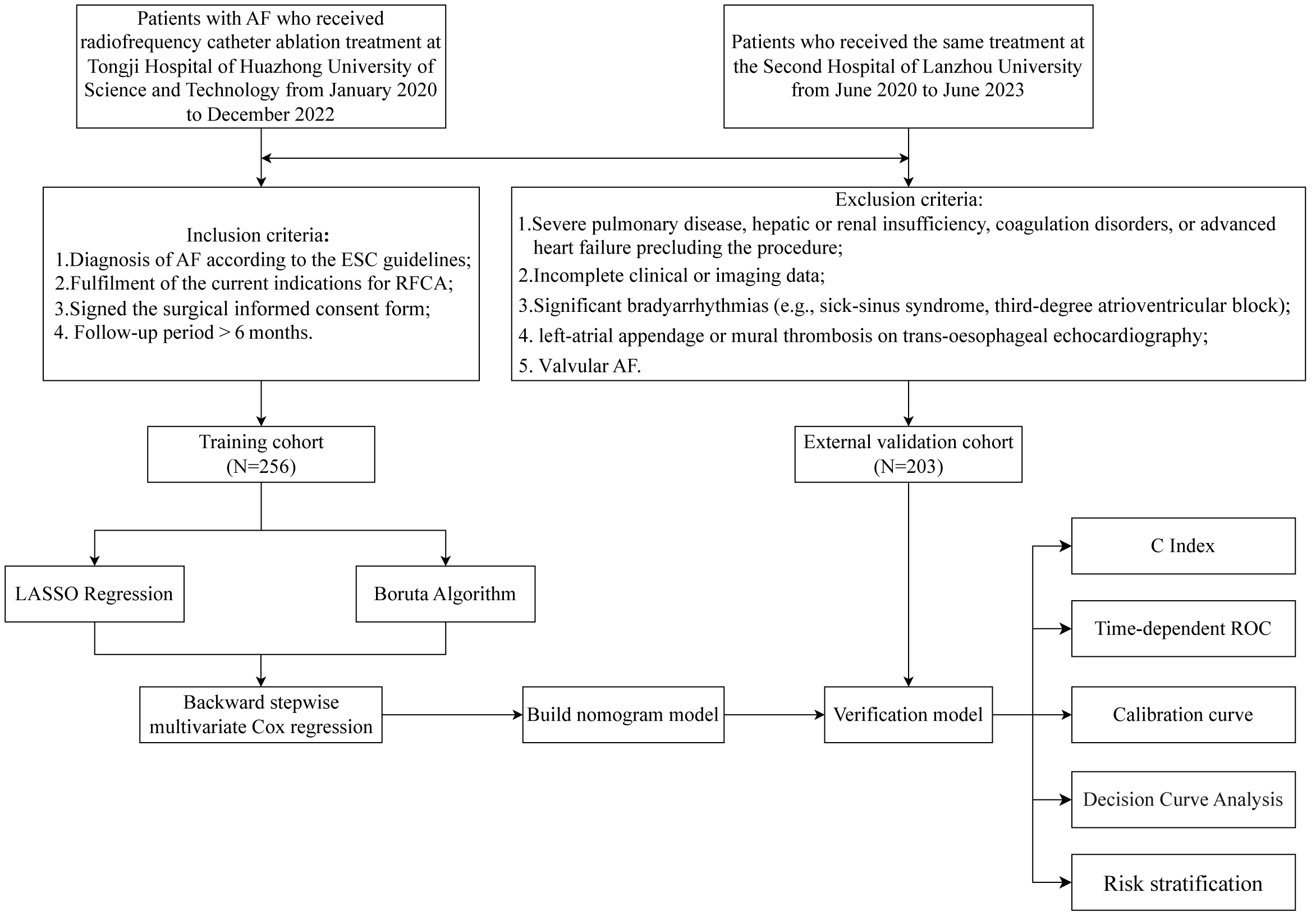
Figure 1. Flow diagram of study design.
Electrophysiological study and catheter ablation procedure
All procedures were performed using a three-dimensional electroanatomical mapping system. In patients with paroxysmal AF, circumferential pulmonary vein isolation (CPVI) was performed as the cornerstone of the ablation strategy. In patients with non-paroxysmal AF, additional linear ablation was performed after CPVI at the operator’s discretion, based on institutional protocols and substrate characteristics. These additional lesions included a left atrial roof line, posterior inferior wall lines (“roof and floor” lines), mitral isthmus line, and/or cavotricuspid isthmus line, as clinically indicated.
If AF persisted after completion of the planned ablation strategy, synchronized direct current cardioversion (150 or 200 J) was performed to restore sinus rhythm. Cardioversion was systematically applied to all patients who remained in AF at the end of the procedure, rather than being performed selectively.
Intraprocedural anticoagulation was maintained with intravenous heparin to achieve an activated clotting time (ACT) of 250-350 seconds. After ablation, all patients underwent continuous electrocardiographic monitoring for at least 24 h.
Data collection and extraction
Candidate variables were pre-specified based on prior literature, clinical relevance, and availability in routine practice[16]. A comprehensive set of demographic, clinical, laboratory, and procedural variables was collected to identify potential predictors of AF recurrence.
Demographic variables included age, sex, smoking status, and alcohol consumption. Clinical and echocardiographic variables included body mass index (BMI), blood pressure (systolic and diastolic), resting heart rate, left atrial diameter, and left ventricular ejection fraction (LVEF). Laboratory variables included hemoglobin, C-reactive protein (CRP), serum creatinine, N-terminal pro-B-type natriuretic peptide (NT-proBNP), thyroid hormones (TSH, FT4, and FT3), and glycated hemoglobin (HbA1c).
AF-related variables included AF duration, AF type (paroxysmal vs. non-paroxysmal), intraoperative cardioversion, and early AF recurrence. Comorbidities included heart failure, hypertension, diabetes mellitus, ischemic stroke or transient ischemic attack, and coronary artery disease. Perioperative medications included ACEIs, ARBs, ARNIs, β-blockers, anticoagulants, statins, and sodium-glucose cotransporter-2 inhibitors (SGLT2i). Procedural characteristics included total ablation duration.
Supplementary Figure 1 shows the proportion of missing values for each variable. Variables with more than 30% missing data were excluded. The remaining missing values were handled using the imputation methods described below.
Follow-up
Patients were followed at 1, 3, 6, 12, and 18 months after catheter ablation through outpatient visits or structured telephone interviews using a standardized questionnaire. Follow-up was completed in December 2024, and duration was calculated in months. At each visit, postoperative symptoms were assessed, and a standard 12-lead electrocardiogram (ECG) was obtained or reviewed. Additional 24-h Holter monitoring was performed when clinically indicated. A blanking period of 3 months after ablation was applied. AF recurrence was defined as any documented episode of atrial tachyarrhythmia, including AF, atrial flutter, or atrial tachycardia, lasting ≥ 30 s.
Early recurrence was defined as any atrial tachyarrhythmia occurring within the first 3 months after ablation, whereas late recurrence was defined as events occurring thereafter[17]. During the blanking period, short-term antiarrhythmic therapy was permitted in accordance with standard practice. Early recurrence was treated as a potential prognostic indicator rather than procedural failure. All study endpoints were adjudicated by a blinded, independent Clinical Events Committee.
Construction and validation of clinical prediction model
A nomogram was developed based on the final multivariable model to provide individualized estimates of AF recurrence risk[18-20]. In the training cohort, candidate variables were initially screened using the least absolute shrinkage and selection operator (LASSO) regression and the Boruta algorithm for dimensionality reduction. Variables identified by these methods, together with clinically relevant factors, were then entered into a multivariable Cox proportional hazards model. Backward stepwise selection was applied, guided by the Akaike Information Criterion (AIC), which emphasizes overall model fit rather than individual P values. Hazard ratios (HRs) with 95% confidence intervals (CIs) were estimated, and the proportional hazards assumption was assessed before finalizing the model.
Based on the final Cox model, a nomogram was developed to estimate the probability of AF recurrence at 6, 12, and 18 months. Model performance was assessed using Harrell’s C-index and time-dependent area under the receiver operating characteristic curve (AUC). Calibration was evaluated by comparing predicted and observed recurrence rates using calibration plots. Decision curve analysis (DCA) was performed to assess the potential clinical benefit across a range of decision thresholds[21,22]. Internal validation was conducted in the training cohort, and external validation was performed in the independent validation cohort.
Statistical analysis
Continuous variables were tested for normality using the Shapiro-Wilk test. Normally distributed variables were summarized as mean ± standard deviation (SD) and compared using the Student’s t-test, whereas non-normally distributed variables were presented as median (interquartile range, IQR) and compared using the Mann-Whitney U test. Categorical variables were expressed as counts and percentages and compared using the chi-square test or Fisher’s exact test, as appropriate.
Variables with less than 30% missing data were imputed using the MissForest method, whereas variables with more than 30% missing data were excluded from further analysis[23]. Missing data were assumed to be missing at random. Imputation performance was evaluated using the normalized root mean square error (NRMSE) for continuous variables and the proportion of falsely classified entries (PFC) for categorical variables. The overall proportion of missing data is presented in Supplementary Figure 1.
Multivariable modeling was performed using R software (version 4.4.2). The proportional hazards assumption for the Cox model was assessed prior to model fitting. Model performance metrics, including the C-index and time-dependent AUC, were estimated with corresponding 95% confidence intervals. Internal validation was conducted using bootstrap resampling to reduce optimism bias. To minimize the risk of overfitting, variable selection was guided by a combination of data-driven methods and clinical relevance. A two-sided P value < 0.05 was considered statistically significant.
RESULTS
Patient characteristics
A total of 459 eligible patients with AF were included, comprising 256 in the training cohort and 203 in the external validation cohort. In the training cohort, 157 patients (61.3%) were male and 99 (38.7%) were female, with a median age of 64 years [Table 1]. Compared with patients without recurrence, those with late AF recurrence had a larger left atrial diameter (4.54 ± 0.78 cm vs. 4.24 ± 0.67 cm) and a longer AF duration [24.0 (11.5-51.0) months vs. 12.0 (3.0-36.0) months]. Patients with recurrence also showed mildly elevated liver enzymes, including higher alanine aminotransferase (ALT) [22.0 (17.0-34.25) vs. 19.5 (15.0-26.0) U/L] and aspartate aminotransferase (AST) levels [23.0 (19.0-29.0) vs. 21.0 (18.0-25.0) U/L]. Serum creatinine levels were also higher [79.5 (72.0-94.0) vs. 77.0 (66.8-89.0) µmol/L], along with a greater prevalence of renal insufficiency (17.9% vs. 6.5%). In terms of procedural and clinical characteristics, intraoperative ECV was more frequently performed in the recurrence group (48.2% vs. 27.5%). Early recurrence during the blanking period was also more common in these patients (32.1% vs. 5.0%).
Baseline clinical and demographic characteristics according to recurrence outcomes in training cohort
| Variables | Total (n = 256) | No (n = 200) | Yes (n = 56) | P |
| Sex, n(%) | 0.839 | |||
| Female | 99 (38.67) | 78 (39.00) | 21 (37.50) | |
| Male | 157 (61.33) | 122 (61.00) | 35 (62.50) | |
| Age (years) | 64.00 (57.00, 70.00) | 64.00 (57.00, 70.00) | 66.00 (59.75, 70.25) | 0.336 |
| BMI (kg/m2) | 24.55 (22.41, 26.44) | 24.51 (22.41, 26.54) | 24.64 (22.61, 26.32) | 0.821 |
| SBP (mmHg) | 126.00 (116.00, 139.00) | 126.00 (116.75, 139.00) | 125.50 (114.50, 138.00) | 0.641 |
| DBP (mmHg) | 82.00 (74.00, 88.00) | 82.50 (73.75, 88.25) | 81.50 (74.00, 86.50) | 0.402 |
| Pulse (beats/min) | 76.00 (67.00, 88.00) | 76.00 (67.00, 87.00) | 75.00 (65.50, 94.00) | 0.963 |
| LAD (cm) | 4.31 ± 0.71 | 4.24 ± 0.67 | 4.54 ± 0.78 | 0.005 |
| Hb (g/L) | 135.86 ± 16.35 | 136.28 ± 15.97 | 134.34 ± 17.73 | 0.434 |
| CHA2DS2-VASC | 2.00 (1.00, 3.00) | 2.00 (1.00, 3.00) | 2.00 (1.00, 3.00) | 0.587 |
| AF course (months) | 12.00 (3.00, 36.00) | 12.00 (3.00, 36.00) | 24.00 (11.50, 51.00) | 0.041 |
| Surgery time (hours) | 2.16 (2.00, 2.60) | 2.16 (2.00, 2.58) | 2.29 (2.00, 2.69) | 0.530 |
| CRP (mg/L) | 1.10 (0.60, 2.00) | 1.10 (0.60, 2.00) | 1.10 (0.50, 2.00) | 0.713 |
| ALT (IU/L) | 20.00 (16.00, 28.00) | 19.50 (15.00, 26.00) | 22.00 (17.00, 34.25) | 0.029 |
| AST (IU/L) | 21.00 (18.00, 25.00) | 21.00 (18.00, 25.00) | 23.00 (19.00, 29.00) | 0.029 |
| NT-proBNP (pg/mL) | 363.00 (151.75, 730.75) | 363.00 (139.00, 705.75) | 363.00 (223.00, 847.50) | 0.136 |
| Cr (μmol/L) | 77.00 (68.00, 90.25) | 77.00 (66.75, 89.00) | 79.50 (72.00, 94.00) | 0.017 |
| TSH (μIU/mL) | 2.04 (1.47, 2.76) | 2.04 (1.43, 2.81) | 2.04 (1.62, 2.69) | 0.778 |
| FT4 (pmol/L) | 1.19 (1.02, 15.22) | 1.19 (1.02, 15.33) | 1.19 (1.08, 15.12) | 0.702 |
| FT3 (pmol/L) | 2.83 (2.57, 4.29) | 2.83 (2.58, 4.29) | 2.83 (2.50, 4.21) | 0.762 |
| HbA1c | 5.80 (5.50, 6.00) | 5.80 (5.50, 5.93) | 5.80 (5.50, 6.00) | 0.946 |
| EF (%) | 59.00 (55.00, 64.00) | 59.00 (55.00, 64.00) | 58.00 (50.75, 63.00) | 0.212 |
| ECV, n(%) | 0.003 | |||
| No | 174 (67.97) | 145 (72.50) | 29 (51.79) | |
| Yes | 82 (32.03) | 55 (27.50) | 27 (48.21) | |
| Early recurrence, n(%) | < 0.001 | |||
| No | 228 (89.06) | 190 (95.00) | 38 (67.86) | |
| Yes | 28 (10.94) | 10 (5.00) | 18 (32.14) | |
| HF, n(%) | 0.253 | |||
| No | 218 (85.16) | 173 (86.50) | 45 (80.36) | |
| Yes | 38 (14.84) | 27 (13.50) | 11 (19.64) | |
| Hypertension, n(%) | 0.940 | |||
| No | 136 (53.12) | 106 (53.00) | 30 (53.57) | |
| Yes | 120 (46.88) | 94 (47.00) | 26 (46.43) | |
| Diabetes, n(%) | 0.738 | |||
| No | 211 (82.42) | 164 (82.00) | 47 (83.93) | |
| Yes | 45 (17.58) | 36 (18.00) | 9 (16.07) | |
| Cerebral infarction/TIA, n(%) | 0.957 | |||
| No | 220 (85.94) | 172 (86.00) | 48 (85.71) | |
| Yes | 36 (14.06) | 28 (14.00) | 8 (14.29) | |
| CHD, n(%) | 0.619 | |||
| No | 190 (74.22) | 147 (73.50) | 43 (76.79) | |
| Yes | 66 (25.78) | 53 (26.50) | 13 (23.21) | |
| Type of AF, n(%) | 0.365 | |||
| Paroxysmal | 164 (64.06) | 131 (65.50) | 33 (58.93) | |
| Non-paroxysmal | 92 (35.94) | 69 (34.50) | 23 (41.07) | |
| AF duration, n(%) | 0.459 | |||
| < 6 years | 214 (83.59) | 169 (84.50) | 45 (80.36) | |
| ≥ 6 years | 42 (16.41) | 31 (15.50) | 11 (19.64) | |
| Cardiomyopathy, n(%) | 0.303 | |||
| No | 229 (89.45) | 181 (90.50) | 48 (85.71) | |
| Yes | 27 (10.55) | 19 (9.50) | 8 (14.29) | |
| Sleep apnea syndrome, n(%) | 0.771 | |||
| No | 242 (94.53) | 190 (95.00) | 52 (92.86) | |
| Yes | 14 (5.47) | 10 (5.00) | 4 (7.14) | |
| Renal insufficiency, n(%) | 0.009 | |||
| No | 233 (91.02) | 187 (93.50) | 46 (82.14) | |
| Yes | 23 (8.98) | 13 (6.50) | 10 (17.86) | |
| Hyperlipidemia, n(%) | 0.176 | |||
| No | 216 (84.38) | 172 (86.00) | 44 (78.57) | |
| Yes | 40 (15.62) | 28 (14.00) | 12 (21.43) | |
| COPD, n(%) | 1.000 | |||
| No | 254 (99.22) | 198 (99.00) | 56 (100.00) | |
| Yes | 2 (0.78) | 2 (1.00) | 0 (0.00) | |
| Valvular regurgitation, n(%) | 0.603 | |||
| No | 216 (84.38) | 170 (85.00) | 46 (82.14) | |
| Yes | 40 (15.62) | 30 (15.00) | 10 (17.86) | |
| Smoking history, n(%) | 0.872 | |||
| No | 121 (47.27) | 94 (47.00) | 27 (48.21) | |
| Yes | 135 (52.73) | 106 (53.00) | 29 (51.79) | |
| Drinking history, n(%) | 0.779 | |||
| No | 209 (81.64) | 164 (82.00) | 45 (80.36) | |
| Yes | 47 (18.36) | 36 (18.00) | 11 (19.64) | |
| SGLT2i, n(%) | 0.579 | |||
| No | 252 (98.44) | 196 (98.00) | 56 (100.00) | |
| Yes | 4 (1.56) | 4 (2.00) | 0 (0.00) | |
| Statin, n(%) | 0.925 | |||
| No | 134 (52.34) | 105 (52.50) | 29 (51.79) | |
| Yes | 122 (47.66) | 95 (47.50) | 27 (48.21) | |
| Beta-blocker, n(%) | 0.446 | |||
| No | 144 (56.25) | 110 (55.00) | 34 (60.71) | |
| Yes | 112 (43.75) | 90 (45.00) | 22 (39.29) | |
| Amiodarone, n(%) | 0.176 | |||
| No | 19 (7.42) | 12 (6.00) | 7 (12.50) | |
| Yes | 237 (92.58) | 188 (94.00) | 49 (87.50) | |
| Propafenone, n(%) | 0.802 | |||
| No | 222 (86.72) | 174 (87.00) | 48 (85.71) | |
| Yes | 34 (13.28) | 26 (13.00) | 8 (14.29) | |
| Rivaroxaban, n(%) | 0.578 | |||
| No | 150 (58.59) | 119 (59.50) | 31 (55.36) | |
| Yes | 106 (41.41) | 81 (40.50) | 25 (44.64) | |
| Dabigatran, n(%) | 0.755 | |||
| No | 160 (62.50) | 124 (62.00) | 36 (64.29) | |
| Yes | 96 (37.50) | 76 (38.00) | 20 (35.71) | |
| ACEI/ARB/ARNI, n(%) | 0.253 | |||
| No | 129 (50.39) | 97 (48.50) | 32 (57.14) | |
| Yes | 127 (49.61) | 103 (51.50) | 24 (42.86) |
No significant differences were observed in other demographic, clinical, or echocardiographic characteristics between the training and validation cohorts. A detailed summary of baseline characteristics for both cohorts is provided in Supplementary Table 1.
Variable selection
Candidate predictors were screened in the training cohort using two complementary feature selection methods: LASSO regression and the Boruta random forest algorithm.
The LASSO model was optimized using 10-fold cross-validation, yielding an optimal λ of 0.0537 that minimized the partial likelihood deviance[24]. Five variables with non-zero coefficients were identified, including intraoperative ECV, early recurrence, ACEI/ARB/ARNI therapy, left atrial diameter, and serum creatinine [Supplementary Figure 2].
In parallel, the Boruta algorithm identified early recurrence, AF duration, left atrial diameter, and serum creatinine as important predictors [Figure 2C and D]. These findings were largely consistent with the variables selected by the LASSO model.
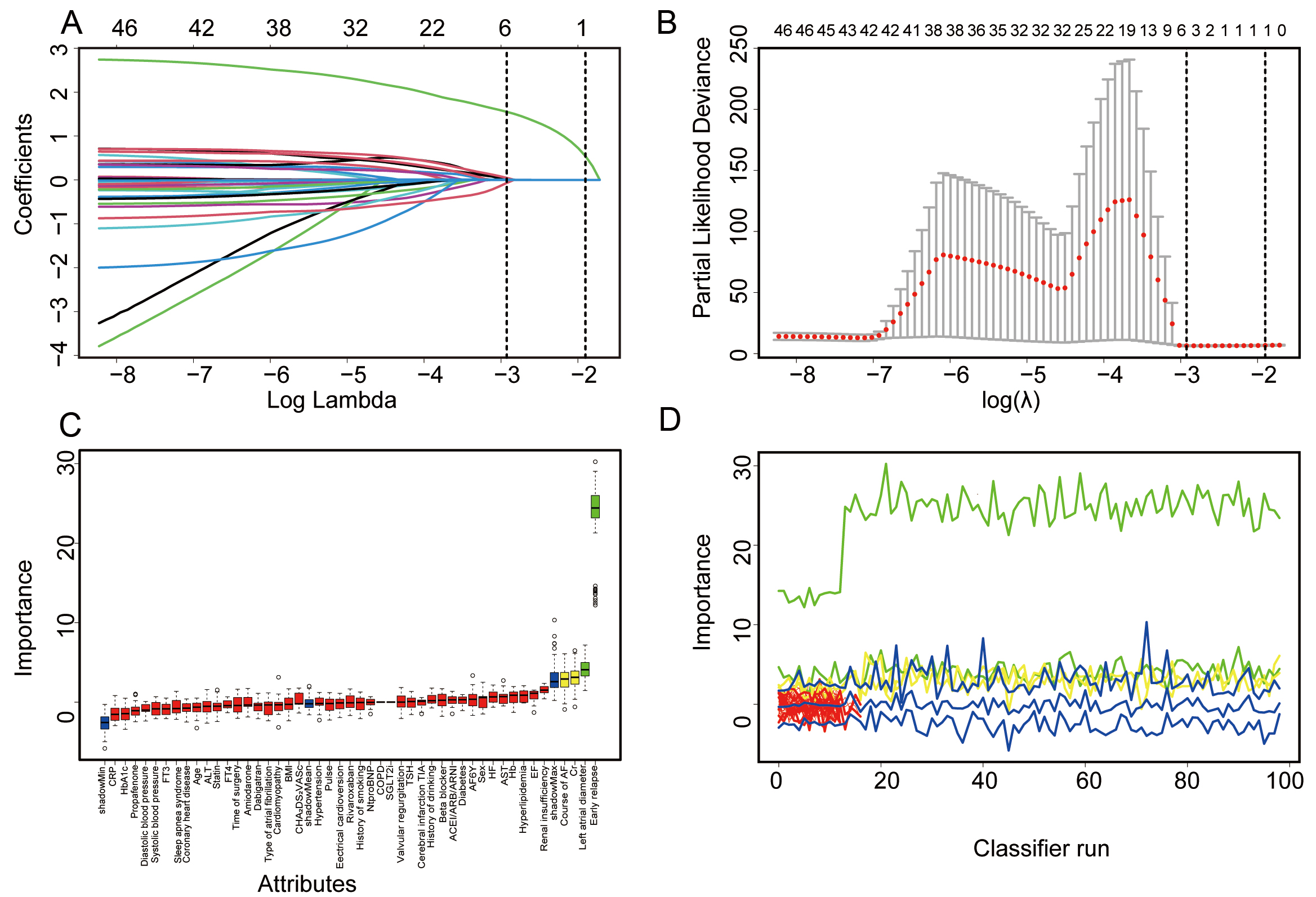
Figure 2. Feature selection using LASSO regression and the Boruta algorithm. (A) LASSO coefficient profiles plotted against log(λ); five variables with nonzero coefficients were retained at the optimal λ value. (B) Partial likelihood deviance (binomial deviance) curve used to identify the optimal λ; vertical dashed lines represent the minimum deviance and the 1-standard-error rule. (C) Boruta-based feature selection for predicting late recurrence. The y-axis shows Z-scores indicating feature importance; candidate predictors are listed on the x-axis. (D) Evolution of Z-scores across Boruta iterations. The x-axis shows iteration cycles; the y-axis indicates Z-score values. Color coding: blue = shadow features, green = confirmed predictors, red = rejected variables. Box plots display the range (min, mean, max) of Z-scores at each step.
Variables identified by either method were entered into a multivariable Cox proportional hazards model with backward stepwise selection [Table 2]. In the final model, six variables were retained: early recurrence (HR = 7.616, 95%CI: 4.124-14.062), left atrial diameter (HR = 1.684, 95%CI: 1.074-2.642), intraoperative ECV (HR = 1.423, 95%CI: 0.800-2.531), serum creatinine (HR = 1.018, 95%CI: 1.007-1.029), ACEI/ARB/ARNI therapy (HR = 0.426, 95%CI: 0.238-0.760), and AF duration (HR = 1.003, 95%CI: 0.999-1.006). Early recurrence was the strongest predictor of late AF recurrence, while ACEI/ARB/ARNI therapy was associated with a reduced risk.
Multivariate Cox regression analysis predicting late recurrence in patients with AF in training cohort
| Variable | β | Hazard ratio (95%CI) | P value |
| Early recurrence | 2.03 | 7.616 (4.124-14.062) | < 0.001 |
| Left atrial diameter | 0.521 | 1.684 (1.074-2.642) | 0.023 |
| ECV | 0.353 | 1.423 (0.8-2.531) | 0.229 |
| Cr | 0.018 | 1.018 (1.007-1.029) | 0.001 |
| ACEI/ARB/ARNI | -0.854 | 0.426 (0.238-0.76) | 0.004 |
| Course of AF | 0.003 | 1.003 (0.999-1.006) | 0.101 |
Construction of the nomogram
Based on the final multivariable Cox model, a nomogram was developed to estimate the probability of AF recurrence at 6, 12, and 18 months in the training cohort [Figure 3]. In the nomogram, early recurrence contributed the highest number of points, followed by left atrial diameter, ACEI/ARB/ARNI therapy, intraoperative ECV, serum creatinine, and AF duration.
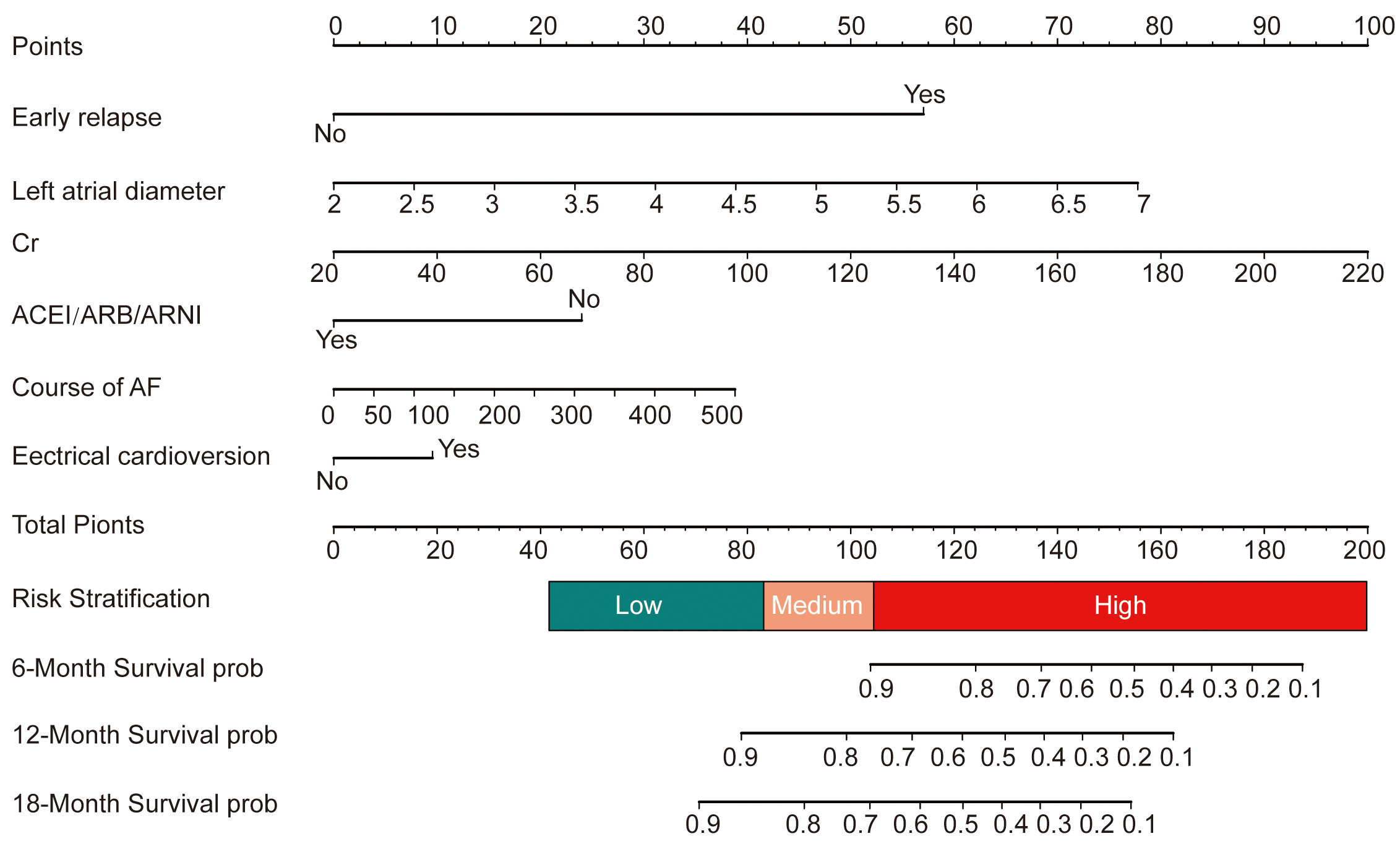
Figure 3. Nomogram for predicting recurrence rates at 6, 12, and 18 months.
Variance inflation factors (VIFs) for all predictors were close to 1, indicating minimal multicollinearity [Supplementary Table 2]. The proportional hazards assumption was assessed for each predictor and for the global model, with no significant violations detected (all P > 0.05) [Supplementary Figure 3]. These findings support the appropriateness of the Cox proportional hazards model for this analysis.
Evaluation of nomogram performance
Model performance was evaluated in terms of discrimination, calibration, and clinical usefulness[25]. The C-index was 0.776 (95%CI: 0.705-0.847) in the training cohort and 0.779 (95%CI: 0.699-0.859) in the validation cohort, indicating good discriminative ability and consistent performance across cohorts.
Internal validation was performed using nonparametric bootstrap resampling with 500 iterations to estimate optimism. In the training cohort, the apparent C-index was 0.776, with an estimated optimism of 0.007 and a standard error of 0.035. The bias-corrected C-index remained highly consistent with the apparent estimate. These results indicate minimal optimism and support the stability and robustness of the model.
Time-dependent AUCs at 6, 12, and 18 months were 0.869 (95%CI: 0.765-0.972), 0.810 (95%CI: 0.709-0.911), and 0.776 (95%CI: 0.662-0.890), respectively, in the training cohort. In the external validation cohort, the corresponding AUCs were 0.831 (95%CI: 0.689-0.973), 0.848 (95%CI: 0.743-0.953), and 0.789 (95%CI: 0.664-0.913) [Figure 4A and B]. These results indicate good and consistent discriminative performance across different time points and between cohorts.
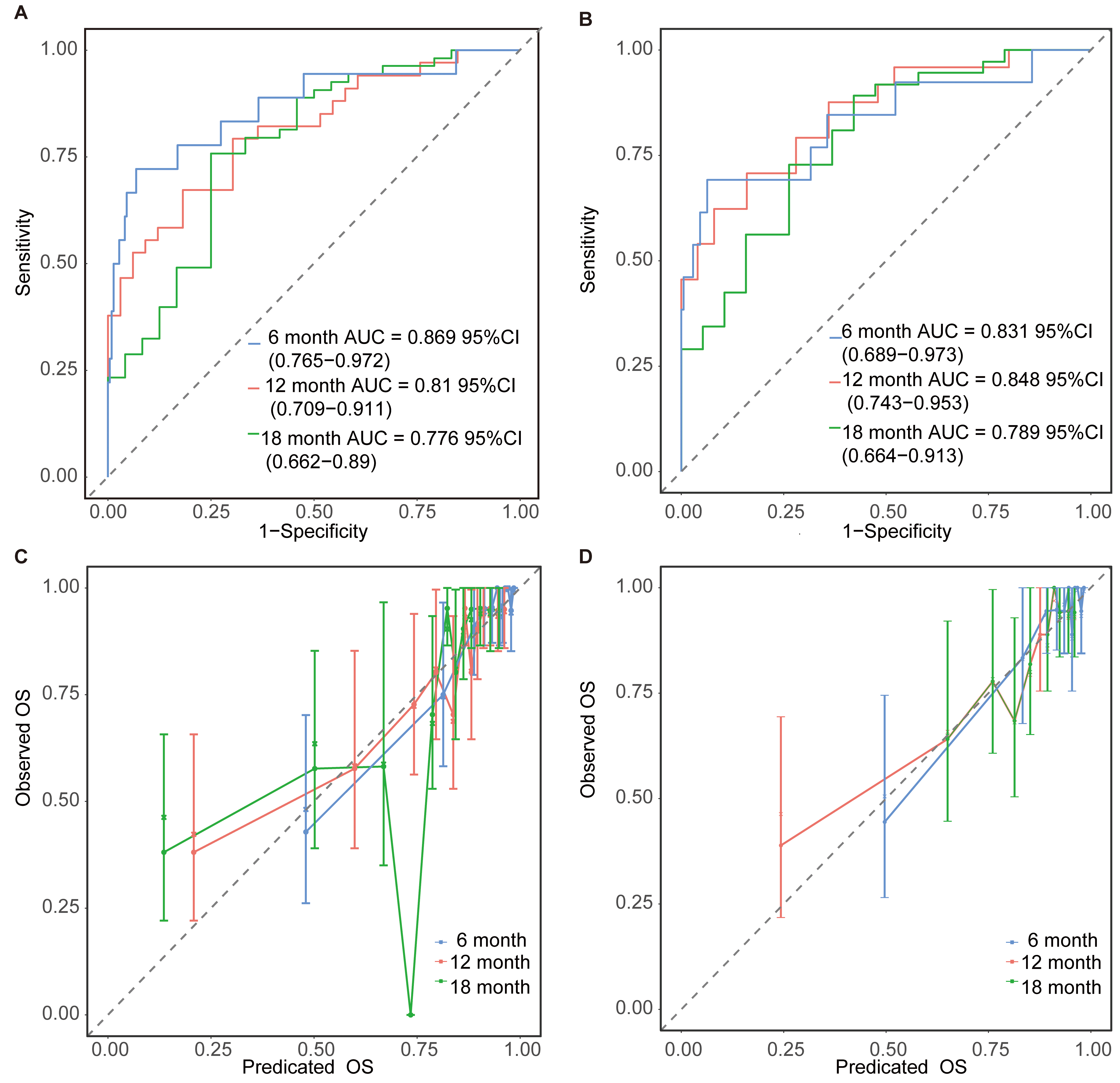
Figure 4. ROC curves of the nomogram for predicting 6-, 12-, and 18-month recurrence in the training cohort (A) and validation cohort (B). Calibration plots of the nomogram for predicting 6-, 12-, and 18-month recurrence in the training cohort (C) and validation cohort (D).
Calibration plots showed good agreement between predicted and observed recurrence probabilities at all evaluated time points [Figure 4C and D]. The calibration slope was 1.00 (95%CI: 0.75-1.25) in the training cohort and 0.99 (95%CI: 0.70-1.27) in the validation cohort, indicating no evidence of model overfitting. Calibration-in-the-large at 6, 12, and 18 months showed intercepts of 0.37 (95%CI: -0.09 to 0.84), 0.45 (95%CI: 0.10-0.81), and -0.20 (95%CI: -0.56 to 0.16), respectively, in the training cohort. In the validation cohort, the corresponding values were 0.36 (95%CI: -0.16 to 0.89), 0.41 (95%CI: 0.00-0.81), and -0.32 (95%CI: -0.73 to 0.10). Overall, calibration-in-the-large was close to zero, although a mild underestimation of risk was observed at 12 months in the training cohort. The calibration slope remained close to 1.0, and similar patterns were observed in the validation cohort, indicating good calibration and preserved model structure.
DCA demonstrated that the nomogram provided meaningful clinical benefit across a range of decision thresholds [Figure 5].
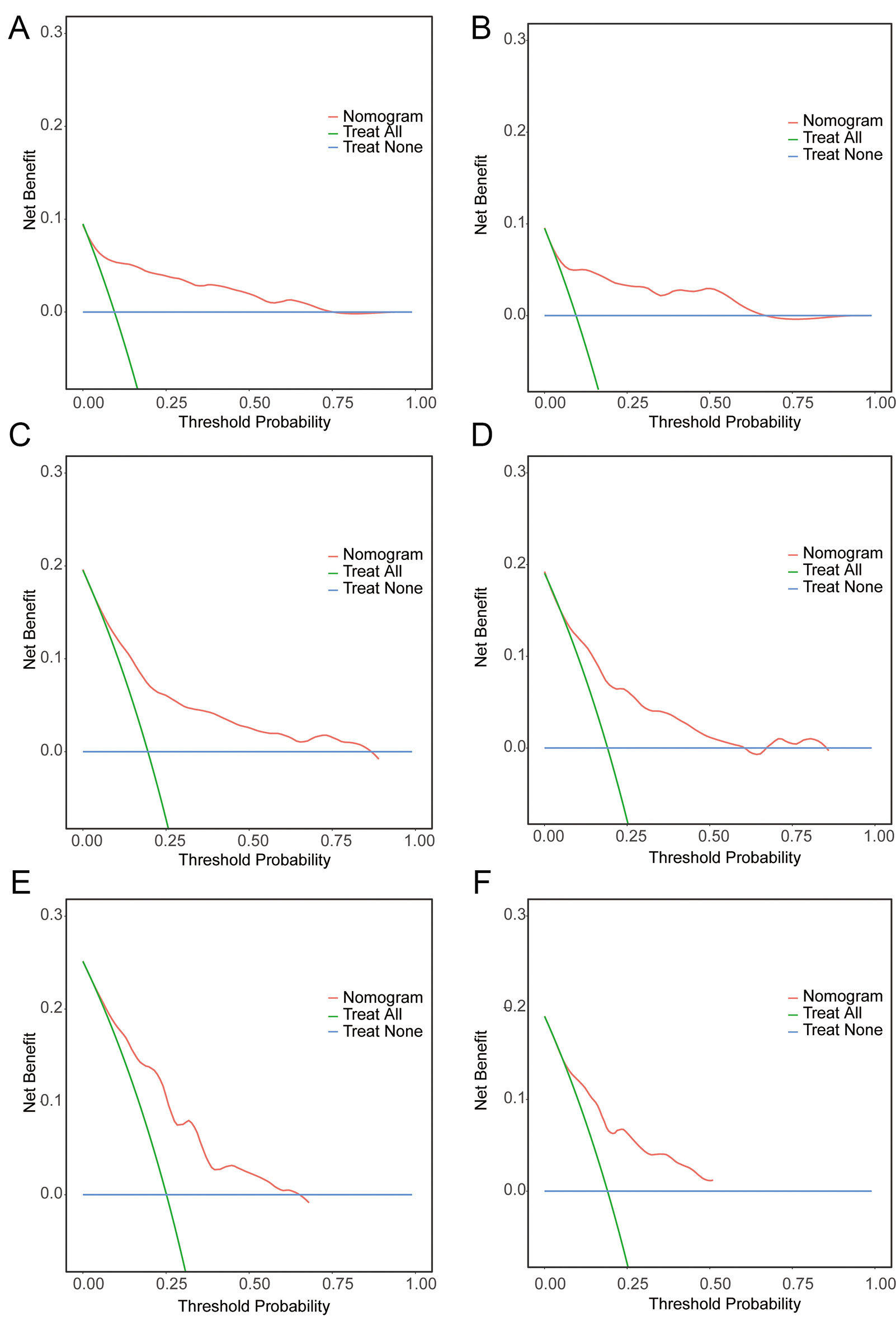
Figure 5. DCA curves show the net benefit, represented by a backslash with a negative slope, in the training (A-C) and validation (D-F) cohorts.
To further assess the incremental predictive value of early recurrence, a sensitivity analysis was performed by reconstructing the model without this variable. The reduced model showed a lower C-index of 0.683 (95%CI: 0.605-0.761), compared with 0.776 (95%CI: 0.705-0.847) for the full model. Time-dependent C-index and AUC analyses for both models are presented in Supplementary Figure 4, further confirming the additional discriminative contribution of early recurrence.
For comparative evaluation, the nomogram was assessed against the CAAP-AF and APPLE scores. As shown in Table 3, the nomogram demonstrated higher area under the receiver operating characteristic curve (AUROC) values and improved classification performance. Net reclassification improvement (NRI) and integrated discrimination improvement (IDI) analyses further confirmed the incremental predictive value of the nomogram over CAAP-AF (continuous NRI = 0.724; IDI = 0.159) and APPLE (continuous NRI = 0.623; IDI = 0.139) (all P < 0.05). Consistent findings were observed in decision curve analysis [Figure 6], indicating superior clinical utility of the nomogram.
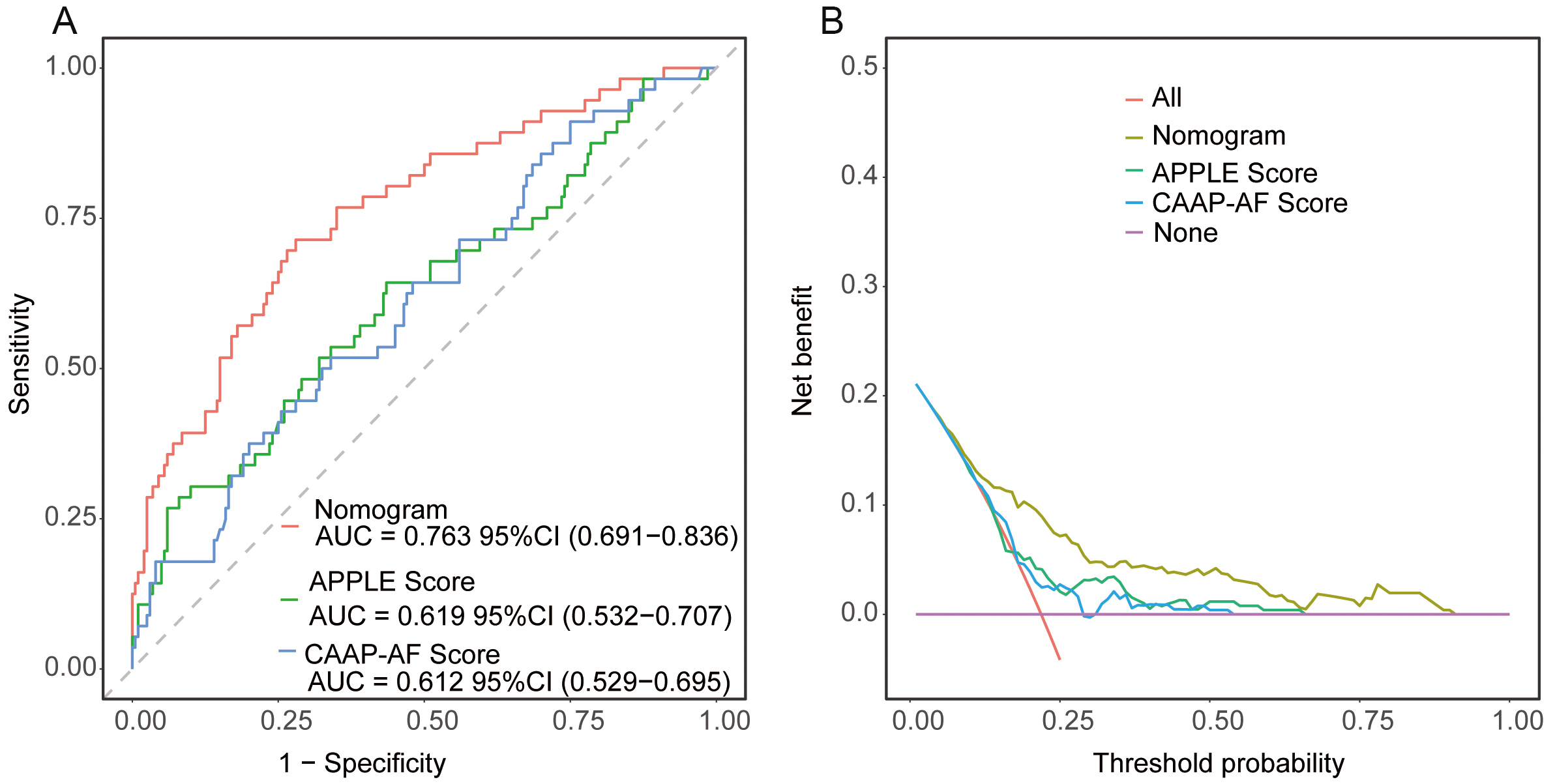
Figure 6. Receiver operating characteristic curves and DCA curves for the 3 models. (A) ROC curves of the training cohort for the 3 models. (B) DCA curves of the training cohort for the 3 models.
The performance of models to predict AF recurrence in the training cohort
| AUROC | Sensitivity | Specificity | Accuracy | F1 score | NRI-categorical | NRI-continuous | IDI | |
| CAAP-AF score | 0.612 | 0.518 | 0.660 | 0.629 | 0.379 | Ref | Ref | Ref |
| APPLE score | 0.619 | 0.643 | 0.565 | 0.582 | 0.402 | Ref | Ref | Ref |
| Nomogram | 0.763 | 0.714 | 0.720 | 0.719 | 0.526 | +0.238 vs. CAAP-AF; +0.202 vs. APPLE | +0.724 vs. CAAP-AF; +0.623 vs. APPLE | +0.159 vs. CAAP-AF; +0.139 vs. APPLE |
In addition, individualized 18-month recurrence-free probabilities were estimated based on three key predictors identified in the model: early AF recurrence, intra-procedural cardioversion, and left atrial diameter above the cohort median (4.3 cm). The corresponding stratified estimates are presented in Supplementary Table 3.
Based on nomogram-derived risk scores, patients were stratified into high- and low-risk groups using the median value as the cutoff. Kaplan-Meier analysis showed a clear and consistent separation in recurrence-free survival between the two groups in both the training and validation cohorts. Patients in the high-risk group had significantly worse outcomes than those in the low-risk group. The hazard ratios for recurrence-free survival were 0.22 (95%CI: 0.11-0.43) in the training cohort and 0.17 (95%CI: 0.07-0.40) in the validation cohort (log-rank P < 0.001 for both; Figure 7).
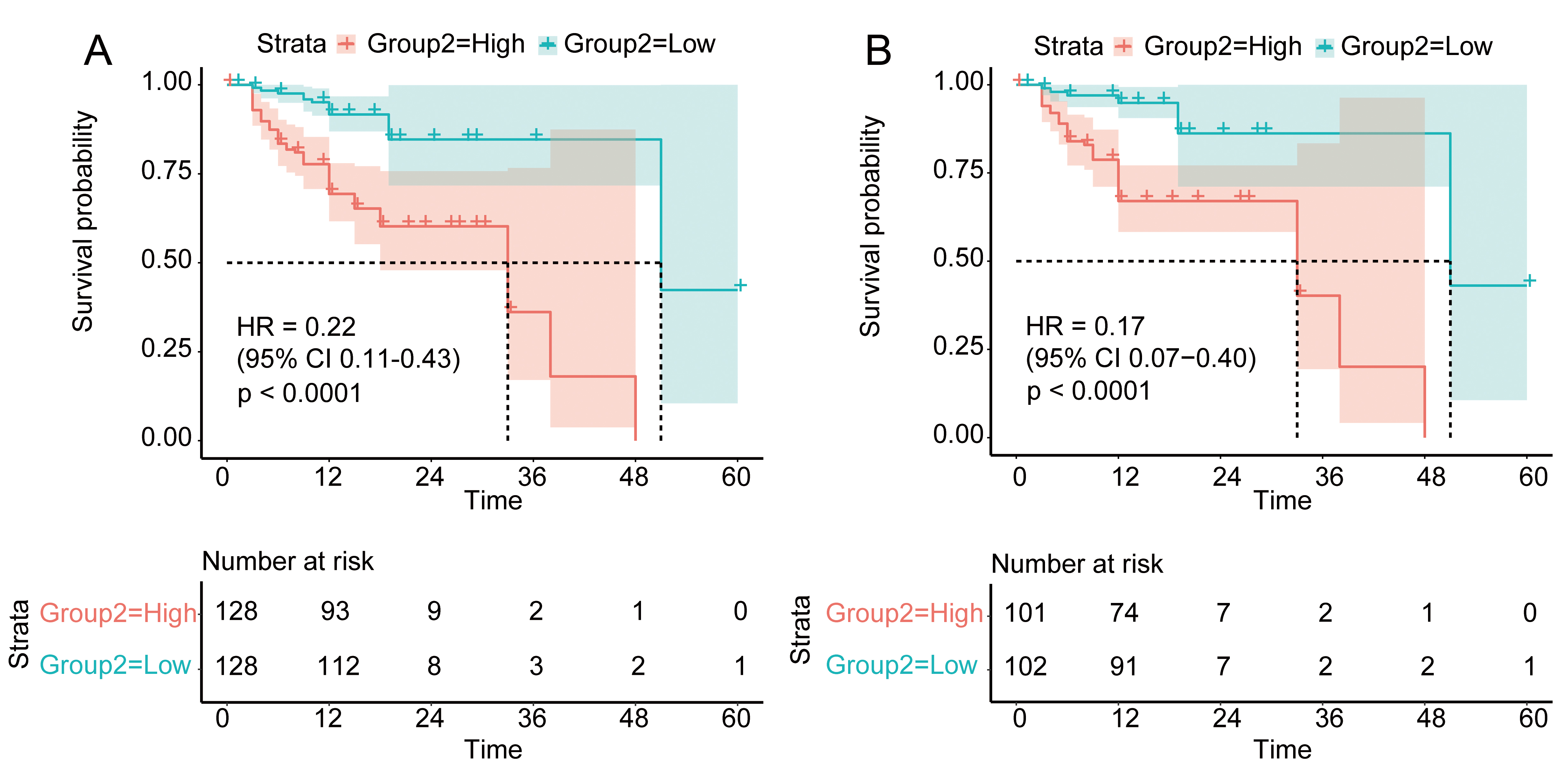
Figure 7. The nomogram distinguished the recurrence risk of AF patients in the training cohort (A) and the validation cohort (B).
DISCUSSION
Over the past decades, numerous studies have identified clinical factors associated with AF recurrence after catheter ablation, including left atrial size, AF type and duration, hypertension, and structural heart disease[26]. Based on these variables, several risk scores, such as CAAP-AF[11], APPLE[13], and ATLAS[10], have been developed to estimate recurrence risk before ablation. Although these tools have demonstrated clinical utility, their predictive performance varies across different populations and clinical settings[27]. Moreover, most existing scoring systems include a limited number of variables and may not fully account for procedural or post-procedural factors that influence long-term outcomes[28]. Therefore, further refinement and external validation of prediction models remain essential to improve individualized risk stratification after AF ablation.
This retrospective, two-center study developed and externally validated a nomogram to predict late AF recurrence following RFCA. The final prediction model incorporated six variables: early recurrence, intraoperative ECV, left atrial diameter, serum creatinine, ACEI/ARB/ARNI therapy, and AF duration.
By integrating clinical, laboratory, and procedural factors into a single framework, the nomogram provides individualized risk estimates in a visual and clinically practical format. Risk stratification based on the model may help identify patients at higher risk of recurrence, thereby supporting tailored follow-up and post-ablation management strategies.
Among the variables included in the model, early recurrence had the largest effect size (HR = 7.616), indicating a strong association with subsequent late AF recurrence. This finding aligns with previous studies suggesting that early recurrence during the post-ablation blanking period may reflect transient atrial inflammation, edema, or underlying substrate vulnerability that predisposes patients to future arrhythmia recurrence[29].
Large cohort studies have likewise identified early recurrence as a strong predictor of long-term outcomes. For instance, Stabile et al. reported that early recurrence during the post-ablation blanking period was associated with late recurrence following cryoablation[30].
Additionally, long-term follow-up studies by Njoku et al.[31] and Choi et al.[32] showed that markers of atrial remodeling, together with early recurrence, were associated with an increased risk of subsequent AF recurrence.
Although early recurrence occurs after the ablation procedure and is not a pre-procedural factor, identifying patients with early recurrence can help stratify those at particularly high risk for late recurrence. In this context, early recurrence may serve as a dynamic prognostic marker to guide closer monitoring and individualized post-ablation management.
Intraoperative ECV is typically performed when sinus rhythm is not restored spontaneously at the end of the ablation procedure. The need for ECV may reflect a lack of spontaneous cardioversion and could indicate a more advanced atrial substrate, incomplete substrate modification, or greater procedural complexity.
Although intraoperative ECV did not reach conventional statistical significance in the multivariable model, it was retained because variable selection was guided by overall model performance rather than individual P values. In prediction modeling, variables that are clinically plausible and provide incremental information can enhance overall prognostic discrimination, even if their independent association is modest.
Prior studies have shown that failure to restore sinus rhythm at discharge is associated with higher post-ablation recurrence rates. For instance, Henn et al.[33] identified absence of sinus rhythm at discharge, along with age, peripheral vascular disease, left atrial volume, and AF duration, as predictors of recurrence. In this context, intraoperative ECV should be considered a procedural marker of atrial vulnerability and substrate severity, rather than a direct causal determinant of late recurrence.
Left atrial enlargement is a well-established anatomical marker associated with AF recurrence[34]. In the present study, increased left atrial diameter was independently associated with a higher risk of recurrence (HR = 1.684), consistent with the concept of atrial structural remodeling. A larger atrial chamber may reflect a greater arrhythmogenic substrate burden and more advanced electrical remodeling, which could reduce long-term procedural durability[35].
Elevated serum creatinine was independently associated with AF recurrence (HR = 1.018), suggesting a potential link between renal dysfunction and post-ablation outcomes. Impaired renal function has been linked to increased atrial pressure, autonomic dysregulation, and systemic inflammation—factors that may create a pro-arrhythmic milieu and predispose patients to AF recurrence.
The use of renin-angiotensin system (RAS) inhibitors—including ACEIs, ARBs, and ARNIs—was associated with a lower risk of AF recurrence (HR = 0.426). These agents have been reported to attenuate atrial fibrosis and modulate RAS-mediated structural remodeling, potentially supporting the maintenance of sinus rhythm after ablation. In our cohort, patients not receiving these medications had higher recurrence rates, suggesting that RAS blockade may represent a modifiable factor in post-ablation management.
However, this observation reflects an association rather than a causal relationship. Given the retrospective study design, confounding by indication and residual confounding cannot be excluded, as patients prescribed RAS inhibitors may differ systematically from those not receiving them in baseline characteristics or comorbidities. Prospective randomized studies are needed to determine whether RAS blockade confers a direct protective effect against AF recurrence following ablation.
Lastly, longer AF duration showed a modest association with increased recurrence risk (HR = 1.003). This finding aligns with prior evidence suggesting that prolonged AF is associated with progressive electrical and structural remodeling, which may compromise long-term rhythm control[36]. Lin et al.[37] reported that earlier catheter ablation following AF diagnosis was associated with improved outcomes, particularly among patients with long-standing persistent AF. In that study, each additional month of delay from diagnosis to ablation was associated with a small incremental increase in recurrence risk. Taken together, AF duration may serve as a surrogate marker of cumulative atrial remodeling and procedural complexity, rather than a direct causal determinant of recurrence.
This study has several strengths. First, a structured variable selection strategy was applied, incorporating Boruta, LASSO regression, and multivariable Cox modeling. Internal and external validation procedures—including assessment of discrimination and calibration (calibration slope and calibration-in-the-large)—were conducted to reduce potential overfitting and evaluate model stability. Second, the model incorporated both clinical and procedural variables, including intraoperative ECV, which may reflect procedural complexity and atrial substrate characteristics. The inclusion of such variables extends beyond pre-ablation factors and provides a more comprehensive risk assessment framework. Third, external validation was performed in an independent cohort from a geographically distinct tertiary referral center. The two centers operate with independent clinical teams, procedural protocols, and follow-up infrastructures, providing a robust test of model transportability. Although baseline characteristics appeared broadly similar, external heterogeneity cannot be fully assessed from statistical comparisons of measured variables alone. Differences in referral pathways, peri-procedural management, operator expertise, local practice patterns, and healthcare delivery structures may introduce contextual variability. The consistent discrimination and calibration observed in the validation cohort supports the model’s applicability across institutional settings. Finally, the nomogram provides a practical visualization of individualized recurrence probabilities at 6, 12, and 18 months, which may assist clinicians in post-ablation risk stratification and follow-up planning.
Several limitations of this study warrant consideration. First, although this was a multicenter retrospective analysis, prospective studies are needed to further evaluate the generalizability and reproducibility of the model. Second, the follow-up duration was relatively limited (median 12 months; mean 12.82 ± 6.89 months), primarily reflecting short- to mid-term outcomes. Accordingly, the present model is applicable to predicting recurrence within 18 months after ablation. Longer follow-up would enable a more comprehensive assessment of sustained rhythm control and late recurrence, particularly beyond 2 years. Third, AF recurrence was assessed using standard 12-lead electrocardiograms and 24-h Holter monitoring. These methods may fail to detect asymptomatic or intermittent episodes, potentially underestimating the true recurrence rate. Emerging wearable rhythm monitoring technologies may improve detection in future studies.
Fourth, this study focused exclusively on AF recurrence as the primary endpoint. Other clinically meaningful outcomes, such as all-cause mortality or major adverse cardiovascular events, were not evaluated, limiting the broader prognostic assessment. Fifth, although ACEI/ARB/ARNI use was associated with a lower risk of late recurrence, detailed data on medication dose, duration, and adherence were not consistently available. Moreover, although baseline left ventricular ejection fraction did not differ significantly between users and non-users, differences in hypertension prevalence and other clinical characteristics may have introduced residual confounding. Therefore, the observed association should be interpreted cautiously and does not constitute definitive evidence of a causal protective effect. Sixth, the number of outcome events in both cohorts was modest. Although the final model satisfied the conventional “10 events per predictor” criterion, limited event counts may still increase the risk of optimism-biased estimates and coefficient instability. Finally, the use of multiple feature-selection approaches (Boruta, LASSO, and backward Cox regression) may raise concerns regarding potential overfitting. Although internal validation via bootstrapping and external validation in an independent cohort demonstrated stable performance, these procedures can only partially mitigate optimism. Further validation in larger and more diverse populations is warranted.
Conclusion
In this two-center retrospective study, we developed and externally validated a nomogram to estimate the risk of late AF recurrence following RFCA. The model demonstrated good discrimination and consistent performance in an independent validation cohort. By integrating clinical and procedural factors into an individualized risk prediction framework, the nomogram may aid post-ablation risk stratification and follow-up planning. Further prospective studies are warranted to confirm its generalizability in broader clinical settings.
DECLARATIONS
Acknowledgements
We thank the people and specialists who assisted us in all steps of this study.
Authors’ contribution
Had full access to all of the data in the study: Li Y, Liu X
Concept and design: Li Y, Zhao C
Acquisition, analysis, or interpretation of data: Li Y, Liu X, Chen Y, Sun R, Li H, Li Q
Drafting of the manuscript: Li Y
Critical review of the manuscript for important intellectual content, administrative, technical, or material support: Zhou L, Zhao C
Statistical analysis: Li Y, Liu X, Wang X
Obtained funding: Zhao C
Supervision: Zhou L, Zhao C, Wang F
All authors participated in manuscript revision and approved the final version.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
AI and AI-assisted tools statement
Not applicable.
Financial support and sponsorship
None.
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethics approval and consent to participate
The study was approved by the Ethics Committees of Tongji Hospital, Huazhong University of Science and Technology (Approval No. TJ-IRB202404056), and Second Hospital of Lanzhou University (2024A-1246). Given the retrospective nature of the study, the Ethics Committee waived the requirement for obtaining informed consent, in accordance with the Declaration of Helsinki and relevant national regulations. The data used in this study were anonymized, and no individual patient information is disclosed in this manuscript. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
Supplementary Materials
REFERENCES
1. Lippi G, Sanchis-Gomar F, Cervellin G. Global epidemiology of atrial fibrillation: an increasing epidemic and public health challenge. Int J Stroke. 2020;16:217-21.
2. Joglar JA, Chung MK, Armbruster AL, et al. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2024;149:e1-156.
3. Al-khatib SM, Benjamin EJ, Buxton AE, et al. Research needs and priorities for catheter ablation of atrial fibrillation: a report from a national heart, lung, and blood institute virtual workshop. Circulation. 2020;141:482-92.
4. Reddy VY, Gerstenfeld EP, Natale A, et al. Pulsed field or conventional thermal ablation for paroxysmal atrial fibrillation. N Engl J Med. 2023;389:1660-71.
5. Schnabel RB, Marinelli EA, Arbelo E, et al. Early diagnosis and better rhythm management to improve outcomes in patients with atrial fibrillation: the 8th AFNET/EHRA consensus conference. EP Europace. 2023;25:6-27.
6. Benali K, Macle L, Haïssaguerre M, et al. Impact of catheter ablation of atrial fibrillation on disease progression. JACC Clin Electrophysiol. 2025;11:421-35.
7. Modin D, Claggett B, Gislason G, et al. Catheter ablation for atrial fibrillation is associated with lower incidence of heart failure and death. EP Europace. 2020;22:74-83.
8. Cappato R, Calkins H, Chen S, et al. Updated worldwide survey on the methods, efficacy, and safety of catheter ablation for human atrial fibrillation. Circ Arrhythm Electrophysiol. 2010;3:32-8.
9. Luik A, Kunzmann K, Hörmann P, et al. Cryoballoon vs. open irrigated radiofrequency ablation for paroxysmal atrial fibrillation: long-term FreezeAF outcomes. BMC Cardiovasc Disord. 2017;17:135.
10. Kornej J, Hindricks G, Shoemaker MB, et al. The APPLE score: a novel and simple score for the prediction of rhythm outcomes after catheter ablation of atrial fibrillation. Clin Res Cardiol. 2015;104:871-6.
11. Winkle RA, Jarman JW, Mead RH, et al. Predicting atrial fibrillation ablation outcome: the CAAP-AF score. Heart Rhythm. 2016;13:2119-25.
12. Mujović N, Marinković M, Marković N, Shantsila A, Lip GYH, Potpara TS. Prediction of very late arrhythmia recurrence after radiofrequency catheter ablation of atrial fibrillation: the MB-LATER clinical score. Sci Rep. 2017;7:40828.
13. Mesquita J, Ferreira AM, Cavaco D, et al. Development and validation of a risk score for predicting atrial fibrillation recurrence after a first catheter ablation procedure - ATLAS score. EP Europace. 2018;20:f428-35.
14. Marrouche NF, Wilber D, Hindricks G, et al. Association of atrial tissue fibrosis identified by delayed enhancement MRI and atrial fibrillation catheter ablation: the DECAAF study. JAMA. 2014;311:498.
15. Collins GS, Reitsma JB, Altman DG, Moons KGM. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): the TRIPOD statement. BMJ. 2015;350:g7594.
16. Zhang H, Zheng L, Yang Z, et al. Development and validation of prognostic models for bleeding and ischemia in elderly patients with comorbid acute coronary syndrome and atrial fibrillation. J Am Heart Assoc. 2024;13:e035086.
17. Hindricks G, Potpara T, Dagres N, et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The task force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42:373-498.
18. Bergonti M, Ascione C, Marcon L, et al. Left ventricular functional recovery after atrial fibrillation catheter ablation in heart failure: a prediction model. Eur Heart J. 2023;44:3327-35.
19. Guan C, Gong A, Zhao Y, et al. Interpretable machine learning model for new-onset atrial fibrillation prediction in critically ill patients: a multi-center study. Crit Care. 2024;28:349.
20. Balachandran VP, Gonen M, Smith JJ, Dematteo RP. Nomograms in oncology: more than meets the eye. Lancet Oncol. 2015;16:e173-80.
22. Yang J, Li Y, Liu Q, et al. Brief introduction of medical database and data mining technology in big data era. J Evid Based Med. 2020;13:57-69.
23. Stekhoven DJ, Bühlmann P. MissForest—non-parametric missing value imputation for mixed-type data. Bioinformatics. 2012;28:112-8.
24. Hu J, Wang Y, Tong X, Yang T. When to consider logistic LASSO regression in multivariate analysis? Eur J Surg Oncol. 2021;47:2206.
25. Wang J, Wang Y, Duan S, et al. Multimodal data-driven prognostic model for predicting long‐term prognosis in patients with ischemic cardiomyopathy and heart failure with preserved ejection fraction after coronary artery bypass grafting: a multicenter cohort study. J Am Heart Assoc. 2024;13:e036970.
26. Winkle RA, Mead RH, Engel G, Patrawala RA. Long-term results of atrial fibrillation ablation: the importance of all initial ablation failures undergoing a repeat ablation. Am Heart J. 2011;162:193-200.
27. Soffer S, Klang E, Barash Y, Grossman E, Zimlichman E. Predicting in-hospital mortality at admission to the medical ward: a big-data machine learning model. Am J Med. 2021;134:227-34.e4.
28. Ma G, Zou C, Zhang Z, Zhang L, Zhang J. A novel nomogram for predicting the recurrence of atrial fibrillation in patients treated with first-time radiofrequency catheter ablation for atrial fibrillation. Front Cardiovasc Med. 2024;11:1397287.
29. Calkins H, Hindricks G, Cappato R, et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. EP Europace. 2018;20:e1-160.
30. Stabile G, Iacopino S, Verlato R, et al. Predictive role of early recurrence of atrial fibrillation after cryoballoon ablation. EP Europace. 2020;22:1798-804.
31. Njoku A, Kannabhiran M, Arora R, et al. Left atrial volume predicts atrial fibrillation recurrence after radiofrequency ablation: a meta-analysis. EP Europace. 2018;20:33-42.
32. Choi SH, Yu HT, Kim D, et al. Late recurrence of atrial fibrillation 5 years after catheter ablation: predictors and outcome. EP Europace. 2023;25:euad113.
33. Henn MC, Lancaster TS, Miller JR, et al. Late outcomes after the Cox maze IV procedure for atrial fibrillation. J Thorac Cardiovasc Surg. 2015;150:1168-78.e2.
34. Luong C, Thompson DJ, Bennett M, et al. Right atrial volume is superior to left atrial volume for prediction of atrial fibrillation recurrence after direct current cardioversion. Can J Cardiol. 2015;31:29-35.
35. Takagi T, Nakamura K, Asami M, et al. Impact of right atrial structural remodeling on recurrence after ablation for atrial fibrillation. J Arrhythm. 2021;37:597-606.
36. Bisbal F, Alarcón F, Ferrero‐de‐Loma‐Osorio A, et al. Diagnosis‐to‐ablation time in atrial fibrillation: a modifiable factor relevant to clinical outcome. J Cardiovasc Electrophysiol. 2019;30:1483-90.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Special Topic
Copyright

Data & Comments
Data
0











Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].